Article Text

Abstract
Aims Assessment of hormone receptor expression is part of routine examination of every breast cancer. In this study, we report the characterisation of a novel rabbit monoclonal antibody, clone EP1, directed against oestrogen receptor (ER) α. Additionally, its immunohistochemical performance characteristics in archival tissues are evaluated in normal tissues and two distinct cohorts of breast cancer patients.
Methods Comparative analyses between EP1 and the anti-ERα component of the ER/PR pharmDx kit (cocktail of mouse monoclonal antibody clones 1D5 and ER-2-123) and between EP1 and another commercially available rabbit monoclonal antibody, clone SP1, are described.
Results Clone EP1 specifically detects nuclear ER in all tissues examined; cytoplasmic staining was not observed. The analysis shows a high degree of concordance (∼95%) between EP1 and both the ERα component of the Dako ER/PR pharmDx kit and Ventana clone SP1. However, the use of EP1 antibody together with Dako EnVision FLEX detection system resulted in a stronger staining intensity as compared with SP1 antibody using the Ventana ultraView DAB detection system resulting in better ‘ease of use.’
Conclusions The use of EPI can result in better interpretation of the results of the ER analysis.
- Antibodies
- Breast Cancer
- Immunohistochemistry
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
The oestrogen receptor (ER) is a regulator of normal breast development and function. It also plays an important role in the development and progression of breast cancer, with approximately 80% of invasive breast cancers expressing ER. In the clinical setting, ER-positive patients with both metastatic and nonmetastatic disease have been shown to respond to hormonal therapies.1–5
As ER status is a critically important variable for prediction of response to hormonal therapies, a great deal of attention has been focused on the laboratory methods that are employed to assess ER expression. Immunohistochemistry (IHC) has been a well-accepted technique for the detection of ER in formalin-fixed, paraffin-embedded (FFPE) tissues of breast cancer specimens for the last few decades. This technique is preferred by pathologists because it also enables the simultaneous evaluation of morphologic characteristics.6 ,7 With the general adoption of this method, there has been particular emphasis on identifying new ER antibodies for use in IHC with appropriate sensitivity and specificity, and supported by clinical and technical validation of their performance. These efforts have led to the standardisation of these ER IHC assays and formulation of specific guidelines for their use and interpretation.8–11
In recent years, a number of significant improvements have been made to IHC methods. These include the introduction of polymer-based detection methods that improve the quality of staining by decreasing the non-specific binding of endogenous biotin and enhanced sensitivity.12 At the same time, advances in the generation and production of primary antibodies have resulted in the replacement of rabbit polyclonal antibodies by mouse monoclonal and, most recently, by rabbit monoclonal antibodies.13 During the past few years, the use of rabbit monoclonal antibodies in ER IHC assays has been implemented in an effort to continuously improve assay quality by introducing new highly sensitive, specific and robust reagents. These ongoing efforts have resulted in the rigorous evaluation of a novel rabbit monoclonal antibody, clone EP1.
In this study, we describe the characterisation of this antibody and demonstrate its utility in detecting ERα in breast cancer tissue specimens. The performance characteristics of this rabbit antibody were compared with the anti-ERα component of the ER/PR pharmDx kit (Dako) (cocktail of mouse monoclonal antibody clones 1D5 and ER-2-123) and with another commercially available rabbit monoclonal antibody to ERα, clone SP1 (Ventana).
Materials and methods
Epitope mapping
In order to identify the epitope of human ERα to which monoclonal rabbit anti-ERα, clone EP1 binds, a large number of overlapping 15-mer peptides were synthesised, covering an amino acid sequence corresponding to 1–300 of the human protein (UniProt ID: P03372), which is equal to the recombinant protein fragment used for generating the EP1 clone. Binding of the antibody to each linear peptide was tested in a PEPSCAN-based ELISA.14 In brief, the 455-well miniPEPSCAN card, containing the covalently linked peptides, was incubated with the ERα antibody, clone EP1 (1 µg/mL). After washing, the wells were incubated with peroxidase-conjugated antirabbit antibody at a dilution of 1/1000 for 1 h at 25°C. The wells were then repeatedly washed, and a peroxidase substrate was added. After 1 h, the colour development of the ELISA was quantified with a charge-coupled device camera and an image-processing system.
IHC protocols and reagents
Tissue pretreatment and IHC staining were performed using the protocols, reagents and instrumentation platforms shown in table 1.
Protocols, reagents, and instrumentation used in the analysis
Specimens
Specimens for the studies were procured and used as shown in table 2. Some of the tissue samples from the Dako Tissue Bank were provided by the Cooperative Human Tissue Network, which is funded by the National Cancer Institute. For the concordance testing between EP1 and the ER component of the pharmDx kit, both ER positive and negative specimens were used. For the comparative analysis between EP1 and SP1, two different sets of tissue microarrays (TMAs) were used. The first set consisted of 200 ER+ cases with known Oncotype DX recurrence scores, and the second set was generated from a large series of cases (n=400) with known long-term outcomes. Multiples of 1 mm cores were used to generate the TMA. The latter TMA was generated from patients who had received adjuvant hormonal and chemotherapy.
Details of the specimens used in the study and the source from where they were obtained
Scoring
The data captured for the analytical specificity study on 30 normal tissue types included cell type, staining intensity (0–3 scale), percentage of positively stained cells and staining pattern (nuclear, cytoplasmic or membranous).
For scoring the results of the EP1 and the ERα component of the ER/PR pharmDx Kit concordance study, nuclear staining intensity and proportion of positive tumour cells were recorded and were combined to formulate a diagnostic score (Allred score) for the ER pharmDx results. Cutoff for positivity was according to the Allred score for the ER pharmDx and 1% for EP1.8 ,15
For the comparative analysis between clones EP1 and SP1, both Allred and H-score systems were used. The TMAs were analysed in a blinded fashion by two pathologists using the ASCO/CAP 1% cutoff for positivity, and differences in scores were resolved by consensus achieved through simultaneous viewing using a dual-headed microscope.
Statistical analysis
Graph pad programme was used to perform χ2 test analysis to observe correlations between the different parameters. Additionally, paired t test was performed to analyse the correlations between H-scores of SP1 and EP1 expression. κ analysis was performed to assess the degree of agreement between the two reagents.
Results
Epitope mapping
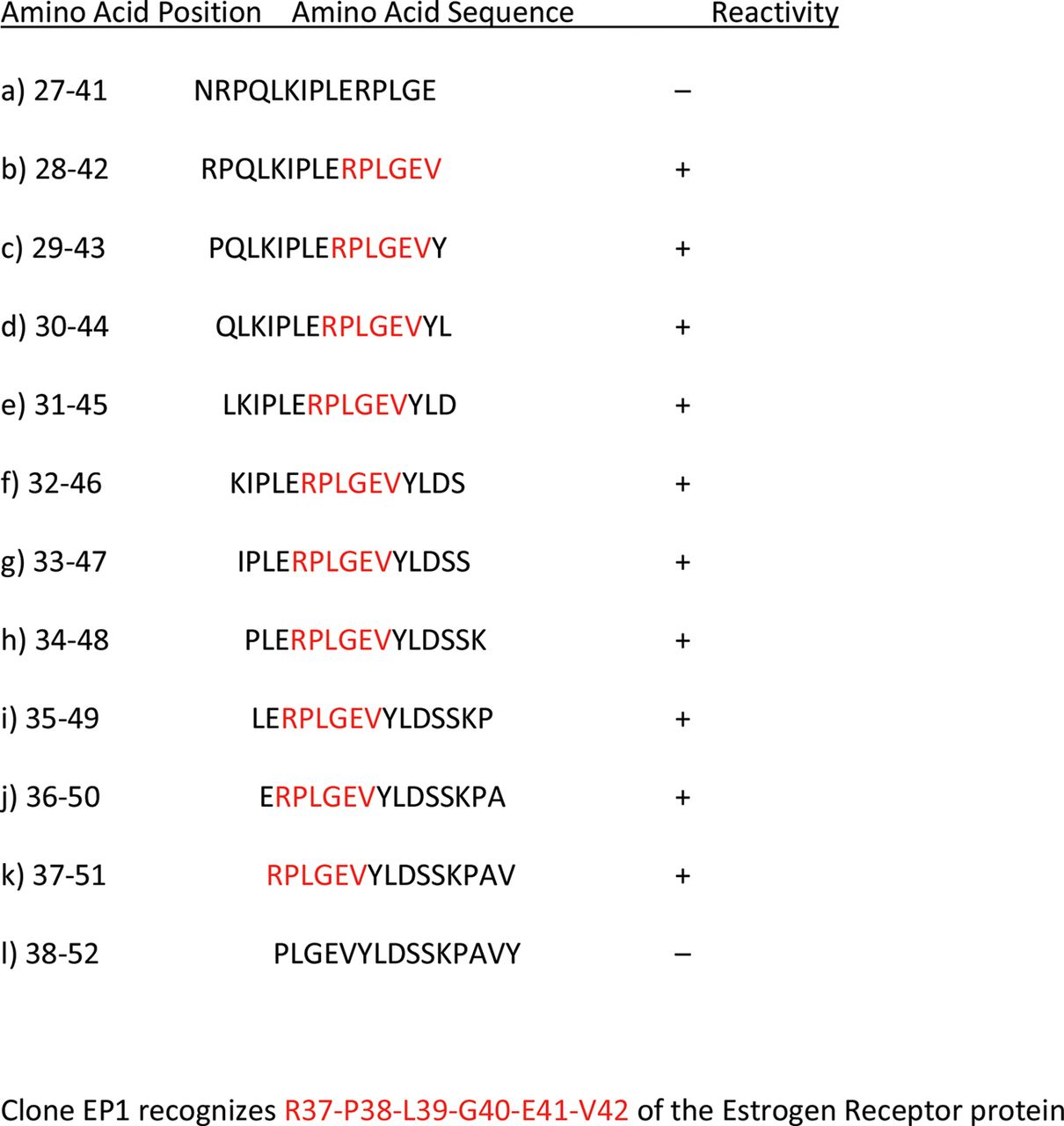
The presumptive epitope of human ERα that is recognised by clone EP1 was identified by assessing the binding of the antibody to a series of overlapping 15-mer peptides that spanned the amino acid sequence of the human protein. As shown in figure 1, the results of these epitope mapping studies clearly indicate that rabbit monoclonal antibody to ERα, clone EP1 recognises the amino acid sequence RPLGEV, which corresponds to amino acid residues 37–42 of human ERα (figure 1). This linear sequence is unique to the α form of the ER protein, and is located in the unstructured, N-terminal A/B domain (AF1).

Summary of epitope mapping results, antioestrogen receptor α, clone EP1.
Immunohistochemical staining of normal tissues using clone EP1
The specificity of clone EP1 was evaluated by examining the immunoreactivity pattern on a set of 90 (89 evaluable) FFPE normal tissue specimens composed of three patient cases from 30 different tissue types. When tested with these normal tissues, EP1 demonstrated nuclear positivity only in tissue types known to express ERα. These included epithelial cells and/or stromal cells from breast, cervix, oesophagus, ovary, prostate, tonsil and uterus.
Comparison of clone EP1 with the ERα component of the ER/PR pharmDx kit
As recommended in the current ASCO/CAP guidelines, a concordance study was performed to compare the monoclonal rabbit anti-ERα, clone EP1 with the anti-ERα component of the clinically validated ER/PR pharmDx kit as the predicate device. As shown in table 3 and figure 2, the staining results obtained on breast carcinoma specimens with clone EP1 were found to be highly concordant with those produced by the ERα component of the ER/PR pharmDx kit. Among the 314 cases analysed (table 3), 183 cases were found to be positive with both antibody assays, and 119 cases were found to be negative. There were 10 cases that were scored as negative with ERα pharmDx kit, but positive with clone EP1. Two cases were scored as positive with the predicate test, but negative with clone EP1. Values for the positive, negative and overall percent agreement were 98.9%, 92.2% and 96.2%, respectively.
Concordance of clone EP1 and the ERα component of the ER/PR pharmDx kit

Comparison of rabbit monoclonal antibody EP1 with mouse monoclonal oestrogen receptor α (ERα) component of the ER/PR pharmDx kit. Matched images from cases showing low and high expression of pharmDx and EP1 are demonstrated in these panels.
Comparison studies between clones EP1 and SP1
Following the demonstration of concordance with the ER/PR pharmDx Kit, clone EP1 was also tested on two different TMAs containing breast cancer tissues (Oncotype DX TMA and a TMA with long-term follow-up), and the IHC staining results were compared with those produced by rabbit monoclonal anti-ERα, clone SP1 (figure 3).

Comparison of clone EP1 performed using Dako reagents and kits with SP1 using Ventana BenchMark reagents and kits. Representative images of SP1 and matched EP1 expression in breast tumours are shown in these panels.
Oncotype DX TMA
Staining results for both clones EP1 and SP1 were assessed on 311 breast cancer cores, representing 176 unique cases in the Oncotype DX ER-positive TMA. Tables 4 and 5 summarise the positive and negative comparisons by cores (311 cores; table 4) and by cases (176 cases; table 5). Both antibodies identified 277 (89.1%) cores as positive and five (1.6%) cores as negative. Seventeen (5.5%) cores were characterised as positive by SP1 alone and 12 (3.9%) cores as positive by EP1 alone. When the same analysis was performed by cases, 165 (93.8%) cases were characterised as positive by both antibodies and two (1.1%) cases as negative. Five (2.8%) cases were classified as positive by SP1 alone and four (2.3%) cases by EP1 alone. For the positive cases, the distribution of the intensity and percentages (proportion of positive staining cells) by cores and cases is detailed in online supplementary tables S1 and S2. Both antibodies showed a strong correlation with ERα mRNA levels in the Oncotype DX assay (figure 4). Correlation of SP1 (Log2) and EP1 (Log2) with ERα mRNA levels were 0.44 (p<0.0001) and 0.37 (p<0.0001), respectively.
Comparison of clone EP1 and the SP1 in the Oncotype DX ER+ TMA set by cores
Comparison of clone EP1 and the SP1 in the Oncotype DX ER+ TMA set by cases

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of clones EP1 and SP1 with oestrogen receptor α score from Oncotype DX assay. The dotted line at 6.5 units indicates the cutoff for positivity.
In brief, when compared with SP1, EP1 stained a greater number of cores and cases with a staining intensity of 3+ (185 vs 139, χ2 test p=0.0003; 114 vs 91, p=0.0173), and a nearly identical number of cores and cases with greater than 10% of tumour cell positivity (281 vs 284; 167 vs 165), with overall a similar number of negative cases (22 vs 17; 7 vs 6). Paired t test was performed between the H-score for EP1 (Log2) and SP1 (Log2), the mean difference was 0.147 (SD (diff)=0.598; p=0.0059; 95% CI (0.0431 to 0.2507).
TMA with long-term follow-up
In the long-term follow-up TMA, EP1, and SP1 immunostaining was assessed in 617 cores representing 390 cases. Tables 6 and 7 show the positive and negative comparisons by cores (617 cores; table 6), and by cases (390 cases; table 7). Both antibodies identified 416 (67.4%) cores as positive and 173 (28.0%) cases as negative. Six (1.0%) cores were characterised as positive by SP1 alone and 22 (3.6%) cores as positive by EP1 alone. When the same analysis was performed by cases, 284 (73.0%) cases were characterised as positive by both antibodies, and 93 (23.9%) cases as negative. Four (1.0%) cases were classified as positive by SP1 alone and nine (2.3%) cases by EP1 alone. The distribution of the intensity and percentages (proportion of positively staining cells) by cores and cases is detailed in online supplementary tables S3 and S4. Survival analysis was not performed as the two antibodies detected similar numbers of positive cases, and the dataset was considered too small for doing survival analysis. Additionally, all patients in the long-term follow-up cohort had received adjuvant chemotherapy.
Comparison of clone EP1 and the SP1 in the long-term follow-up TMA set by cores
Comparison of clone EP1 and the SP1 in the long-term follow-up TMA set by cases
Briefly, when EP1 was compared with SP1, EP1 was observed to immunostain a larger number of cores and cases with a staining intensity of 3+ (186 vs 111, χ2 test p=0.0001; 132 vs 84, p=0.0002) and a similar number of cases with greater than 10% tumour cell staining (391 vs 379; 268 vs 259), with an overall smaller number of negative cases (179 vs 195; 97 vs 102). However, the differences were not statistically significant.
Discussion
Accurate assessment of ER status is critical to ensure that breast cancer patients receive appropriate therapy. IHC is currently the most commonly used method for determining ER status because of its relatively low cost, its general applicability to routinely processed tissue samples, and importantly, its utility in evaluating small cancers and ensuring that only invasive tumour cells are assessed.9 Because it is especially important to minimise false-negative and false-positive test results, guidance has been provided for analytical (technical) validation procedures, and recommendations have been made for ER testing methods and test interpretation.9 ,10
Previously, the mouse monoclonal antibody, clone 1D5, had been one of the most routinely used antibodies for the detection of ERα in FFPE tissue. More recently, the clinically validated ER/PR pharmDx kit using a mouse monoclonal antibody cocktail has been introduced. The continued need to improve reagent quality through generation of highly sensitive, specific and robust reagents led to the development of a new rabbit monoclonal antihuman ERα, designated clone EP1. In this manuscript, we describe the specificity and sensitivity of this novel antibody and demonstrate its utility in detecting ERα in FFPE breast cancer tissues. In keeping with recommended practices, the performance characteristics of EP1 were compared with those of other anti-ER antibodies, particularly to the predicate ERα component of the ER/PR pharmDx kit and another rabbit monoclonal antibody, clone SP1.
The specificity of this new antibody was established by epitope mapping and an assessment of the IHC staining of normal tissues. Epitope mapping clearly demonstrated that clone EP1 recognises an antigenic domain defined by the linear sequence RPLGEV, which corresponds to amino acid residues 37–42 of human ERα.16 The specificity of clone EP1 for an epitope in the N-terminal A/B domain is consistent with that of the ERα antibody cocktail in the ER/PR pharmDx kit, but distinct from clone SP1 which is derived from the C-terminal domain of the ERα molecule.17 When assessed with normal tissues, the IHC staining patterns produced by this antibody are consistent with previous observations, with epithelial cells and/or stromal cells from breast, cervix, oesophagus, ovary, prostate, tonsil and uterus exhibiting nuclear staining.18–23
In a comparative analysis of 314 cases, clone EP1 demonstrated 96.2% overall concordance with the ERα component of the ER/PR pharmDx kit. In additional comparisons with clone SP1, a very strong overall agreement (94.9% and 96.9% for Oncotype Dx and follow-up TMA, respectively) was observed.
Disagreement in reading of ER IHC stains often occurs at the lower limit of the staining intensity range, as it may be difficult to classify a nucleus as weakly positive or negative when contrasted against a blue nuclear counterstain. A recent study documented the importance of staining intensity as the major source of discordance between IHC and fluorescence-based AQUA analysis of ER.24 To analyse this issue, we also evaluated the intensity of staining in the comparative testing between clones EP1 and SP1 using cases that showed strong intensity or had greater than 10% of tumour cells expressing ER. This analysis clearly demonstrated the better intensity of staining with EP1 antibody when compared with SP1, the p value being significant for both the analyses.
In summary, we document that rabbit monoclonal antihuman ERα, clone EP1 is a highly sensitive and specific antibody for use in the detection of ERα by IHC. In multiple comparisons on a large series of breast cancer cases, clone EP1, when used with the Dako Autostainer Link system and FLEX protocol, identifies a highly comparable number of cases as ER-positive or ER-negative when compared with other established ER antibody assays. Ease of interpretation is also facilitated by the use of EP1, with a greater number of low positive cases demonstrating a stronger intensity and higher proportion of positive tumour cells.
Take-home messages
-
Immunohistochemical (IHC) assessment of hormone receptor expression is important in breast cancer diagnosis. It is essential that optimal reagents and assays are used for accurate performance of this assessment. Rabbit monoclonal antibodies have been shown to be superior to mouse monoclonal antibodies in IHC assays, and a new rabbit monoclonal antibody to ERα, clone EP1, was evaluated in the studies described in this manuscript. It was demonstrated that clone EP1, used with the Dako EnVision FLEX detection system, is comparable to the anti-ERα component of the Dako ER/PR pharmDx kit, and shows a high degree of concordance to the Ventana CONFIRM ERα assay which uses rabbit monoclonal antibody clone SP1. The EP1/EnVision FLEX assay resulted in a stronger staining intensity compared to SP1/BenchMark ultraView DAB, allowing improved interpretation of the ER IHC results.
Interactive multiple choice questions
This JCP review article has an accompanying set of multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://jcp.bmj.com/education. Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into JCP with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Acknowledgments
Tracey Bender Department of Pathology, Indiana University for secretarial assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Contributors Design: SB, TP; Writing: SB, ITV, BS, BE, AS, TP; Material: SB, TP, BS; Technique: SH, AS, LB-T, CD; Stats: SB, BS; Overall: All authors.
-
Competing interests Betsy Spaulding, Anna Strickland, Therese Phillips are employees of Dako North America, Inc. and Bjorn Elleby is employee of Dako Denmark A/S. Sunil Badve is supported by the Scholarly Program for Susan G Komen for the Cure.
-
Provenance and peer review Not commissioned; internally peer reviewed.