Article Text

Abstract
Endometrial stromal tumours (ESTs) are diagnosed in most instances by light microscopy. Often, the greatest challenge is to distinguish between the different subtypes of these tumours. Furthermore, a handful of new or relatively new entities have been described in the literature, which may cause problems in the differential diagnosis; highly cellular leiomyoma is the most common. In addition, new antibodies have been developed to help in the distinction of ESTs from their mimics, as there are prognostic and therapeutic implications. A practical approach is provided for the diagnosis of ESTs on the basis of systematic assessment of histological and immunohistochemical parameters, and recent developments related to these tumours are highlighted.
- ESN, endometrial stromal nodule
- ESS, endometrial stromal sarcoma
- EST, endometrial stromal tumour
- EST-SMD, endometrial stromal tumours with smooth-muscle differentiation
- HCL, highly cellular leimyoma
- IVL, intravenous leiomyomatosis
- PEComa, perivascular epithelioid cell
- UES, undifferentiated endometrial sarcoma
- UTROSCT, uterine tumour resembling an ovarian sex cord stromal tumour
Statistics from Altmetric.com
- ESN, endometrial stromal nodule
- ESS, endometrial stromal sarcoma
- EST, endometrial stromal tumour
- EST-SMD, endometrial stromal tumours with smooth-muscle differentiation
- HCL, highly cellular leimyoma
- IVL, intravenous leiomyomatosis
- PEComa, perivascular epithelioid cell
- UES, undifferentiated endometrial sarcoma
- UTROSCT, uterine tumour resembling an ovarian sex cord stromal tumour
Endometrial stromal tumours (ESTs) of the uterus are the second most common mesenchymal tumours of the uterus even though they account for <10% of all such tumours.1 In the latest 2003 World Health Organization classification,2 ESTs are divided into
-
endometrial stromal nodule (ESN),
-
low-grade endometrial stromal sarcoma (ESS),
-
undifferentiated endometrial sarcoma (UES).
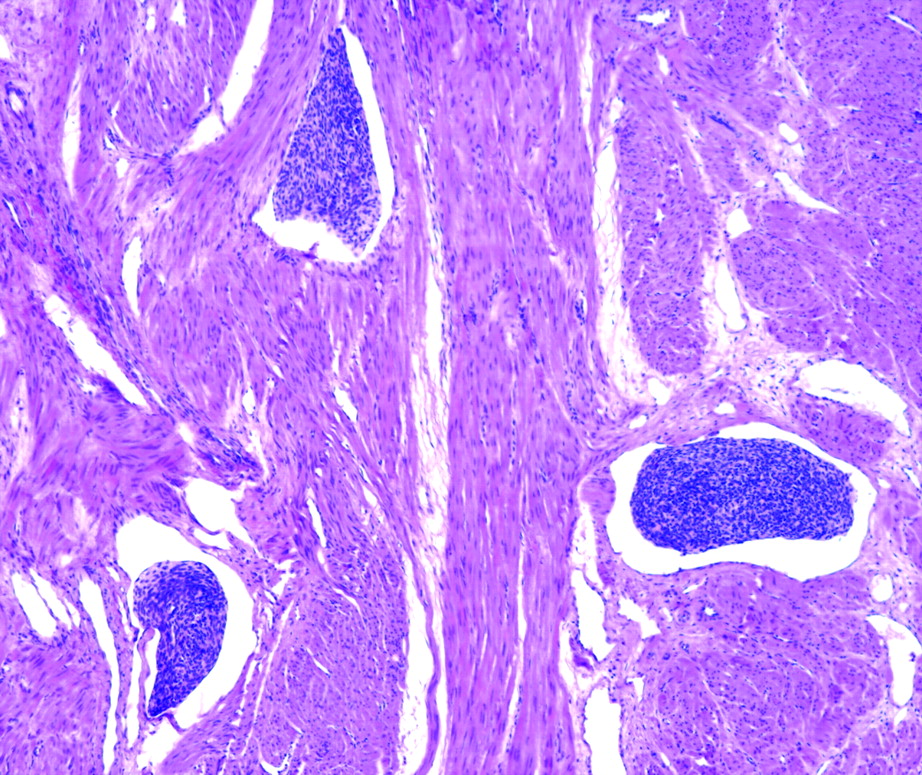
The ESN and the low-grade ESS fall in the lower end of the spectrum of this group of tumours. Both are typically composed of a diffuse growth of small blue cells with scant cytoplasm, and oval to spindle nuclei that resemble the endometrial stromal cells of the proliferative endometrium (fig 1).3,4 At the other end of the spectrum is the UES, a very high-grade sarcoma, which does not resemble the proliferative endometrium. The diagnosis of UES is reached after excluding other high-grade tumours of the uterus with a sarcomatous component.5,6
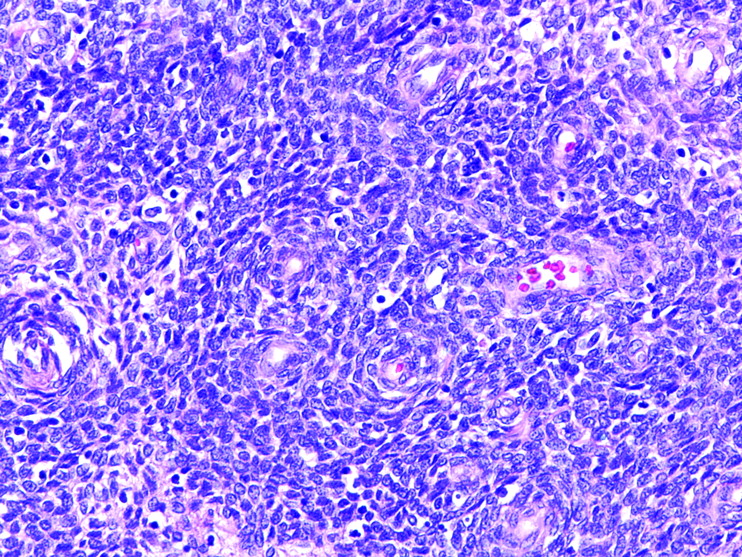
Endometrial stromal tumour. Small uniform cells with oval nuclei and scant cytoplasm grow in sheets and focally whorl around arterioles.
DISTINCTION OF ESN FROM LOW-GRADE ESS
Both tumours have similar presentation, vaginal bleeding being the most common.7 Of note, about a third to a half of the low-grade ESSs have extrauterine spread at the time of diagnosis and, rarely, these tumours may initially present at an extrauterine site, most commonly the ovary.6–9 Thus, when evaluating an ovarian tumour with a microscopic appearance consistent with an EST, it is important to exclude a history of a uterine EST and to suggest inspection of the uterus, as ESTs of the uterus are far more common than primary ovarian ESTs.
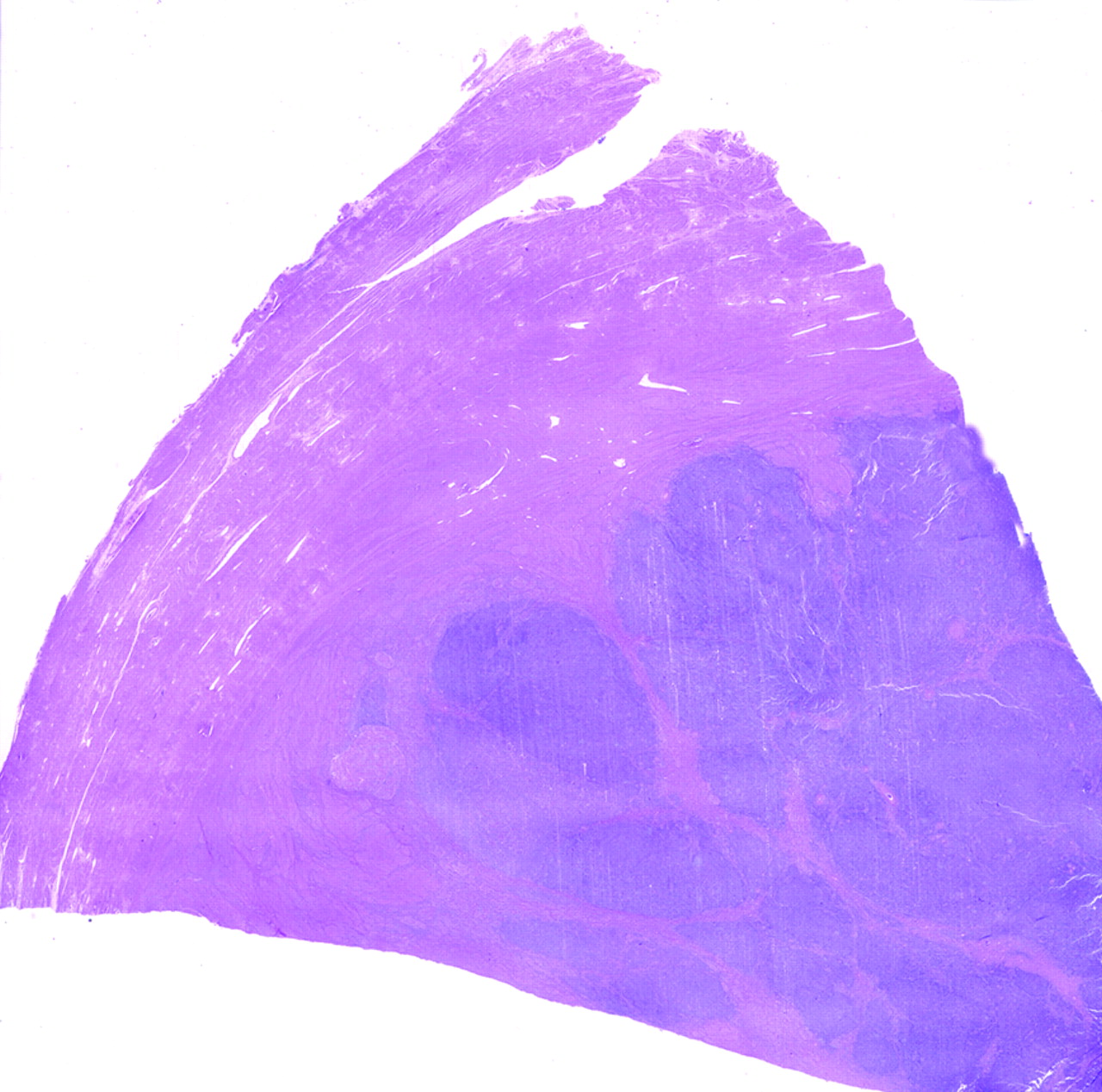
On gross examination, the main differentiating feature between the two neoplasms is tumour circumscription. Typically, ESN is a well-circumscribed, although non-encapsulated, neoplasm (fig 2).10,11 In contrast, low-grade ESSs often show an irregular nodular growth affecting the endometrium, myometrium or both. The main mass is often associated with varying degrees of permeation of the myometrium, including worm-like plugs of tumour that fill and distend myometrial veins, often extending to parametrial veins.6,7,12 However, on rare occasions, low-grade ESSs may appear deceptively well circumscribed on gross examination. Both tumours have a soft, tan to yellow cut surface.

Endometrial stromal nodule. A large well-circumscribed mass shows a tan cut surface, scattered cysts and an extensive area of infarction.
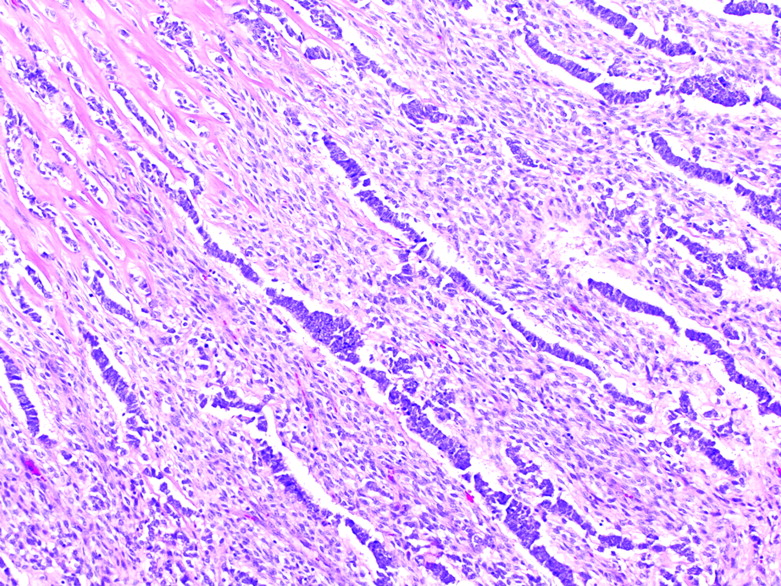
Microscopically, the most important single criterion for the diagnosis of ESN is the finding of a non-infiltrative border of the tumour. Focal irregularities in the form of lobulated or finger-like projections into the adjacent myometrium that are not ⩾3 mm and are not >3 in number may be seen. Vascular invasion is not allowed; thus, if present, the tumour should be diagnosed as a low-grade ESS.10 In contrast with ESN, low-grade ESSs permeate the myometrium in irregular tongues and often invade myometrial (fig 3) as well as extrauterine veins and lymphatics (fig 4).6,7,12 Myometrial invasion and vascular invasion are the two most important features used to distinguish between these two tumours. In most cases it is impossible to differentiate between an ESN and a low-grade ESS on the basis of curettage specimens and, thus, distinction can only be confidently established in a hysterectomy specimen. This is an important issue when the patient is of reproductive age and desires to preserve her uterus. In these circumstances, a combination of diagnostic imaging and hysteroscopy may be used to monitor the growth of the tumour, and occasionally local excision has been successful.13,14

Low-grade endometrial stromal sarcoma. Irregular nests and islands of blue cells with a prominent delicate vascular network diffusely infiltrate the myometrium.

Low-grade endometrial stromal sarcoma. Nests of neoplastic endometrial stromal cells are present in vascular spaces.
Other microscopic features, including whorling of the neoplastic stromal cells around arterioles, hyalinisation of the arteriolar walls, collagen bands or plaques, diffuse areas of hyalinisation, foamy histiocytes, cystic degeneration associated with cholesterol clefts, and necrosis, may be seen in both tumours and are not useful in the differential diagnosis.6,7,10–12
The treatment of choice for an ESN is surgical resection, whereas patients with low-grade ESS undergo hysterectomy with bilateral salpingo-oophorectomy. Adjuvant treatment either with progestins, radiation therapy or even aromatase inhibitors may be given, depending on the extension of the tumour and patients’ risk factors.15–20 From the prognostic point of view, it is extremely important to distinguish between these two tumours, as ESNs do not relapse and low-grade ESSs have a low malignant potential characterised by late recurrences. For this reason, patients with low-grade ESS should be followed up for an extended period of time, up to 30 years.6,7,16,21,22
Potential pitfall
Low-grade ESSs may be well circumscribed and may simulate an ESN on gross examination.
Recommendations
In endometrial curettage, the working diagnosis should be EST, as in most cases the margin cannot be completely assessed.
Adequate sampling of the tumour–myometrial interface is necessary to evaluate the degree of infiltration of the tumour into the myometrium, correctly classify the tumour and thus properly treat the patient.
DISTINCTION OF ESN FROM LOW-GRADE ESS WITH LIMITED INFILTRATION
These two lesions are grossly indistinguishable, as they have well-defined pushing borders in relationship to the surrounding myometrium.11 On microscopic examination, low-grade ESS with limited infiltration is defined as a tumour that does not fulfil the criteria for an ESN (having <3 tongues or nodules at the most 3 mm in largest dimension) and does not have the overt permeative growth of a low-grade ESS or the associated vascular invasion (fig 5). These tumours have been recently described in a series of 50 ESNs that included three such tumours.11 Follow-up was available for only one patient with a tumour that had six tongues or detached nodules from the main mass ranging from 1 to 5 mm, but it was limited to 62 months. The tumour was extensively sampled, with 51 slides showing the tumour–myometrium interface. The behaviour of these tumours is very difficult to predict, as studies with long follow-up are scarce. Currently, these tumours are best diagnosed as low-grade ESSs with an explanatory note stating that the tumour is not as overtly invasive as a typical low-grade ESS, and for this reason the tumour may behave in a more benign fashion.

Endometrial stromal sarcoma with limited infiltration. Several distinct islands of the tumour, some showing a typical tongue-like configuration, are seen in close proximity to the main mass. Occasional nests are >3 mm away.
Potential pitfall
Relying on the gross circumscription may lead to undersampling of the tumour and therefore to a diagnosis of ESN.
Recommendations
The tumor–myometrium interface should be sampled to identify invasive foci.
For practical purposes and owing to limited experience with these tumours, it is currently best to report them as low-grade ESS, with an explanatory note describing that the degree of invasion is much less than that seen in conventional low-grade ESS.
DISTINCTION OF LOW-GRADE ESS FROM HIGH-GRADE ESS AND UES
On gross examination, high-grade ESS and UES show a destructive infiltrative growth into the myometrium, which contrasts with the permeative invasion of the myometrium and myometrial vessels seen in low-grade ESS.2,5,6 Both tumours have a grey, fleshy, cut surface often associated with areas of necrosis. Microscopically, marked degrees of nuclear atypia are absent in low-grade ESS, but are characteristic of high-grade ESS and UES. Although low-grade EES often shows mitotic rates <3 in 10 high-power fields, higher rates do not exclude this diagnosis, and it is now accepted that mitotic activity is not important in classifying an ESS as low or high grade.5,6 If a tumour has the typical morphology of an EST with the characteristic tongue-like growth into the myometrium and/or myometrial veins, it should be classified as a low-grade ESS regardless of the mitotic counts, as mitotic counts do not influence prognosis in these tumours. The most important feature for distinguishing low-grade from high-grade tumours is the resemblance of the neoplastic cells to proliferative endometrial stroma. The diagnosis of high-grade ESS should be made only in cases where a component of low-grade ESS may be recognised; otherwise, the diagnosis is that of UES.3 It is extremely important to distinguish low-grade from high-grade tumours, as the high-grade tumours behave as high-grade sarcomas and carry a poor prognosis.5,6 UESs should be diagnosed only after extensive sampling has excluded smooth or skeletal muscle differentiation, as this would result in a diagnosis of high-grade leiomyosarcoma or rhabdomyosarcoma. Small foci of carcinoma admixed with the sarcomatous component would favour a malignant mixed mullerian tumour, whereas the finding of typical adenosarcoma would clinch the diagnosis of adenosarcoma with sarcomatous overgrowth. This may be difficult in curettage specimens, owing to the limited representation of the tumour. CD10 expression is not helpful in this differentiation as high-grade ESSs as well as leiomyosarcomas, rhabdomyosarcomas and malignant mixed mullerian tumours, express this marker.23–25 The differential diagnosis is largely based on morphology. Smooth-muscle markers and myogenin or myoD1 may be used to rule out a leiomyosarcoma or rhabdomyosarcoma respectively, or to identify a rhabdomyosarcoma component in a malignant mixed mullerian tumour.
Potential pitfall
A high mitotic rate may lead to a misdiagnosis of high-grade ESS.
Recommendations
If the histological features of the tumour are reminiscent of endometrial stroma the diagnosis should be low-grade ESS. The diagnosis of high-grade ESS can be made only when a component of low-grade ESS is recognised and, therefore, UES is a diagnosis of exclusion. Extensive sampling of the tumour is necessary to rule out other high-grade uterine tumours.
DISTINCTION OF EST FROM HIGHLY CELLULAR LEIOMYOMA
The clinical presentation of highly cellular leimyomas (HCLs) is non-specific, as occurs with most leiomyomas. However, these tumours may be confused with ESTs on gross and microscopic examination.26 On gross examination, HCLs have an appearance that closely overlaps with that seen in ESTs as they are yellow or yellow-tan and have a soft consistency (fig 6), in contrast with conventional leiomyomas, which are typically white with a firm cut surface. On histological examination, shared features include hypercellularity and prominent vascularity (fig 7A), as well as, in some cases, the finding of an irregular margin in relation to the surrounding myometrium. Helpful histological clues in this differential diagnosis are as follows:

Highly cellular leiomyoma associated with intravenous leiomyomatosis. A tan to yellow mass with a slightly irregular margin is associated with tan worm-like plugs of tumour distending vascular spaces.

Highly cellular leiomyoma. A densely cellular proliferation of small spindle cells with elongated nuclei and scant cytoplasm is associated with large thick-walled vessels (A). The smooth-muscle cells are positive for CD10 (B) and for h-caldesmon (C).
-
Focal merging of the highly cellular areas with typical fascicular areas of smooth-muscle neoplasia, more commonly seen at the periphery of the tumour in most cases.
-
Large thick muscular-walled blood vessels throughout the tumour, in contrast with the arterioles of an endometrial stromal neoplasm (fig 7A). On occasion, some large, thick-walled blood vessels may be found at the junction of the EST and the myometrium; however, these are most likely entrapped.
-
Cleft-like spaces, some apparently representing compressed vessels, others apparently the result of oedema.26,27
In cases where the diagnosis is difficult to establish by light microscopy, immunohistochemical analysis may be helpful in arriving at the correct diagnosis, which is crucial owing to differences in treatment and prognosis.26 If the diagnosis of HCL is based on curettage material, the tumour can be managed conservatively, whereas given the diagnosis of an EST, the patient will need hysterectomy to further categorise the tumour.
The neoplastic endometrial stromal cells are typically immunoreactive for vimentin, muscle-specific and smooth-muscle actin, and may be positive for keratin and desmin.28–33 Thus, this panel of antibodies is not helpful in distinguishing EST from HCL or from leiomyosarcoma, the two most common tumours in the differential diagnosis with EST.
Although CD10 was initially thought to be a specific marker of ESTs,34,35 it has been shown that CD10 is expressed in smooth-muscle tumours of the uterus, most commonly in leiomyosarcomas and HCLs (fig 7B).33,36 Other antibodies useful in this differential diagnosis include h-caldesmon (fig 7C),24,33,37–39 histone deacetylase 8,40 and smooth-muscle myosin.40,41 However, it is important to remember that ESTs may have areas with smooth-muscle differentiation that express these markers, underscoring the importance of correlating immunohistochemical results with the morphological findings.24,33,40 Furthermore, leiomyosarcomas may be h-caldesmon negative,38 indicating that a panel of antibodies rather than a single antibody should be used in the differential diagnosis of ESTs and smooth-muscle tumours. Finally, oxytocin receptor, a neurohypophysial peptide associated with muscle contraction during labour, stains all conventional leimyomas and HCLs as well as leiomyosarcomas but is not expressed in ESTs24; however, this antibody is not widely used in daily practice at present.
Potential pitfalls
The finding of prominent cellularity (small blue-cell tumour) in the uterus may lead to the wrong diagnosis of EST, especially as the margin with the surrounding myometrium may appear sharper and worrisome for the “tongue-like” growth of a low-grade ESS. The use of a single antibody, especially CD10, may lead to a wrong final diagnosis.
Recommendations
Fascicular areas, thick-walled blood vessels and cleft-like spaces in the tumour, more often seen at the periphery of the tumour, and the transition of the tumour cells with the surrounding myometrium should be looked for. A panel of antibodies that includes CD10 and two muscle markers should be used. The immunohistochemical findings should be correlated with the morphological findings.
DISTINCTION OF LOW-GRADE ESS FROM HIGHLY CELLULAR INTRAVENOUS LEIOMYOMATOSIS
The clinical presentation of intravenous leiomyomatosis (IVL) is non-specific; however, as with low-grade ESS, this lesion is present outside the uterus at the time of diagnosis in at least 30% of patients. In some, extension of the tumour into the inferior vena cava and the right side of the heart may result in cardiac manifestations, a feature rarely seen in low-grade ESS.42,43
On gross examination, cellular IVL may be misinterpreted as an ESS, because of its prominent intravascular growth, a soft tan to yellow cut surface and frequent association with a conventional leiomyoma that may be confused with the main mass of an ESS (fig 8).44,45 Microscopically, the dense cellularity resembling a HCL may increase confusion with a low-grade ESS (fig 9). Helpful morphological features include all those typically seen in conventional leiomyomas, including the following:

Intravenous leiomyomatosis. Prominent intravascular growth of small blue cells mimics the growth of endometrial stromal sarcoma.

Intravascular leiomyomatosis. Loosely spindle-shaped cells growing inside vascular spaces are seen. The intravascular growth is associated with a highly cellular leiomyoma (not shown).
-
clefted or lobulated contour of the intravascular masses,
-
focal fascicular architecture,
-
cells with blunt-ended nuclei,
-
prominent thick-walled vessels and
-
hydropic change.44
Finally, other clues to the diagnosis of IVL include low mitotic activity in most tumours and the presence of tumour growth beneath the vascular endothelium with colonisation of the walls of veins. However, this phenomenon is seen in only a minority of cases.46
Low-grade ESS and IVL may recur months to years after the initial treatment because of growth of residual tumour in vascular spaces.42 It is, however, important to differentiate between those tumours, as about 50% of patients with low-grade ESS develop pelvic recurrences, a pattern of spread not seen in IVL,6,15,16,44 and also because the main treatment for IVL is still surgical resection, whereas patients with low-grade ESS often receive adjuvant radiation or hormonal treatment.17,22,42
Potential pitfall
Intravascular growth pattern of small blue cells may first be considered a low-grade ESS.
Recommendations
Fascicular areas, thick-walled blood vessels, cleft-like spaces, as seen in HCLs, and tumour growth beneath the vascular endothelium should be looked for. A panel of antibodies should be used that includes CD10 and two muscle markers. The immunohistochemical findings should be correlated with the morphological findings.
DISTINCTION OF EST FROM PERIVASCULAR EPITHELIOD CELL TUMOUR
The perivascular epithelioid cell tumour (PEComa) is a newly described low-grade mesenchymal tumour. It belongs to the family of lesions that includes the clear-cell “sugar” tumours of the lung and pancreas, some forms of angiomyolipoma and rare tumours in other locations.47 All these tumours originate from the perivascular epithelioid cell, which is a cell defined by the presence of abundant clear to eosinophilic granular cytoplasm and positive staining for human melanoma black 45, as well as frequent expression of muscle markers. Interestingly, some tumours are associated with lymphangiomyomatosis as well as tuberous sclerosis, a feature not described in ESTs.47
On gross examination, PEComas may show poorly defined margins, with a fleshy, soft, cut surface that ranges from grey-white to tan or yellow, resembling the appearance of an EST.48
On examination by low-power microscopy, some tumours have a tongue-like infiltrative growth resembling the infiltrative pattern seen in low-grade ESS.48 The tumour cells have abundant clear to eosinophilic cytoplasm that may grow in sheets, with a scant amount of intervening stroma and a prominent network of small blood vessels (fig 10).47–50 Most of the aforementioned features, including eosinophilic or clear cells with abundant cytoplasm, may be seen in ESTs.51,52 However, PEComas show a predominantly nested growth, which is often associated with a focal fascicular growth of cells with elongated nuclei having a similar appearance to that seen in smooth-muscle tumours. Finally, the cells tend to be arranged in a radial fashion around the vessels.47 These features are not encountered in ESTs, and, furthermore, ESTs will show at least focally some areas that resemble the normal endometrial stroma with arterioles.
Perivascular epitheliod cell tumour is composed of sheets of cells with abundant clear cytoplasm.
On immunohistochemical studies, ESTs may be positive for smooth-muscle markers and PEComas may be positive for CD1023,47,48; thus, these markers are not helpful in this differential diagnosis. However, in contrast with PEComas, ESTs do not express human melanoma black 45, Melan-A or microphthalmia factor.47,48
Potential pitfall
CD10 can be positive in PEComa and it may thus be erroneously diagnosed as EST.
Recommendation
When studying a tumour with clear cells, PEComa should always be considered in the differential diagnosis. A panel of antibodies should be used when considering more than one tumour in the differential diagnosis, as tumours may show overlapping results with isolated antibodies.
EST VARIANTS
ESTs may show different types of differentiation including smooth muscle,53–55 fibrous or myxoid change,55–57 sex cord-like elements,11,58–61 glandular differentiation,62,63 epithelioid,52 rhabdoid61,64–66 or clear cells,51 rhabdomyoblastic differentiation,67,68 and granular change.52 Fatty metaplasia and bizarre nuclei have recently been reported in these tumours.68 In this category, the most common problems in differential diagnosis—namely, smooth-muscle and sex cord-like differentiation—will be discussed.
EST with smooth muscle differentiation versus smooth-muscle tumour
On gross examination, endometrial stromal tumours with smooth-muscle differentiation (ESTs-SMD) often show an admixture of soft tan to yellow nodules and firm white whorled nodules, or alternatively the paler, firmer tissue may be seen at the periphery of softer nodules, a picture that is not characteristic of smooth muscle tumours in general (figs 11, 12). To establish the diagnosis of mixed EST-SMD, the smooth-muscle component should occupy at least 30% of the neoplasm as seen by haematoxylin and eosin staining.27 In many cases, the smooth-muscle component characteristically shows nodules with central hyalinisation (starburst pattern), which merge with disorganised short fascicles or long mature fascicles of the smooth muscle, a feature almost never encountered in conventional smooth-muscle tumours (fig 13).53–55 Furthermore, conventional areas of endometrial stromal neoplasia are present in ESTs-SMD, confirming the endometrial stromal origin of the tumour.

Mixed endometrial stromal and smooth-muscle tumour. A well-circumscribed multilobular mass protrudes from the myometrium. It shows firm pale nodules alternating with irregular tan areas.
Mixed endometrial stromal and smooth-muscle tumour. A well-circumscribed tumour composed of smooth muscle and endometrial stroma is abutting the surrounding myometrium. The smooth-muscle component forms a discrete pink rim at the periphery and coarse bundles that alternate with the endometrial stromal component.

Mixed endometrial stromal and smooth-muscle tumour. A central area of hyalinisation shows radiating fibres of collagen that entrap plump neoplastic cells (starburst pattern), which in turn merge with immature bundles of smooth muscle.
Immunohistochemical staining should be interpreted with caution in these cases, as the smooth-muscle component is often positive for CD10 and smooth-muscle markers and this profile may be considered to be diagnostic of smooth muscle neoplasia.24,33 Immunohistochemical staining should be correlated with the different morphological components of the tumour. Conventional areas of endometrial stromal neoplasia should be positive for CD10 but not positive for >1 smooth-muscle marker, being more often positive for muscle actin and desmin.
Potential pitfalls
If the smooth muscle component, particularly when it is mature and relatively well organised, is misconstrued as myometrium, a well-circumscribed tumour may be misinterpreted as an invasive EST and hence an ESS. It is crucial to appreciate that in such cases, we are examining regions with divergent differentiation in the mass itself rather than myometrial invasion by a low-grade ESS.
Coexpression of CD10 and smooth-muscle markers in areas of SMD may lead to the diagnosis of a smooth-muscle tumour.
Recommendations
The term “stromomyoma” should not be used because it implies that the tumour is an ESN. These tumours should be reported as ESNs or ESSs with SMD (depending on the margins), with the designation “mixed endometrial stromal–smooth-muscle tumour” given in parentheses, as the margin is the most important prognostic parameter.
The results by immunohistochemistry should be interpreted in correlation with the appearance of the different areas identified on histological examination.
EST WITH SEX CORD-LIKE DIFFERENTIATION VERSUS UTERINE TUMOUR RESEMBLING AN OVARIAN SEX CORD STROMAL TUMOUR
Uterine tumour resembling an ovarian sex cord stromal tumour (UTROSCT) is strictly defined as a tumour with prominent sex cord-like differentiation in which there is no conspicuous endometrial stromal background.58 The age and clinical presentation is similar for patients with UTROSCT and for those with ESTs except for the fact that the patients with UTROSCT almost never present with metastases.
On gross examination, UTROSCT typically appears as a circumscribed myometrial or submucosal mass that is soft and ranges from grey to tan to yellow, an appearance that overlaps with that of an ESN.
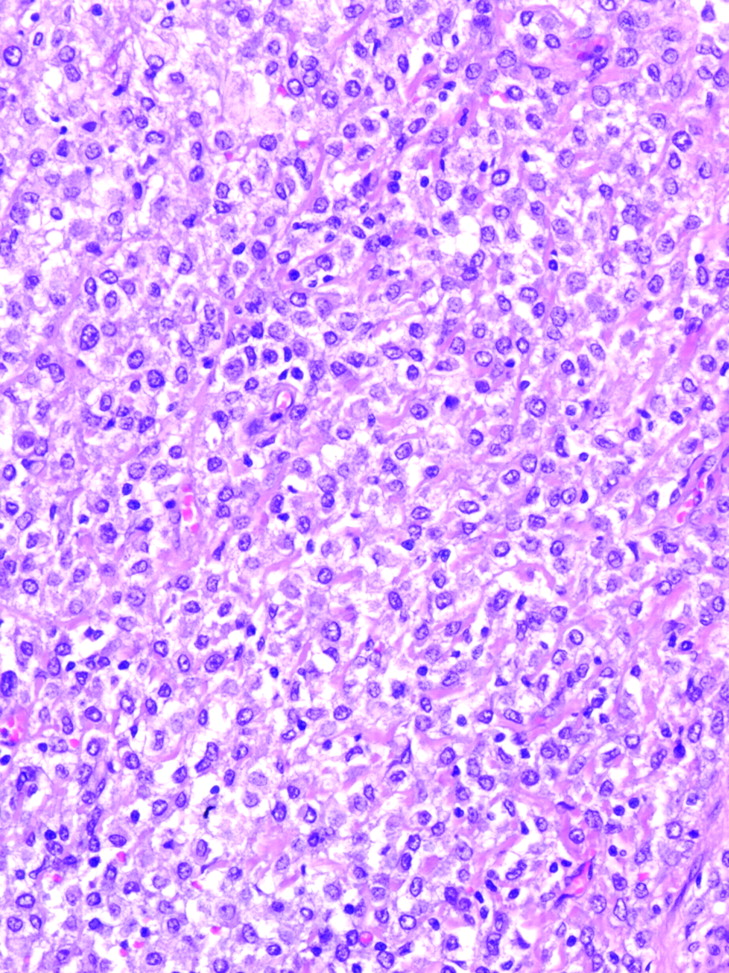
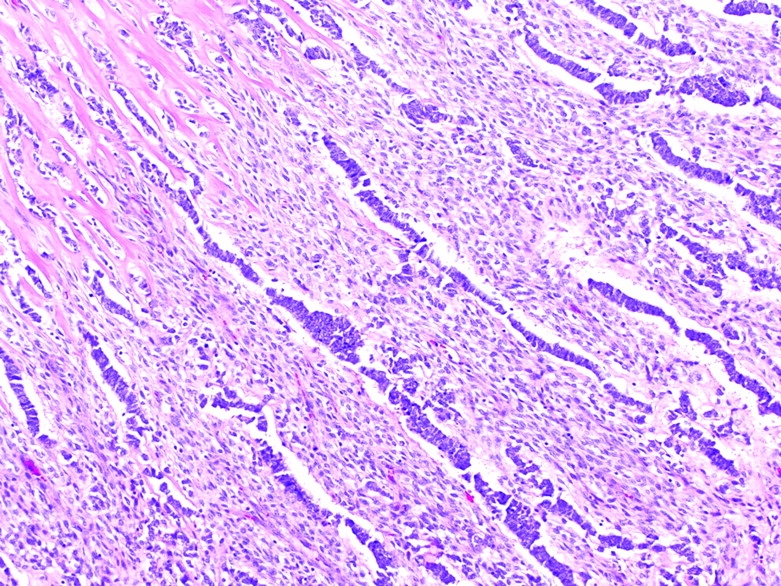
On microscopic examination, ESN and low-grade ESS may show sex cord-like differentiation (fig 14), and the histological appearance of some UTROSCTs may merge imperceptibly with that of ESTs when exhibiting a less than predominant sex cord-like pattern.11,58,59 The histological patterns that create a resemblance to those of ovarian sex cord tumours, especially granulosa-cell and Sertoli-cell tumours, alone or in combination, should be the only elements present in the tumour to establish the diagnosis of UTROSCT.58,59,69
Low-grade endometrial stromal tumour with epithelial-like differentiation. Elongated cords are present in a background of endometrial stromal neoplasia.
Immunohistochemical analysis may be of help in this differential diagnosis. Inhibin, the most specific marker for sex cord stromal tumours of the ovary, is typically negative in pure ESTs,33,59,70–72 but it is often positive in areas of sex cord-like differentiation in ESTs and in UTROSCTs (fig 15A), although positivity varies in intensity and percentage.73 Calretinin and CD99 may also stain normal sex cord elements as well as UTROSCTs (fig 15B), but they are negative in conventional areas of EST.59,72–74 Melan A may show positive staining in sex cord-like cells, consistent with the presence of steroid-producing cells, and is supportive of their specialised gonadal stromal nature, but it is negative in pure endometrial stromal areas.59,73 Finally, CD10, typically positive in ESTs, has been recently reported to be positive also in UTROSCTs.59 These results underscore once again the importance of correlating the immunohistochemical findings with the diverse morphological areas of a given tumour, indicating in this particular scenario that positivity for any of these markers does not establish unequivocally a diagnosis of UTROSCT.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A uterine tumour resembling an ovarian sex cord stromal tumour shows (A) inhibin and (B) calretinin positivity.
Finally, it is important to differentiate UTROSCT from low-grade ESS, as UTROSCT typically behaves in a benign fashion,69,75 whereas patients with low-grade ESSs have frequent recurrences.6,7,16,21,22
Potential pitfalls
Fragments of tumour seen in a curettage specimen that are predominantly composed of sex cord-like elements may lead to the automatic diagnosis of UTROSCT, without consideration of an EST with sex cord-like differentiation.
Positivity for any marker of sex cord differentiation may erroneously lead to a diagnosis of UTROSCT.
Recommendations
It is necessary to sample the tumour extensively to rule out an endometrial stromal component and thus be able to classify the tumour as a UTROSCT.
The distinction of an EST with sex cord differentiation from a UTROSCT can be made only in a hysterectomy specimen. It is important to correlate the immunohistochemical findings with the diverse morphological areas of a given tumour, as areas without sex cord differentiation in an EST do not stain for most markers listed above.
NEW DEVELOPMENTS
It is well known that ESTs often contain oestrogen and progesterone receptors, findings that may have therapeutic and prognostic implications.76,77 However, the presence of these receptors has limited utility in differential diagnosis in as much as these receptors may be found in many other epithelial and mesenchymal tumours of the uterus. Aromatase participates in extraovarian oestrogen production via conversion of androgen to oestrogen through the aromatase enzyme complex.78 Aromatase has been detected in stromal cells of endometriosis, adenomyosis and endometrial carcinomas, as well as ESSs, and in the latter no expression of aromatase tended to correlate with stage I disease in one study.78 The importance of that finding is the introduction of aromatase inhibitors as a new modality of treatment for low-grade ESSs.17–20
Although initial studies on c-kit in ESTs detected absence of staining,33 recent studies have shown some c-kit expression in ESTs.79–81 However, in contrast with gastrointestinal stromal tumours where this expression can be used for treatment purposes, the experience with ESTs is limited and contradictory.
Genetic studies have shown that t(7;17) is the most common translocation encountered in conventional ESTs,82 with involvement of two zinc finger genes, JAZF1 and JJAZ1,83 in conventional ESTs as well as in ESTs-SMD and in those with fibrous or myxoid change.85,86 Other genetic alterations, most often loss of heterozygosity of phosphatase and tensin homolog deleted on chromosome 10, have also been reported in ESTs.1 However, these findings do not at the moment have any prognostic or therapeutic implications.
Take-home messages
-
In most instances, the diagnosis of endometrial stromal tumour (EST) may be established on morphology alone.
-
Extensive sampling may be important in distinguishing endometrial stromal neoplasia from an endometrial stromal sarcoma (ESS).
-
A tumour resembling endometrial stroma should be classified as a low-grade ESS and not as a high-grade ESS.
-
Awareness of the existence of EST variants will help in the correct classification of the tumour.
-
CD10 positivity in a uterine tumour is not diagnostic of EST.
-
A panel of antibodies rather than a single antibody should be used when interpreting mesenchymal tumours of the uterus.
-
The most useful panel includes CD10 and two smooth muscle markers.
-
Diffuse or multifocal and strong positivity for two muscle markers favours a smooth-muscle nature of the tumour despite CD10 positivity.
-
Immunohistochemical results should always be correlated with the histological appearance of the tumour and interpreted accordingly, as ESTs may show areas with different types of differentiation.
REFERENCES
Footnotes
-
Competing interests: None declared.