Article Text

Abstract
Aims: To determine the value of squamous mucosal histology in the assessment of patients with gastro-oesophageal reflux symptoms.
Methods: Sixty six patients with reflux symptoms underwent endoscopy with oesophageal biopsy, manometry, and 24 hour oesophageal pH testing. The following histological features were assessed in squamous mucosa: the degree of basal cell hyperplasia, the degree of papillary zone elongation, and the density of neutrophil and eosinophil infiltration. Comparisons were made between the histological findings and the oesophageal function tests.
Results: The correlation between the traditionally accepted histological markers of gastro-oesophageal reflux disease in squamous mucosa and 24 hour pH testing was predominantly negative, with the exception of neutrophil inflammation in the squamous mucosa of patients with complicated reflux disease.
Conclusions: This study was unable to confirm the value of the Ismail-Beigi criteria as histological markers of acid reflux. By inference, biopsy of the oesophageal squamous mucosa is of limited value in the assessment of patients with reflux symptoms.
- ambulatory pH monitoring
- gastro-oesphageal reflux disease
- histology
- oesophagitis
Statistics from Altmetric.com
It is over 25 years since Ismail-Beigi et al described the effects of gastro-oesophageal reflux disease (GORD) on the histology of the oesophageal squamous mucosa.1,2 These studies focused upon lengthening of the papillae and hyperplasia of the basal zone. Although subsequent reports3,4 indicated that these findings were non-specific, they have stood the test of time and have become accepted as part of the histological diagnosis of reflux disease.5–7 Critical appraisal of the literature reveals that there have been surprisingly few reports8–10 comparing these histological “markers” of reflux oesophagitis to the accepted gold standard of 24 hour pH monitoring.11,12
“It is over 25 years since Ismail-Beigi et al described the effects of gastro-oesophageal reflux disease on the histology of the oesophageal squamous mucosa”
The aim of our current study was to correlate the histological features of oesophagitis with oesophageal function tests (stationary manometry and 24 hour pH monitoring) to determine the place of squamous mucosal histology in the assessment of patients with symptoms of gastro-oesophageal reflux disease.
PATIENTS AND METHODS
The study population comprised 66 patients (42 men) with a median age of 57 years (range, 21–80), who were undergoing gastroscopy for the symptoms of heartburn and/or regurgitation occurring at least twice weekly for ≥ 3 months. These patients formed part of a cohort of 150 consecutive patients with reflux symptoms undergoing endoscopy and biopsy as part of a previously published study.13 Our study was approved by the Bro-Taf local research ethics committee; each patient gave written informed consent (Protocol 96/1627). Patients underwent endoscopy with biopsy, manometry, and 24 hour oesophageal pH studies after discontinuing proton pump inhibitors for two weeks and H2 receptor antagonists for 48 hours.
Endoscopy
Endoscopy was performed in a standardised fashion, with visualisation of the oesophagus, stomach, and duodenum. A hiatal hernia was defined by a ≥ 2 cm disparity between the location of the crural impression and the location of the top of the gastric rugal folds. The presence of oesophagitis was identified and graded according to the Savary-Miller classification.14 Barrett's oesophagus was defined in accordance with the American College of Gastroenterology guidelines.15 A positive pH test but absence of erosive oesophagitis was termed uncomplicated reflux disease, whereas complicated reflux disease was defined as a positive pH test and the presence of either erosion, stricture, or Barrett's oesophagus. Biopsies of the squamous oesophagus, including those patients with Barrett's oesophagus, were obtained from a location 2 cm proximal to the squamo–columnar junction.
Histology
Biopsy specimens were fixed in 4% buffered formalin and 4 μm thick paraffin wax embedded sections were stained with haematoxylin and eosin and reviewed by a single pathologist who was blinded to the endoscopic findings. The following parameters were assessed1,2:
The degree of basal cell hyperplasia, expressed as a percentage of epithelial thickness: none (0–15%), mild (16–33%), moderate (34–67%), and severe (>67%).
The presence or absence of papillary zone elongation, determined by calculating papillary length as a percentage of epithelial thickness: absent (0–67%) and present (> 67%).
The density of neutrophil and eosinophil infiltration: none (0/high power field), mild (1–2/high power field), moderate (3–10/high power field), and severe (> 10/high power field). The area of one high power field was 0.229 mm2.
When there was disparity between biopsies, the score for the most abnormal area was recorded.
Manometry and 24 hour pH studies
Oesophageal manometry was performed using a five channel, water perfused polyethylene catheter. For each of the five channels, measurements of the lower oesophageal sphincter total length, abdominal length, and the mean resting pressure at the respiratory inversion point were made.16 The averages of these values were used. Oesophageal peristaltic function was assessed by placing the catheter so that the pressure transducers were located 1, 6, 11, 16, and 21 cm below the distal border of the upper oesophageal sphincter. Eleven water swallows, each of 5 ml, were given to the patient, allowing a 30 second interval between each. Manometric oesophageal length was defined as the distance between the distal border of the upper oesophageal sphincter and the proximal border of the lower oesophageal sphincter.
Following calibration to pH 1 and pH 7, an antimony pH electrode was positioned 5 cm above the proximal border of the lower oesophageal sphincter. pH measurements were recorded on a microdigitrapper (Synectics, Middlesex, UK) and downloaded upon completion of the study to a desktop computer for automated analysis using the Gastrosoft software (Synectics).
During the study period, subjects were asked to consume two meals and to refrain from taking carbonated beverages, citrus fruits or their juices, alcohol, and coffee. Patients were instructed to remain in the upright position during the daytime and to assume the recumbent position only upon retiring to bed.
Twenty four hour pH data were recorded as the percentage time spent at pH < 4, including all time periods within the analysis. Increased oesophageal acid exposure was defined by a total time oesophageal pH < 4 of 4.4%.11,12
Statistics
Non-parametric statistical tests were used, the Mann-Whitney U-test and Kruskal-Wallis test for continuous data, with comparison of proportions by the χ2 test. Significance was assumed at the 5% level.
RESULTS
The endoscopic findings were grade 0 oesophagitis in 39 patients, grades I–III oesophagitis in nine patients, grade IV oesophagitis in four patients, and grade V oesophagitis (Barrett's oesophagus) in 14 patients. Table 1 compares the characteristics of these 66 patients who underwent manometry and pH testing with those of the 84 patients from the original study cohort of 150 who did not undergo these investigations (see above). In all respects, the two groups were similar, indicating that a representative sample had been obtained.
Characteristics of 66 study patients compared with the 84 patients not undergoing oesophageal manometry and 24 hour pH testing
Figure 1 shows that patients with complicated reflux disease had a higher frequency of severe neutrophil inflammation (nine of 21) compared with patients with uncomplicated reflux disease (none of 18; p < 0.01) and those without reflux (two of 23; p < 0.05). No differences were seen between the severity of neutrophil inflammation in patients with negative pH studies and those with uncomplicated reflux disease.
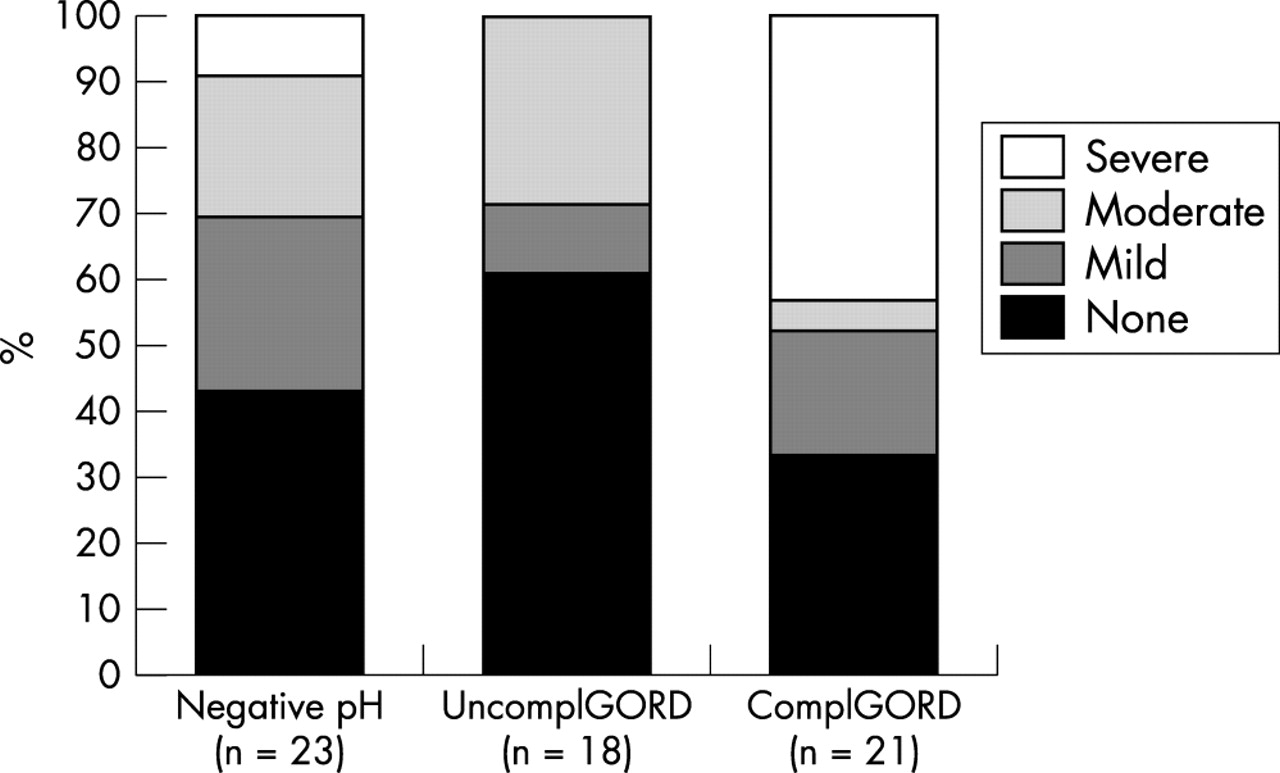
The severity of neutrophil inflammation in squamous mucosa is shown. Note the higher grades of inflammation in patients with complicated gastro-oesophageal reflux (ComplGORD) compared with those with uncomplicated GORD (UncomplGORD) and patients without reflux (Negative pH).
There was no significant association between the indices of basal cell thickening or papillary zone elongation and reflux disease (table 2), although there was a trend for moderate or severe basal cell hyperplasia to be more common in complicated reflux disease than in subjects with a negative pH study or those with uncomplicated reflux (30% v 9% and 12%, respectively).
Prevalence of squamous mucosal histological abnormalities
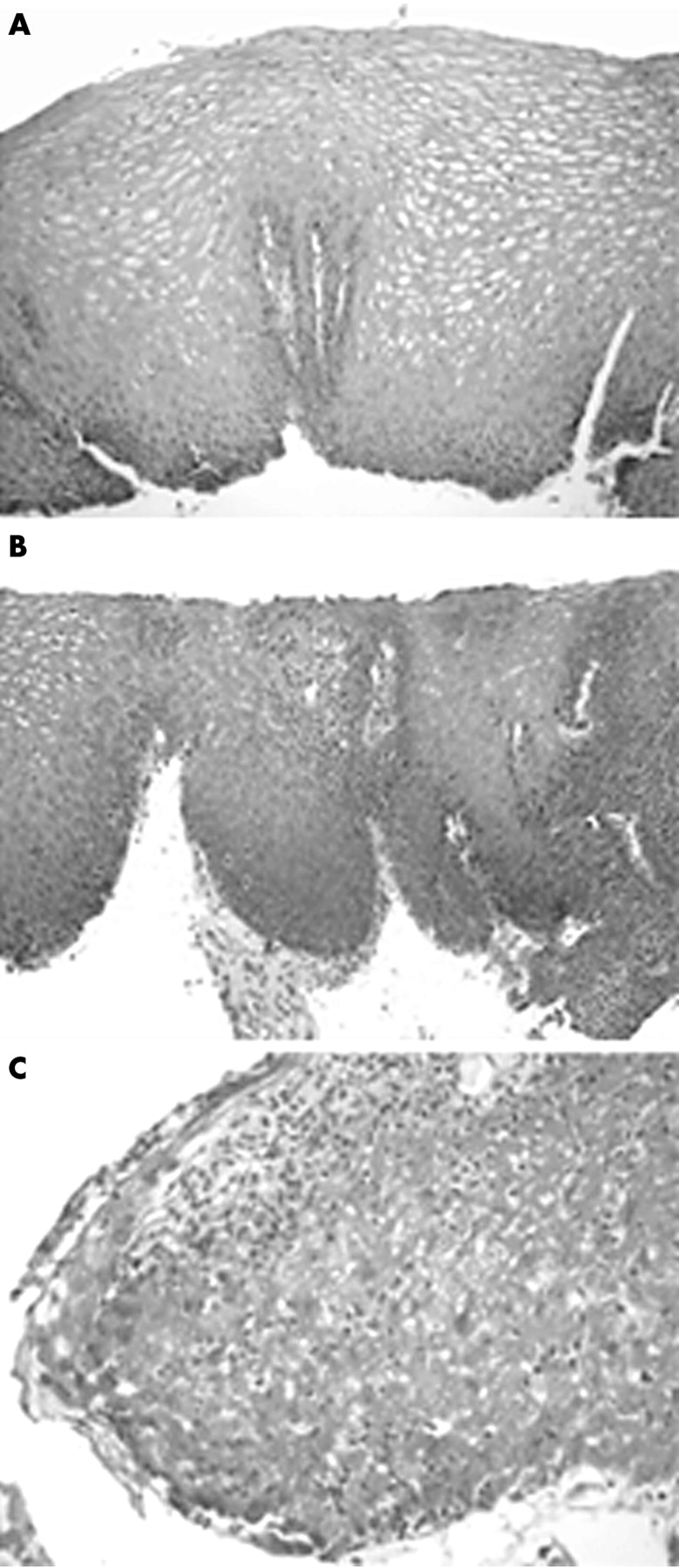
Eosinophils were not identified in the sections. Severe neutrophil inflammation was associated with reductions in lower oesophageal sphincter pressure and contraction amplitudes throughout the smooth muscle portion of the oesophagus (table 3). As the intensity of neutrophil inflammation in squamous mucosa increased, the abdominal length of the lower oesophageal sphincter (fig 2) and the manometric oesophageal length fell progressively (fig 3). Figure 4A–C shows histological examples.
Relation between severity of neutrophil inflammation in squamous mucosa and lower oesophageal sphincter/oesophageal body characteristics
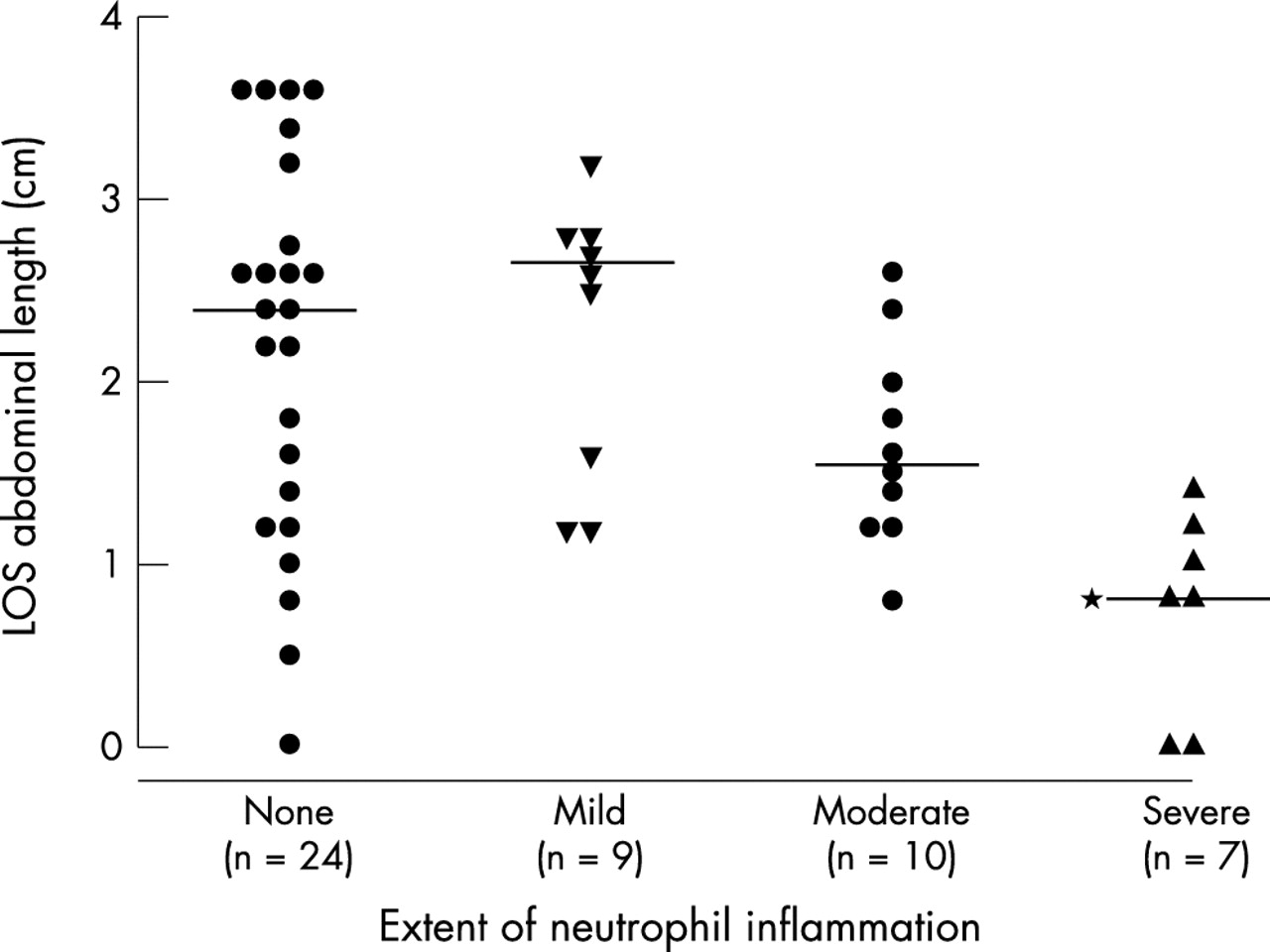
Relation between lower oesophageal sphincter (LOS) abdominal length and the extent of neutrophil inflammation in the oesophageal squamous mucosa. Note the progressive fall in abdominal length as the intensity of neutrophil infiltration increases. *p < 0.01 v none and v mild, p = 0.01 v moderate.
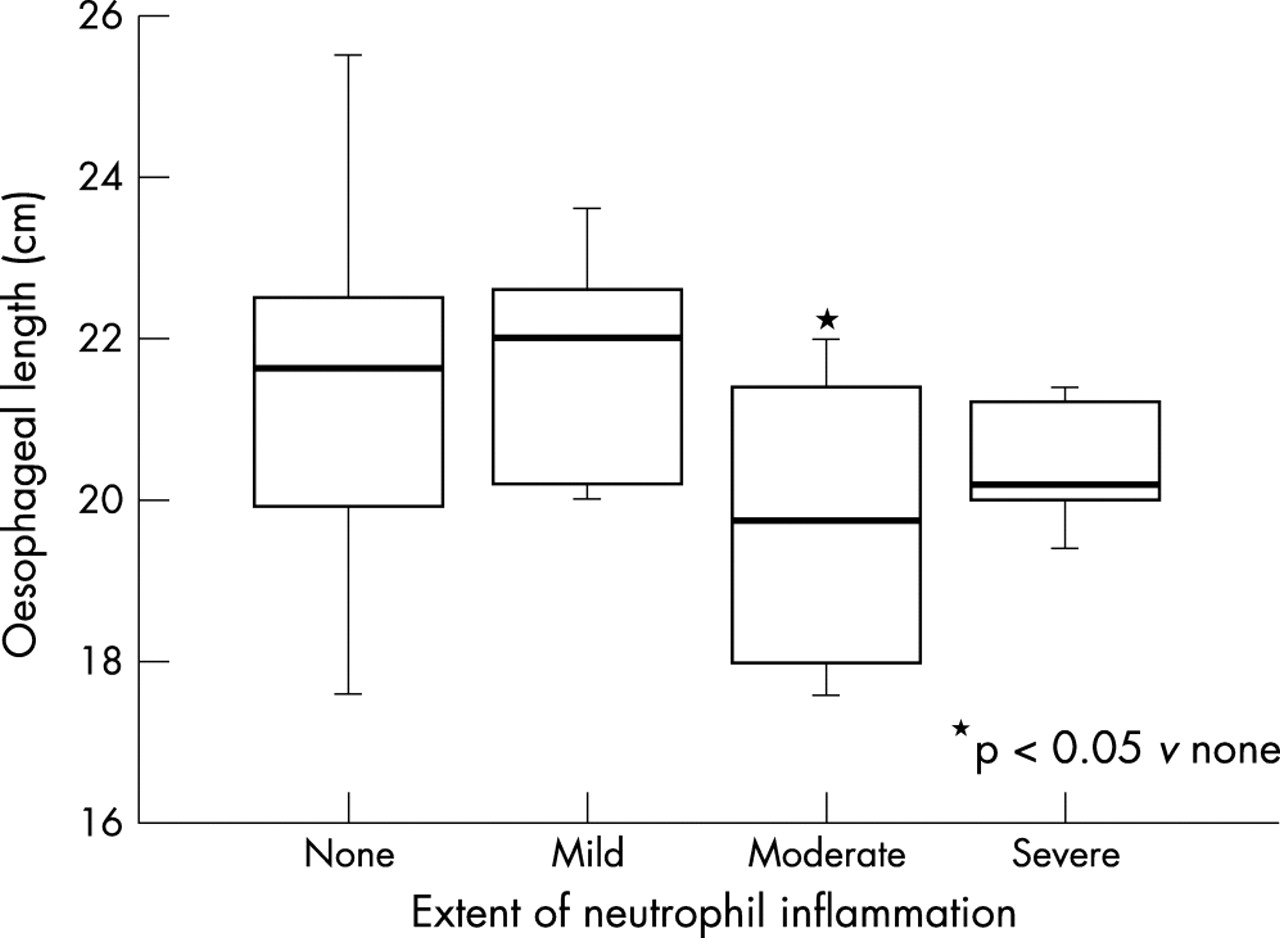
Box and whisker plot showing the relation between manometric oesophageal length and the extent of neutrophil inflammation in the oesophageal squamous mucosa. Note the progressive fall in oesophageal length as the intensity of neutrophil infiltration increases.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examples of oesophageal biopsies from patients with symptoms of gastro-oesophageal reflux disease (haematoxylin and eosin stained). (A) Normal appearing biopsy (mild basal cell hyperplasia, no papillary zone elongation, no inflammatory infiltrate). (B) Biopsy showing severe basal cell hyperplasia, papillary zone elongation, and mild neutrophil infiltration. (C) Incipient ulceration (severe neutrophil infiltration).
DISCUSSION
The correlation between traditionally accepted markers of inflammation in squamous mucosa1,2,17 and acid reflux, as measured by pH monitoring, was predominantly negative in our study. Only neutrophil infiltration in squamous mucosa in patients with endoscopically visible oesophagitis correlated with the severity of reflux. By definition, this implies that in non-erosive reflux disease biopsy is unreliable, and underscores the importance of 24 hour oesophageal pH testing.
In 1970, Ismail-Beigi and colleagues published their much cited study evaluating the squamous mucosa of patients with symptoms of GORD. Based upon their observations in 33 subjects with GORD symptoms and 21 healthy volunteers, the investigators concluded that the normal thickness of the basal zone should be less than 15% of the entire thickness of the squamous epithelium, that the papillae should extend for less than two thirds of the distance to the surface epithelium, and that the squamous epithelium should not contain neutrophils. These criteria were soon afterwards revalidated,17 and have since been widely used as histological markers for GORD.5–7 The findings of more recent studies have generally been less impressive than the findings of earlier work, possibly because the earlier reports included a high proportion of patients with erosive GORD. Based upon all published reports,1,3,4,9,17–19 basal zone thickening has been noted in 15–95% of patients with GORD and 6–40% of controls (median values, 56% v 14%); papillary zone lengthening in 21–98% of patients with GORD and 6–47% of controls (median values, 50% v 14%); and neutrophil inflammation in 18–30% of patients with GORD and 0–8% of controls (median values, 23% v 0%). In our study, we did not look for intraepithelial balloon cells, although they have been reported to be another putative histological marker of oesophagitis.20
Take home messages
-
Except for neutrophil inflammation in the squamous mucosa of patients with complicated reflux disease, the traditionally accepted histological markers of gastro-oesophageal reflux disease in squamous mucosa did not correlate with 24 hour pH testing
-
Thus, we were unable to confirm the value of the Ismail-Beigi criteria as histological markers of acid reflux
-
It therefore seems that the biopsy of the oesophageal squamous mucosa is of limited value in the assessment of patients with reflux symptoms
“We were unable to confirm the value of histological changes in the oesophageal squamous mucosa as markers of gastro-oesophageal reflux in patients with non-erosive reflux disease”
Only two studies have compared squamous mucosal histology directly with the results of 24 hour pH studies. In the first report by Johnson et al,8 on 100 patients, 69 with positive pH studies, the authors found significant correlations between oesophageal acid exposure and the length of both the papillary and basal cell zones, although the correlation coefficients were low, none exceeding 0.33. In the other study, Schindlbeck and colleagues9 found only minor differences in the prevalence of the Ismail-Beigi histological features between 13 patients with non-erosive reflux disease, 11 patient controls, and seven healthy subjects. They concluded that the low sensitivity of the criteria made them unsuitable for clinical use. In a recent study, Nandurkar et al,19 defining histological oesophagitis as any two abnormalities of the three features—basal zone thickening, papillary lengthening, or neutrophil infiltration—found no difference in the prevalence of histological oesophagitis between 75 patients with reflux symptoms and 69 patients free of reflux symptoms (22% v 17%).
In summary, we were unable to confirm the value of histological changes in the oesophageal squamous mucosa as markers of gastro-oesophageal reflux in patients with non-erosive reflux disease. Therefore, biopsy of the oesophageal squamous mucosa is of limited value in the assessment of patients with GORD symptoms. It is possible that histological features in the oesophageal squamous mucosa might predict long term complications, although there is, to date, no good evidence for this.
Acknowledgments
Mr D Bowrey was funded by a Royal College of Surgeons of England/Welsh Office Research Fellowship. Laboratory costs were provided by a grant from the Wales Office of Research and Development for Health and Social Care.