Article Text

Abstract
The diagnosis of drug-induced liver injury (DILI) is a challenging problem, often confounded by incomplete clinical information and the difficulty of eliciting exposure to herbal products, over-the-counter agents and toxins. The task is further rendered difficult on biopsy, as drugs can mimic all the patterns found in primary liver disease. Acute hepatitis, with or without cholestasis, is the most common histological pattern of DILI, and drugs such as acetaminophen are the leading causes of acute liver failure. Most cases of DILI resolve on discontinuation of the drug, but recovery can take months or rarely the disease can progress despite drug withdrawal. Drugs such as methotrexate can lead to chronic hepatitis and cirrhosis, while others such as minocycline, nitrofurantoin and methyldopa are implicated in autoimmune hepatitis. Prolonged cholestasis and ductopenia resembling primary chronic biliary disease can occur. Drug-induced steatohepatitis is also an uncommon pattern, but is well described with drugs such as amiodarone and irinotecan. In the presence of risk factors such as obesity and diabetes, some drugs such as tamoxifen, oestrogens and nifedipine can precipitate or exacerbate steatohepatitis. Other observed patterns include granulomatous hepatitis, vascular injury (eg, sinusoidal obstruction syndrome), Ito cell lipidosis and neoplasms (eg, adenomas).
Statistics from Altmetric.com
Box 1 Drugs associated with acute hepatitis pattern of injury
Non-steroidal anti-inflammatory drugs
Diclofenac*, indomethacin, tolmetin, sulindac, ibuprofen, ketoprofen, mefenamic acid, celecoxib
Anaesthetic agents
Halothane,7 methoxyflurane
Anticonvulsants
Phenytoin, carbamazepine*, valproic acid, chlorpromazine*
Antibacterial agents
Ampicillin, amoxicillin–clavulanic acid,5 8 9 oxacillin, cephalosporins, tetracycline, sulfonamides, erythromycin, trimethoprim–sulfamethoxazole*
Antifungal agents
Griseofulvin, fluconazole, ketoconazole*
Antiparasitic agents
Albendazole, thiabendazole, fansidar
Antituberculous agents
Isoniazid, rifampin
Antiviral agents
Zidovudine, ribavirin, nevirapine*, efavirenz*
Antitumour agents
6-Mercaptopurine, azathioprine, l-asparaginase, mithramycin, vincristine, cyclophosphamide, carmustine
Antihypertensive agents
Methyldopa, hydralazine, lisinopril, labetalol
Antiarrhythmic agents
Quinidine, nifedipine, procainamide
Hypolipidaemics
Statins, clofibrate, nicotinic acid, ezetimibe*
Hypoglycaemics*
Rosiglitazone, troglitazone
Antiandrogens*
Flutamide
Other
Sulfonylureas, troglitazone, dantrolene, chlorzoxazone, dextropropoxyphene, allopurinol, gold
Toxins
Aflatoxin, death cap mushroom (Amanita phalloides), carbon tetrachloride, ethylene dichloride, allyl compounds, ferrous sulfate, phosphorus, MDMA (ecstasy)
*Primarily cholestatic pattern
Box 2 Drugs implicated in granulomatous hepatitis
Antimicrobials
Isoniazid, penicillin, sulfonamides, cephalexin, dapsone, dicloxacillin, oxacillin, interferon
Anticonvulsants/antipsychotic agents
Phenytoin, diazepam, chlorpropamide, chlorpromazine, procarbazine, carbamazepine
Others
Allopurinol, gold, procainamide, quinidine, methyldopa, diclofenac, diltiazem, BCG therapy for cancer, nitrofurantoin, mesalamine, phenylbutazone (veterinary use, use in humans limited due to side effect of aplastic anaemia)78
Evaluation of liver biopsy for adverse drug reaction is one of the most challenging problems in liver pathology. Drug-related injury can mimic all the patterns observed in primary liver disease, and an unequivocal histological diagnosis is not possible in the majority of cases. Inadequate clinical history and multiple drugs being taken simultaneously often compound the problem. It can be difficult to elicit information about herbal agents, over-the-counter medications, and exposure to household or industrial toxins. The list of drugs associated with hepatotoxicity is long, although the association of many drugs with liver injury remains tenuous and can be found only in case reports.
Mechanisms of injury
It is widely recognised that drug-induced liver injury (DILI) is mediated by two chief mechanisms: intrinsic and idiosyncratic hepatoxicity. Intrinsic hepatotoxins cause hepatocellular damage in a predictable dose-dependent manner directly by the drug or indirectly by its metabolite. Some drugs, such as acetaminophen, cause intrinsic hepatotoxicity, but the majority of agents in this category are industrial, household or environmental toxins such as carbon tetrachloride and alkaloids in mushrooms. The majority of drugs lead to idiosyncratic liver injury and can be classified into metabolic and immunological categories. In the former, the drug is metabolised into a toxic metabolite in predisposed individuals, while the latter is akin to “drug allergy” or hypersensitivity following sensitisation to the drug. In general, intrinsic hepatotoxicity manifests with hepatocellular necrosis with little inflammation, while idiosyncratic drug reactions often show inflammation-dominant hepatic injury.
Establishing drug as the causative agent
The temporal profile is crucial to establish the diagnosis of DILI, as the onset of liver disease follows drug ingestion. However, the manifestation of liver toxicity may occur weeks or months after drug ingestion and even after the drug has been stopped. Liver enzyme elevations can persist for up to several months after the drug has been discontinued. In some instances, measurement of serum levels of the drug or its metabolite can be helpful in diagnosis, such as in acetaminophen toxicity. Since the list of drugs capable of causing liver injury is long, a systematic literature search for each drug that the patient has been taking is necessary. The case for DILI is strengthened if the reported pattern of injury in the literature is in keeping with the observed clinical and histological picture. Rechallenge with the drug can help establish the drug aetiology, but it is often not done due to the inherent risk involved. Since diverse histological patterns of DILI can mimic virtually any primary liver disease, appropriate imaging and laboratory tests are necessary to exclude other aetiologies before the diagnosis of DILI can be accepted.
Liver injury can be classified as hepatocellular, cholestatic or mixed, based on criteria established by the Council for International Organizations of Medical Sciences (CIOMS)1 2 (table 1).
The CIOMS system also is used for causality assessment of DILI by scoring parameters such as time to onset of symptoms, laboratory data, additional drug regimen, known toxicity of suspected drug, non-drug causes, and response to rechallenge. The total score is categorised into ranges of causality: highly probable, probable, possible, unlikely and excluded.3–5 The remaining discussion is devoted to the patterns observed in DILI with emphasis on morphological features, common drugs and differential diagnosis for each pattern (table 2).
Acute hepatitis
DILI accounts for ∼10% of acute hepatitis and is perhaps the most common cause of cholestatic hepatitis.6 A wide variety of drugs can cause acute hepatocellular injury (box 1).
Herbal and botanical drugs are an important but often overlooked cause of hepatotoxicity (table 3).
These are not regulated by the Food and Drug Administration and hence are not subject to rigorous testing. More than 20 000 herbal products are marketed in forms including powders, essential oils and teas, and more than $5 billion are spent on these annually. Nearly 20% of American adults have used herbal remedies, and usage is higher in selected groups including Chinese,20 South African21 and Native American22 cultures. Definitive identification of an herbal product can require chemical analysis, as mistranslation or misidentification can be an issue. Eliciting a detailed herbal history is imperative.23 Certain commonly consumed herbal agents now being investigated for their hepatoprotective effects, such as turmeric (Curcuma longa)24 and mate tea (Ilex paraguariensis),25 are listed as potentially hepatotoxic in various patient literature. Finally, contaminants of herbal supplements should be considered, including heavy metals such as arsenic, cadmium, lead or mercury.26
The following morphological patterns can be observed in acute hepatocellular injury.
Acute hepatitis. The hallmarks of acute hepatocellular injury are portal and parenchymal inflammation, hepatocellular injury, and/or necrosis (fig 1). By definition, fibrosis is absent. Regenerative features such as binucleate hepatocytes and thick cell plates are common. Prominent Kupffer cells often are present in the sinusoids. The term “cholestatic hepatitis” is used when these changes are accompanied by cholestasis (see Acute cholestatic injury).
Necrosis. Acute hepatocellular injury can result in necrosis affecting single (spotty necrosis) or groups of hepatocytes (confluent necrosis). In some cases, confluent necrosis can be zonal and may be helpful in diagnosis. Centrizonal (zone 3) necrosis is characteristic of acetaminophen and halothane, and toxins such as carbon tetrachloride. Isolated necrosis affecting zones 1 and 2 is rare; toxins such as cocaine and ferrous sulfate typically affect zone 1, while beryllium has been implicated in zone 2 necrosis. When extensive, confluent necrosis can lead to acute hepatic failure.
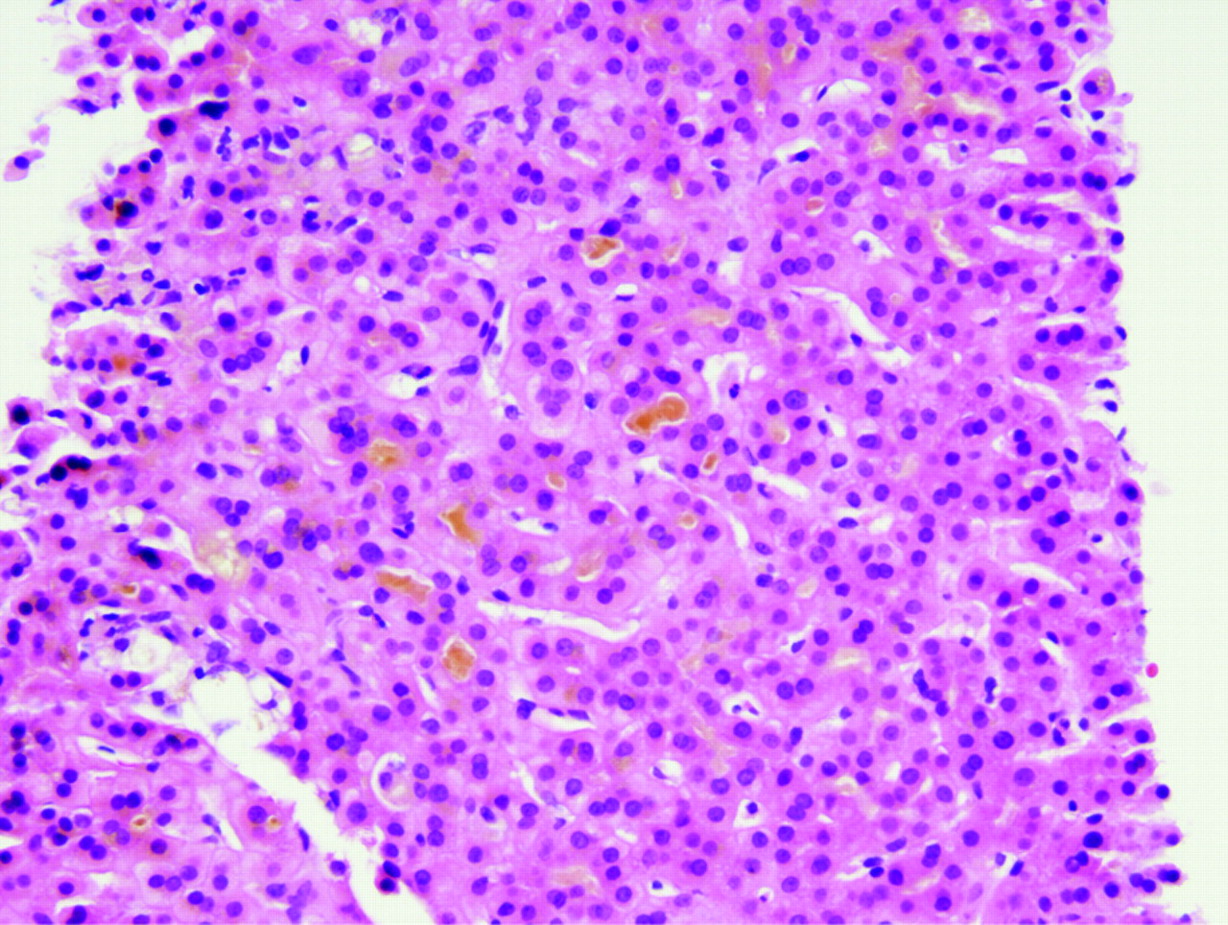
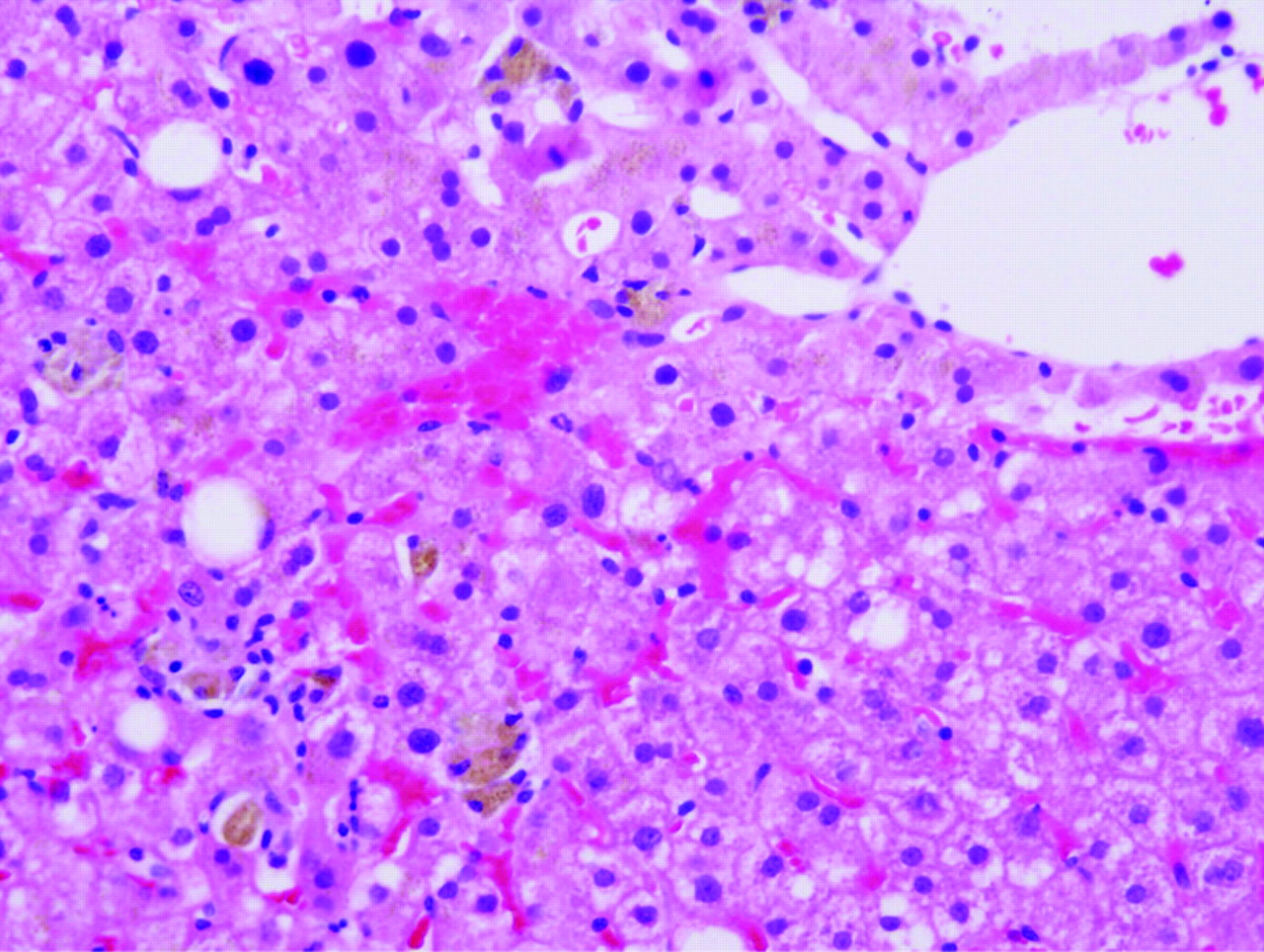
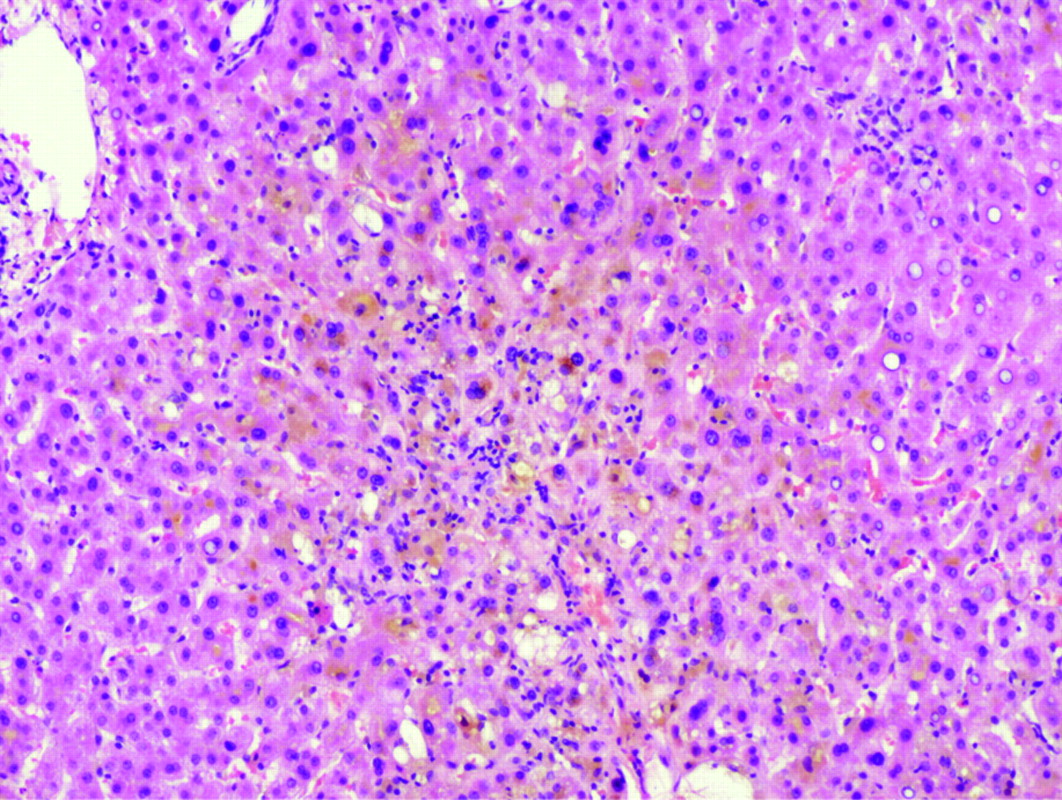
Resolving hepatitis. If biopsy is performed later in the disease course, hepatocellular injury and inflammation may be minimal (fig 2). The presence of numerous macrophages in the sinusoids is a helpful clue for the diagnosis of resolving hepatitis. The stain periodic acid–Schiff with diastase can be used to highlight the macrophages (fig 3).

Atorvastatin-induced acute hepatitis. Mixed parenchymal inflammation is present, consisting of lymphocytes, plasmahistiocytic cells, and neutrophils. There is no bile duct damage or fibrosis. H&E, ×200.
Resolving hepatitis. Parenchymal infiltrate is diminished in comparison to acute hepatitis. Hepatocellular injury is minimal. Pigment accumulation in sinusoidal macrophages is prominent. H&E, ×200.

Resolving hepatitis. Sinusoidal macrophages are evident with periodic acid–Schiff (PAS)-positive diastase-resistant cytoplasmic contents. PAS with diastase, ×200.
Differential diagnosis
The histological features can be indistinguishable from other causes of acute hepatitis such as acute viral hepatitis, initial presentation of autoimmune hepatitis and Wilson disease. The presence of bile duct injury, prominent eosinophilic infiltrate, granulomas, sharply defined perivenular necrosis, or cholestasis out of proportion to hepatocellular injury, favours adverse drug reaction, but none of these features is specific.
Acute liver failure (fulminant hepatitis)
Acute liver failure (ALF) is defined as the onset of hepatic encephalopathy within 8 weeks of onset of symptoms. Drugs are the most common cause of ALF in the USA, accounting for 25–50% of cases.27–30
Based on morphological features, ALF can be subdivided into three categories.
Extensive microvesicular steatosis. This pattern is rare and has been observed with tetracycline and nucleoside analogues such as zidovudine (see Steatosis and steatohepatitis).
Necrosis with marked inflammatory activity. This is the most common pattern seen in idiosyncratic adverse drug reactions. It is similar to the acute hepatitis pattern discussed above except that the confluent necrosis involves most of the liver parenchyma (massive/submassive hepatic necrosis). The most commonly implicated drugs are isoniazid,31 32 other antimicrobial agents (sulfonamides, cotrimoxazole, ketoconazole), monoamine oxidase inhibitors, and anticonvulsants (phenytoin,31 valproate). Any drug that causes acute hepatitis can potentially cause ALF.
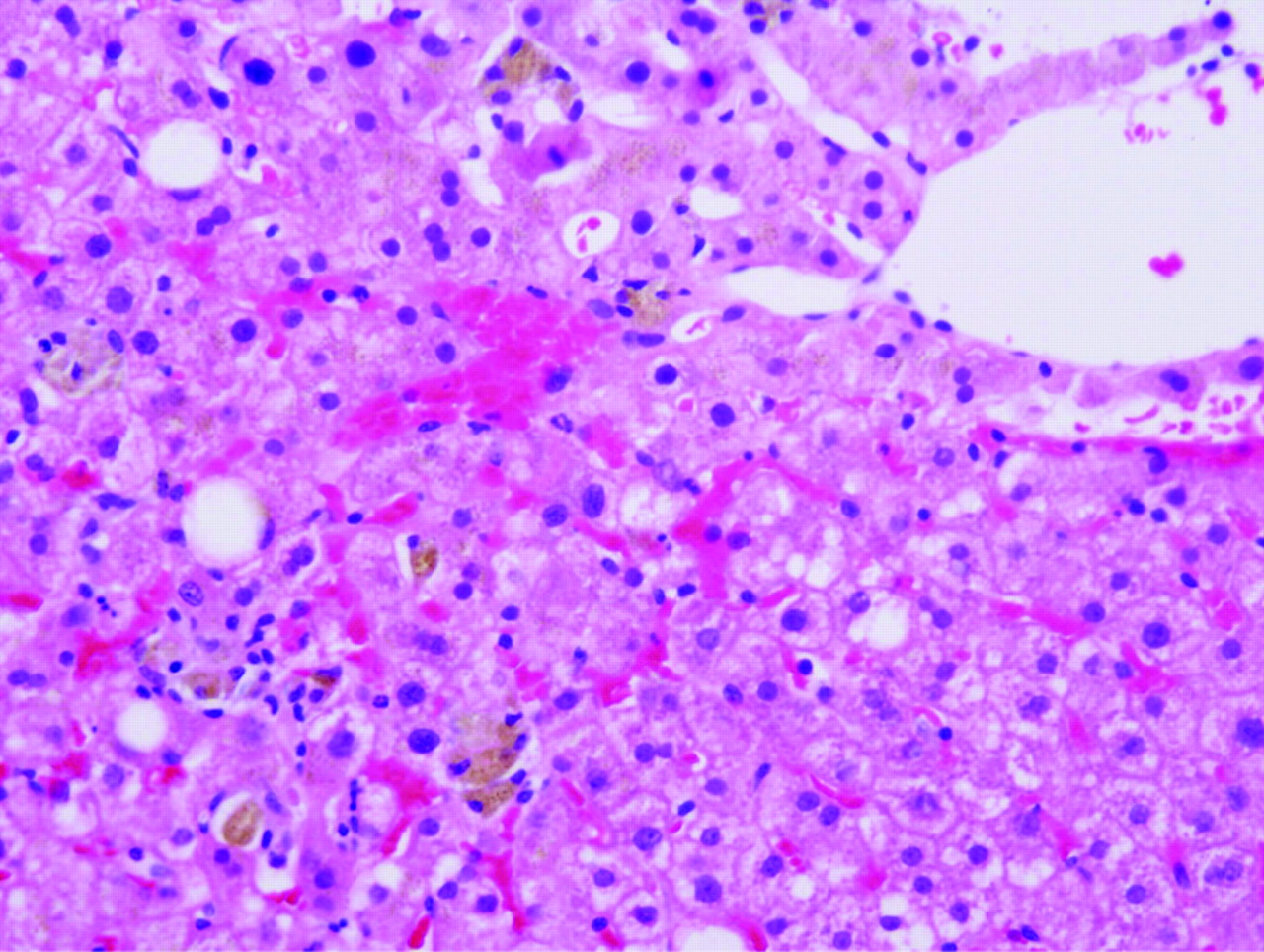
Necrosis with little or no inflammation. This pattern is seen with acetaminophen (fig 4), recreational drugs such as cocaine and 3,4-methylenedioxymethylamphetamine (MDMA; ecstasy), industrial organic compounds such as carbon tetrachloride, and some herbal preparations. Necrosis can be accompanied by steatosis.

Acetaminophen toxicity. Marked hepatocellular necrosis is present in a zonal, centrilobular pattern, while the inflammatory infiltrate is minimal. Residual viable hepatocytes show some steatosis. H&E, ×100. (Image courtesy of Dr Linda Ferrell, University of California, San Francisco, California, USA.)
Acetaminophen
Acetaminophen toxicity is the leading drug-related cause, implicated in nearly 40% of ALF, the remaining being attributed to idiosyncratic drug reactions.27–29 33 Acetaminophen is a very safe drug within its therapeutic window (3–4 g/day), but can cause dose-dependent toxicity with overdose whether accidental (1/3 of cases) or with suicidal intent (2/3 of cases). At low doses, the drug is conjugated to water-soluble metabolites in the liver and is excreted in the urine. At higher doses, glutathione depletion leads to saturation of the conjugation mechanism, leaving the parent compound to be metabolised to toxic intermediates. The minimum toxic dose in adults is 7.5–10 g, but severe liver damage occurs with ingestion of 15–25 g. Acetaminophen blood levels taken 4–16 h after ingestion are the best predictor of outcome. Chronic alcohol consumption, obesity, and drugs that induce the P-450 cytochrome system, such as isoniazid, phenytoin, carbamazepine or cimetidine, can lower the toxic threshold of acetaminophen.
Patients typically experience gastrointestinal symptoms for the first 12–24 h and a latent phase at 24–48 h. The onset of acute hepatitis/acute liver failure occurs 72–96 h after drug ingestion. Hepatotoxicity can be prevented with early presentation and institution of acetyl-cysteine therapy within 12 h. The highest mortality is encountered in late presenters.
Chronic hepatitis
Chronic liver disease typically refers to persistent biochemical abnormalities beyond 6 months.34 In some series, the cut-off of 3 months has been used for hepatocellular injury and 6 months for cholestatic or mixed injury.35 Progression to chronicity has been reported in 5–10% of adverse drug reactions and is higher for the cholestatic/mixed injury pattern.36 Histologically proven drug-induced chronic hepatitis with fibrosis is a rare phenomenon. Some specific patterns and clinicopathological situations are discussed below.
Chronic hepatitis with negative autoimmune markers
The histological features are indistinguishable from chronic viral hepatitis, and progression to fibrosis and even cirrhosis can occur. The features of acute hepatitis may be seen to a variable degree. Drugs associated with this pattern include lisinopril (antihypertensive), sulfonamide (antibiotic), trazodone (antidepressant), and chemotherapeutic agents such as uracil, 5-fluorouracil prodrug tegafur and tamoxifen. Isolated case reports implicate numerous other drugs including phenytoin37 and the Chinese herb Jin bu huan.38 Progression to fibrosing cholestatic hepatitis has been reported in a hepatitis C patient after administration of cyclophosphamide and corticosteroids for glomerulonephritis.39 Discontinuation of the drug may lead to a favourable outcome, but if the fibrosis is advanced the resolution may be slow or the disease may progress.
Autoimmune hepatitis
Several drugs can cause chronic hepatitis that is serologically and morphologically indistinguishable from de novo autoimmune hepatitis (AIH). The hepatic disease may be accompanied by features of hypersensitivity such as rash, arthralgia and peripheral eosinophilia.
Minocycline
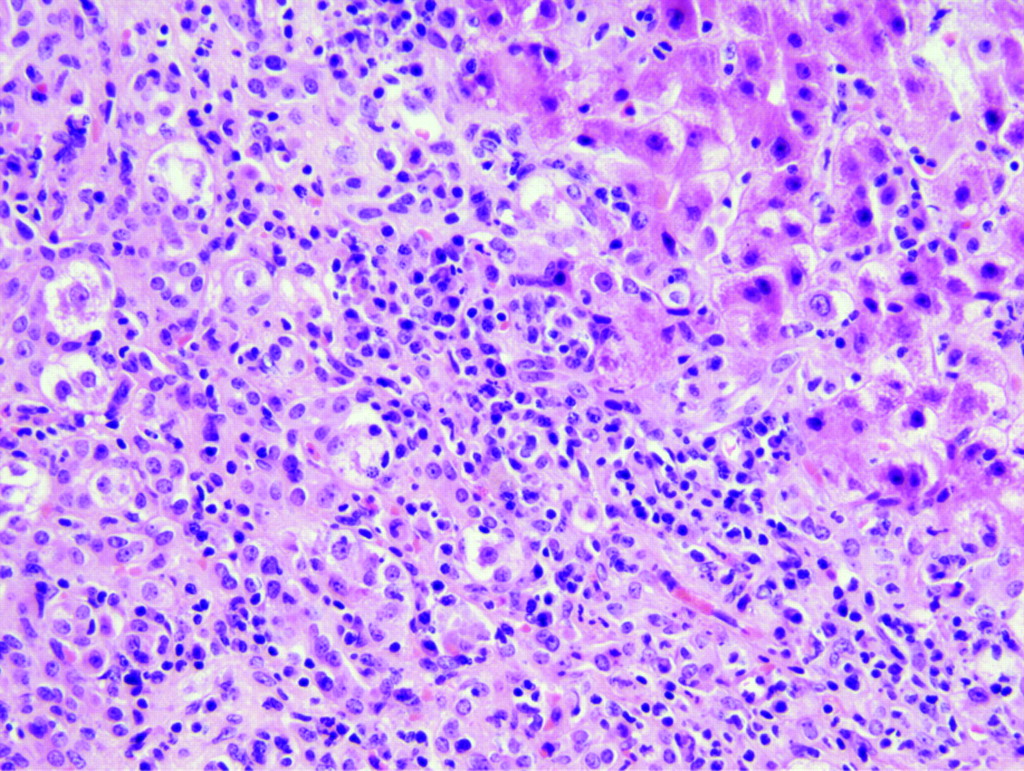
Long-term use of minocycline, a synthetic tetracycline for treatment of acne, can lead to hepatitis that can mimic lupus-related hepatitis, AIH or overlap syndrome. Autoimmune disease can develop within days of starting the drug or may be delayed for many years. High titres of antinuclear antibodies (ANAs) are common, but smooth muscle (SMA) and other autoantibodies often are negative. Autoimmune markers may be elevated in chronic hepatitis due to drugs (drug-induced autoimmune hepatitis). Inflammatory activity can be minimal to mild, and eosinophils are typically inconspicuous (fig 5). Marked fibrosis and cirrhosis are rare, and patients often improve after drug withdrawal.40 Microvesicular and macrovesicular steatosis in response to minocycline have been reported, but these followed high-dose intravenous therapy rather than oral administration.41

Minocycline-induced autoimmune hepatitis. Marked necroinflammatory activity with numerous plasma cells. H&E, ×200.
Nitrofurantoin
Nitrofurantoin is used to treat urinary tract infections. The hepatic injury can manifest as self-limited acute hepatitis, chronic hepatitis, and rarely as hepatic failure.42 Chronic hepatitis can be indistinguishable from de novo AIH and is often associated with ANA and SMA.43 Discontinuation of the drug generally leads to clinical and biochemical improvement. In some cases, the disease may progress despite drug withdrawal. In contrast to minocycline, significant fibrosis and cirrhosis can occur.
Others
Other drugs implicated in AIH include methyldopa (antihypertensive)44 and clometacin non-steroidal anti-inflammatory drug (NSAID).45 Antibodies to liver-kidney-microsomal antibodies, akin to type 2 AIH, have been described in hepatitis related to hydralazine (antihypertensive) and tienilic acid (ticrynafen, a diuretic withdrawn from the American market), but this association is not clearly defined.46
Methotrexate
Methotrexate is a folate antagonist that is used for long-term treatment of rheumatoid arthritis, psoriasis and inflammatory bowel disease. The canals of Hering may be the target of methotrexate-related scarring.47 The risk of liver toxicity is exacerbated with heavy alcohol use, pre-existing liver disease, daily dosing and high cumulative dose.48 Minor elevation in liver enzymes occurs in 20–50% of patients but does not necessarily imply significant toxicity.
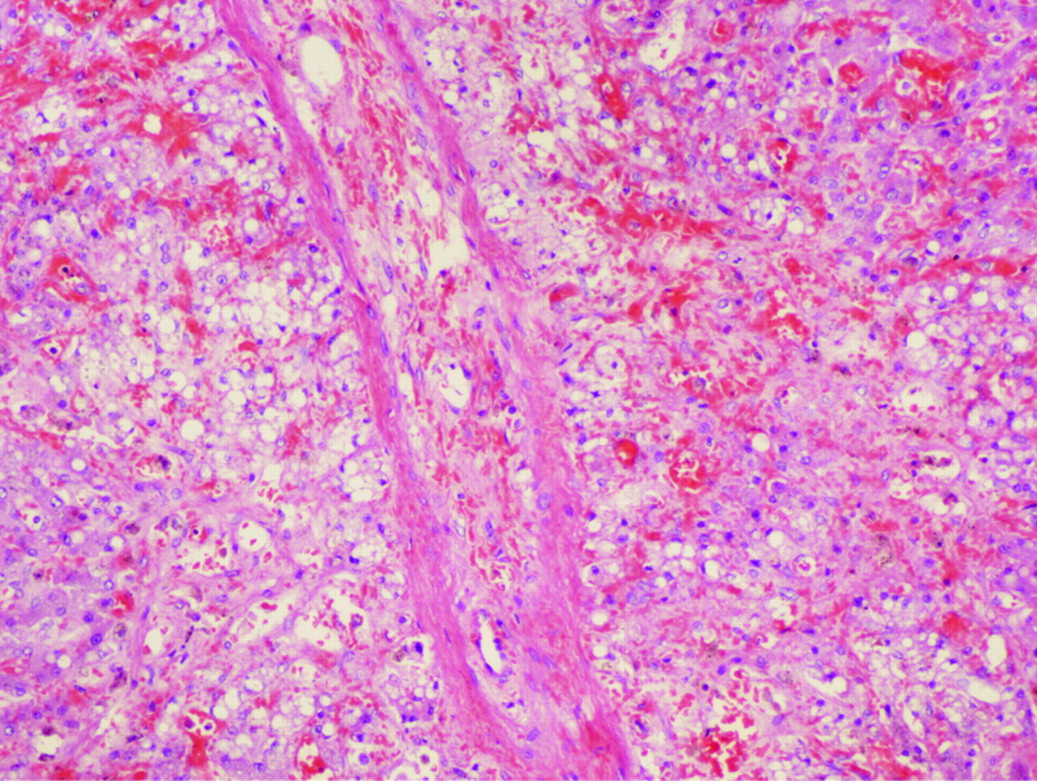
The histological features of methotrexate-related toxicity range from minor fatty change, hepatocyte anisonucleosis, mild portal-based inflammation, and focal necrosis to more severe hepatocellular necrosis, fibrosis and cirrhosis (fig 6). Methotrexate may exacerbate or precipitate steatohepatitis in patients with risk factors such as obesity and diabetes. Some patients with high cumulative dose can have steatohepatitis-like histology without other risk factors.49
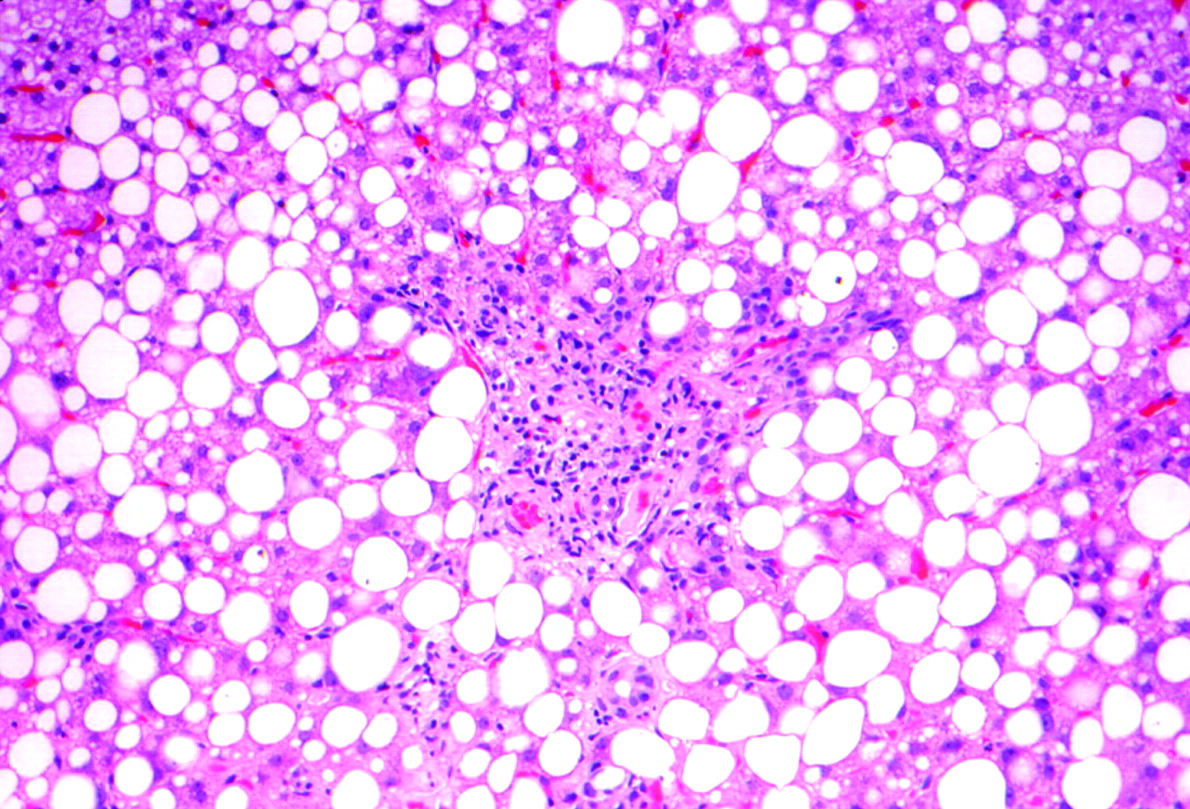
Methotrexate toxicity. Prominent macrovesicular steatosis and periportal fibrosis. H&E, ×100. (Image courtesy of Dr Linda Ferrell, University of California, San Francisco, California, USA.)
Patients on long-term methotrexate need close monitoring. Liver biopsy is necessary in patients who develop deranged liver function following methotrexate therapy. A grading scheme has been proposed to assess toxicity (Roenigk classification50–52; table 4).
Acute cholestatic injury
Drug-induced cholestatic injury can manifest clinically with jaundice, pruritus, dark urine and pale stools. Liver enzyme studies typically reveal elevation of alkaline phosphatase and γ-glutamyl transferase. Transaminases can be variably elevated. A Danish study of 1100 cases of drug-associated injury reported 16% with the acute cholestatic pattern.53
The histological patterns of injury can be divided into two forms. (1) Pure (bland) cholestasis in which bile plugs are seen in hepatocytes or canaliculi and are most prominent in zone 3. Inflammation and hepatocellular injury are not observed. This pattern is typically observed with anabolic steroids (fig 7) and oral contraceptives. Other drugs that have been incriminated include prochlorperazine, thiabendazole54 and warfarin. (2) Cholestatic hepatitis in which the cholestasis is accompanied by inflammation and hepatocellular injury. Bile ductular reaction may be present. This pattern also has been referred to as cholangiolitic or hypersensitivity cholestasis.55 This pattern manifests as mixed-type injury on liver biochemical tests. Cholestatic hepatitis can result from a wide variety of drugs; it is the classic pattern seen with toxicity due to macrolide antibiotics such as erythromycin56 (fig 8) and the antipsychotic agent chlorpromazine (see box 1).
Anabolic-steroid-induced pure cholestasis. Prominent bile plugs are present in hepatocytes and canaliculi without inflammation or hepatocellular damage. H&E, ×200.

Erythromycin-related cholestatic hepatitis. Features similar to acute hepatitis are present, as well as bile plugs in hepatocytes and canaliculi. H&E, ×100.
Differential diagnosis
Drug-induced cholestatic injury can be histologically indistinguishable from obstructive biliary disease. While the latter typically results in portal tract oedema and ductular reaction with inflammation, cholestasis may be the only significant feature in early stages. Drug-induced cholestatic hepatitis also needs to be distinguished from autoimmune hepatitis and acute viral hepatitis.
Bland cholestasis can occur in several systemic disorders such as sepsis, cardiac failure and shock, and hence clinical information is necessary to establish the aetiology. In the appropriate clinical setting, benign recurrent intrahepatic cholestasis, postoperative cholestasis and intrahepatic cholestasis of pregnancy have to be considered. Benign recurrent intrahepatic cholestasis is a mild, non-progressive variant of bile transporter disorder characterised by intermittent episodes of cholestasis.57 Intrahepatic cholestasis of pregnancy also is due to bile transporter gene variation, although it additionally appears affected by hormonal status, as twin pregnancies and patients on oral contraceptives are reported to be more susceptible to intrahepatic cholestasis of pregnancy.58
Chronic biliary diseases such as primary biliary cirrhosis and primary sclerosing cholangitis do not show cholestasis on biopsy early in the course of the disease; serological tests such as antimitochondrial antibodies and cholangiography, respectively, can more definitely rule out these diagnoses.
Chronic cholestasis and ductopenia
Cholestatic symptoms and biochemical findings usually resolve with cessation of the offending drug but may persist in some instances. Drugs causing prolonged cholestasis (defined as greater than 3 months in duration)1 59 and ductopenia include antibiotics such as amoxicillin–clavulanic acid60 61 and flucloxacillin,62 63 antifungals such as terbinafine64 and, rarely, oral contraceptives.65 Amiodarone can also cause prolonged disease.66
Vanishing bile duct syndrome
Cholestasis with variable degree of inflammation, bile duct injury and hepatocellular damage is seen early in the course of the disease (fig 9). If the disease persists for a few months or beyond, loss of bile ducts and overt ductopenia may be observed, termed “vanishing bile duct syndrome”. Persistent inflammation and bile ductular reaction also may be present. Rare cases can progress to cirrhosis. Vanishing bile duct syndrome can be triggered by anticonvulsants such as carbamazepine67 and zonisamide,68 antipsychotics such as chlorpromazine69 and sulpiride,70 NSAIDs such as ibuprofen71 72 and tenoxicam,73 and antibiotics such as amoxicillin,74 flucloxacillin,75 clindamycin and trimethoprim-sulfamethoxazole.76 The histological picture can mimic primary biliary cirrhosis or obstructive biliary disease. Absence of antimitochondrial antibodies and normal imaging of the biliary tree help in establishing drug-related aetiology.
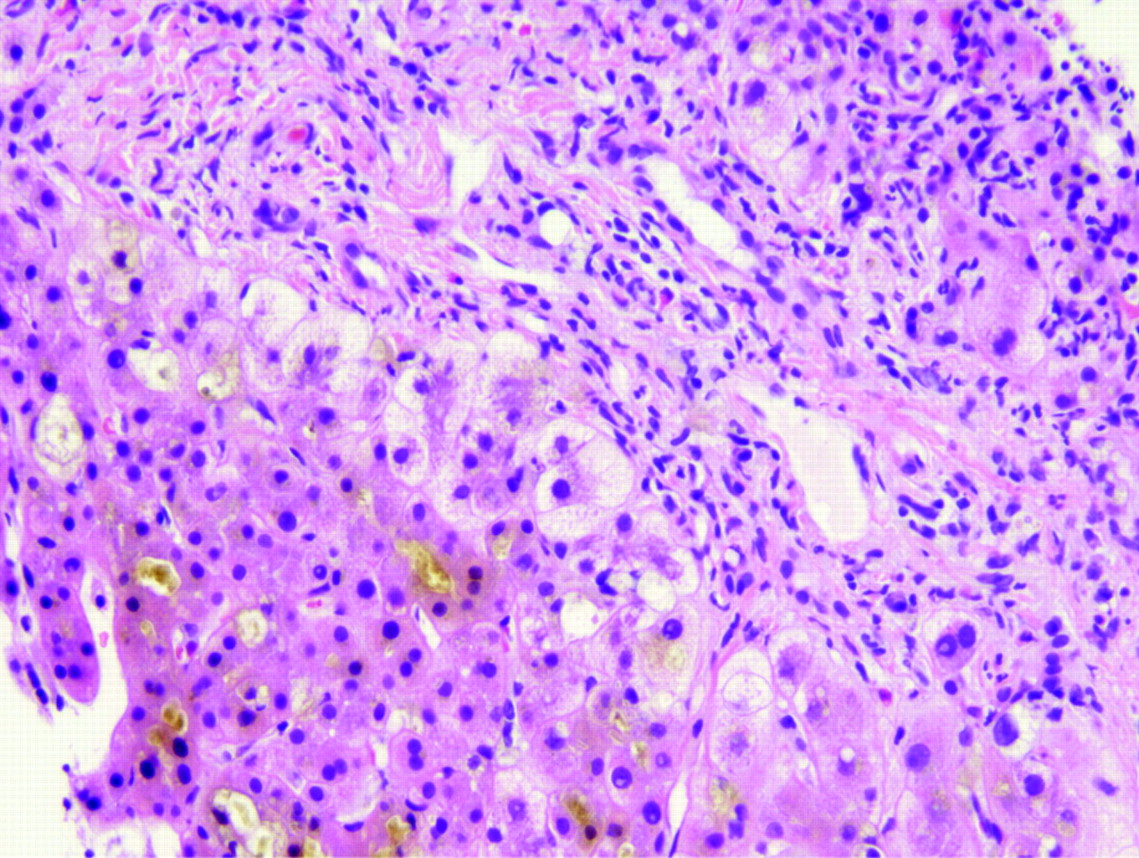
Prolonged cholestasis. Persistence of canalicular bile plugs accompanied by feathery degeneration of periportal hepatocytes (cholate stasis). H&E, ×200.
Other patterns
Biliary sclerosis can result from intra-arterial infusion of 5-fluorodeoxyuridine for treatment of hepatic metastasis of colorectal carcinoma.77 Ischaemic injury to the large intrahepatic and extrahepatic bile ducts can lead to strictures that resemble primary sclerosing cholangitis radiologically and histologically. Similar injury can occur with other agents such as formaldehyde and sodium chloride injected into hydatid cysts.
Granulomatous hepatitis
The most common causes of granulomas in the liver are infections, sarcoidosis, primary biliary cirrhosis and drugs (box 2).
Granulomas are uncommon in hepatitis C but can occur in patients treated with interferon. Talc granulomas can occur in intravenous drug users and can be detected by viewing under polarised light. Other systemic granulomatous disease such as chronic metal toxicity (such as beryllium or copper) can also involve the liver.55 Finally, a study of granulomatous hepatitis cases over a 13-year period identified 11% as idiopathic.79 These cases can present with fever of unknown origin and generally respond favourably to steroids.
The granulomas can be present in the portal tracts or the parenchyma and lack necrosis. Unlike in primary biliary cirrhosis, the granulomas are not centred on the bile ducts. Granulomas also can occur with other patterns of liver injury such as acute hepatitis, cholestasis or steatosis.
The term fibrin-ring granuloma has been used for small granulomas that consist of a ring of fibrin arranged around a central fat vacuole (fig 10). Epithelioid histiocytes are present around the ring of fibrin. In atypical cases, the fibrin is intermixed with the histiocytes and does not form a well-defined ring. More typical granulomas without the fibrin ring generally are present in other areas of the biopsy. Fibrin-ring granulomas have been described with allopurinol, BCG vaccination and intravesical therapy for carcinoma. These granulomas were first described in the rickettsial disease Q fever (Coxiella burnetti) but also occur in boutonneuse fever (Rickettsia conorii), leishmaniasis, toxoplasmosis, cytomegalovirus infection and Hodgkin lymphoma.

Fibrin-ring granulomas. Fat vacuole surrounded by a ring of fibrin deposition and epithelioid cells. H&E, ×200.
Steatosis and steatohepatitis
Macrovesicular steatosis
Macrovesicular steatosis includes large and small droplet fat. The term “large droplet fat” is used when at least half the hepatocyte cytoplasm is occupied by a single lipid vacuole, while multiple lipid vacuoles are seen in small droplet fat. The latter often is confused with true microvesicular steatosis which, unlike small droplet fat, affects the liver in a diffuse fashion (see below). Macrovesicular steatosis can be seen in association with steroids,80 nitrofurantoin, gold, methotrexate, NSAIDs such as ibuprofen, indomethacin and sulindac, and antihypertensives such as metoprolol, chlorinated hydrocarbons such as carbon tetrachloride and chloroform,81 or chemotherapeutic agents such as 5-fluorouracil, cisplatin and tamoxifen.82
Microvesicular steatosis
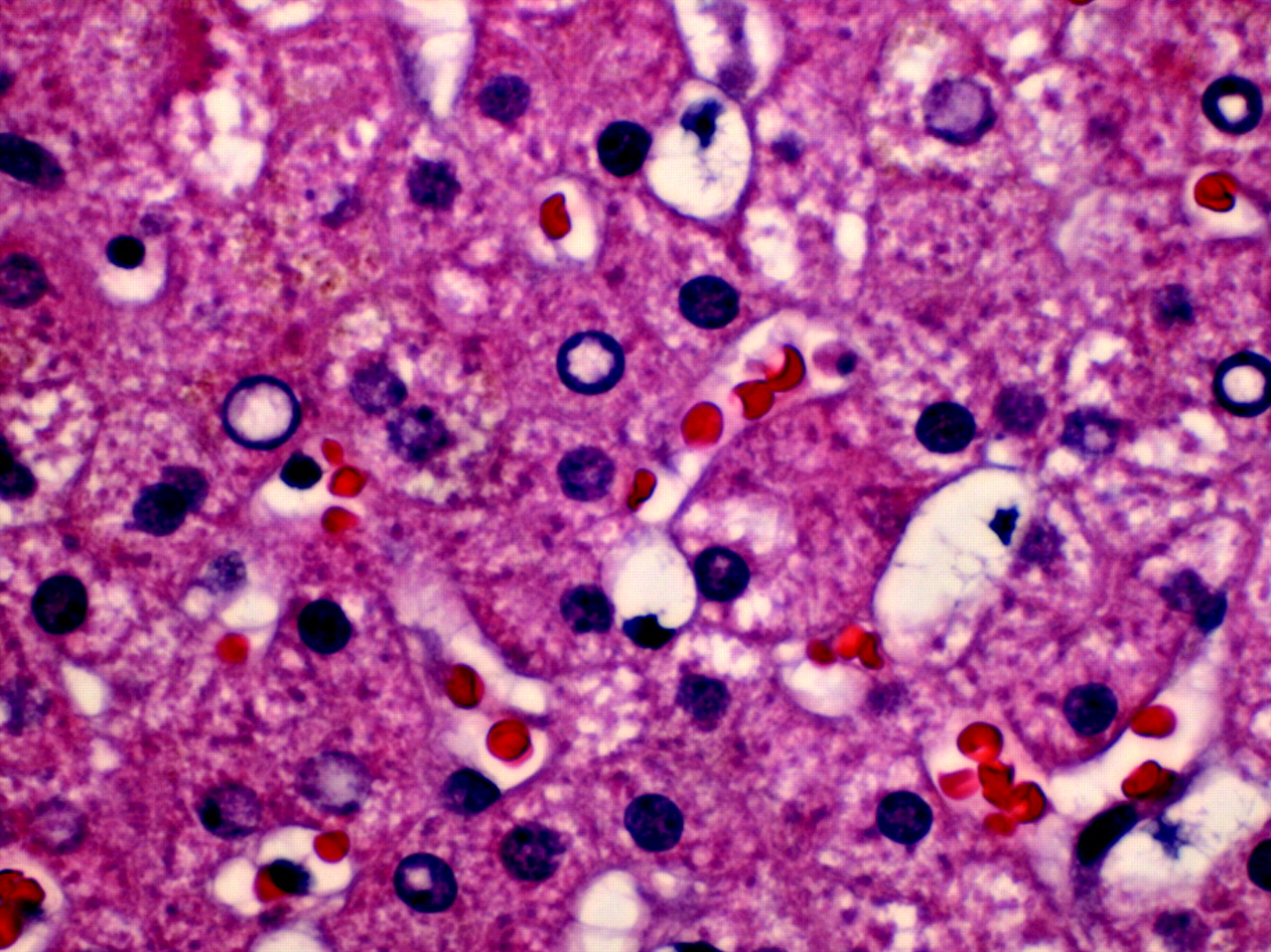
Exclusive or predominant microvesicular steatosis diffusely affecting the liver is a result of mitochondrial injury and often occurs as an adverse effect of drugs/toxins such as cocaine, tetracycline, valproic acid and zidovudine (fig 11). Acute exposure to alcohol (alcohol foamy liver degeneration)83 and paediatric Reye syndrome also show diffuse microvesicular steatosis.84 Other non-drug related aetiologies include acute fatty liver of pregnancy and genetic diseases such as carnitine deficiency.

Microvesicular steatosis. Numerous small lipid droplets are present throughout the hepatocytic cytoplasm. H&E, ×400.
Steatohepatitis
By definition, steatohepatitis is characterised by steatosis, lobular inflammation and hepatocellular injury in the form of hepatocellular ballooning (with or without acidophil bodies or Mallory hyaline) or pericellular fibrosis. A few drugs (notably amiodarone and irinotecan) play a direct aetiological role in steatohepatitis. Most other drugs exacerbate or precipitate steatohepatitis in the presence of other risk factors such as obesity and diabetes.
Amiodarone
Amiodarone, a potent antiarrhythmic agent, causes elevated liver enzymes in up to 30% of patients85 86 and steatohepatitis in 1–2%87 of patients. The majority of cases display liver enzyme abnormalities within 24 h of intravenous infusion.88 Even low oral dosing (200 mg daily) may trigger steatohepatitis with cumulative use.89 Occasionally, jaundice is the major clinical presentation. These cases often show hepatocellular necrosis and fibrosis, and have a poor prognosis.66
Amiodarone steatohepatitis is characterised by prominent Mallory hyaline (occasionally in zone 1) and neutrophilic satellitosis, while steatosis is less conspicuous (fig 12). The findings can be similar to alcoholic steatohepatitis. Reversal of liver injury often occurs with discontinuation of the drug but may be delayed by weeks or months. In addition, amiodarone is also associated with a different type of lipid accumulation called “phospholipidosis” characterised by accumulation of drug in the lysosomes.90 91 This leads to “foamy” appearance of hepatocytes and Kupffer cells. The foamy areas show lamellar lysosomal inclusion bodies on electron microscopy92 (fig 13). Phospholipidosis is not always seen in amiodarone toxicity90 and is independent of steatohepatitis.93

Amiodarone steatohepatitis. Marked hepatocyte ballooning, numerous Mallory hyaline and minimal steatosis. H&E, ×100.

Phospholipidosis. Formation of lysosomal inclusion bodies due to accumulation of amiodarone. Electron micrograph. (Image courtesy of Dr Linda Ferrell, University of California, San Francisco, California, USA.)
Perhexiline maleate (Pexid), an antianginal drug, and diethylaminoethoxyhexestrol (Coralgil), a vasodilator, have been used extensively in Europe and Japan, respectively. Both drugs can cause steatohepatitis and phospholipidosis similar to amiodarone.94 95
Chemotherapy-induced steatohepatitis
Steatosis and steatohepatitis have been reported with chemotherapeutic agents. The latter especially is associated with irinotecan, a drug often used preoperatively in colorectal cancer with hepatic metastases. This has been referred to as chemotherapy-associated steatohepatitis in the oncology literature.82 96 Other chemotherapeutic agents such as oxaliplatin have been variably implicated.82 97
Others
Drugs such as tamoxifen, steroids, oestrogen and diethylstilbestrol often lead to hepatic steatosis, but steatohepatitis is rare. These drugs may exacerbate or precipitate steatohepatitis in patients with risk factors for steatohepatitis rather than play an aetiological role. The evidence linking steatohepatitis and calcium channel blockers such as nifedipine also is anecdotal. Risk factors for steatohepatitis were present in many reported cases, creating uncertainty about the association of these drugs with steatohepatitic injury.98
Vascular abnormalities
Several vascular patterns of injury are recognised, each with distinctive morphological features and drug associations.
Sinusoidal obstruction syndrome
Sinusoidal obstruction syndrome (SOS; veno-occlusive disease) is due to endothelial cell injury to small hepatic venules that manifests histologically as endothelial swelling and thrombosis (fig 14). The resultant venous outflow obstruction leads to sinusoidal dilatation, congestion, hepatocellular necrosis, and can result in centrilobular fibrosis.

Sinusoidal obstruction syndrome. Endothelial injury in small hepatic venules leads to luminal occlusion due to endothelial swelling and thrombosis, and results in sinusoidal dilatation and congestion. H&E, ×100.
Cytotoxic/chemotherapeutic drugs such as oxaliplatin (used in colorectal cancer) can cause injury to sinusoidal endothelial cells and hepatic stellate cells.97 99 100 SOS can also occur due to myeloablation before stem cell transplantation, chemotherapy for acute lymphocytic leukaemia, bone marrow transplantation101 and pyrrolizidine alkaloids.97 Genetic polymorphisms in methylenetetrahydrofolate reductase have been implicated in SOS in post-transplant patients.102 Recently, defibrotide has been used with success to resolve cases of SOS,103 although in some cases, transplantation can be required.104
Peliosis hepatis
Peliosis is characterised by blood-filled cavities without an endothelial lining in the hepatic parenchyma (fig 15). This phenomenon most commonly is associated with androgens105 or contraceptive steroids.106 Thiopurine-derived chemotherapeutic drugs also have been implicated.107 108 Peliosis also occurred with the intravenous contrast agent thorium dioxide (Thorotrast), which has been discontinued due to the high risk of angiosarcoma.109 110 Sinusoidal dilatation may accompany peliosis or may occur independently, particularly with androgenic or oestrogenic steroid use.111
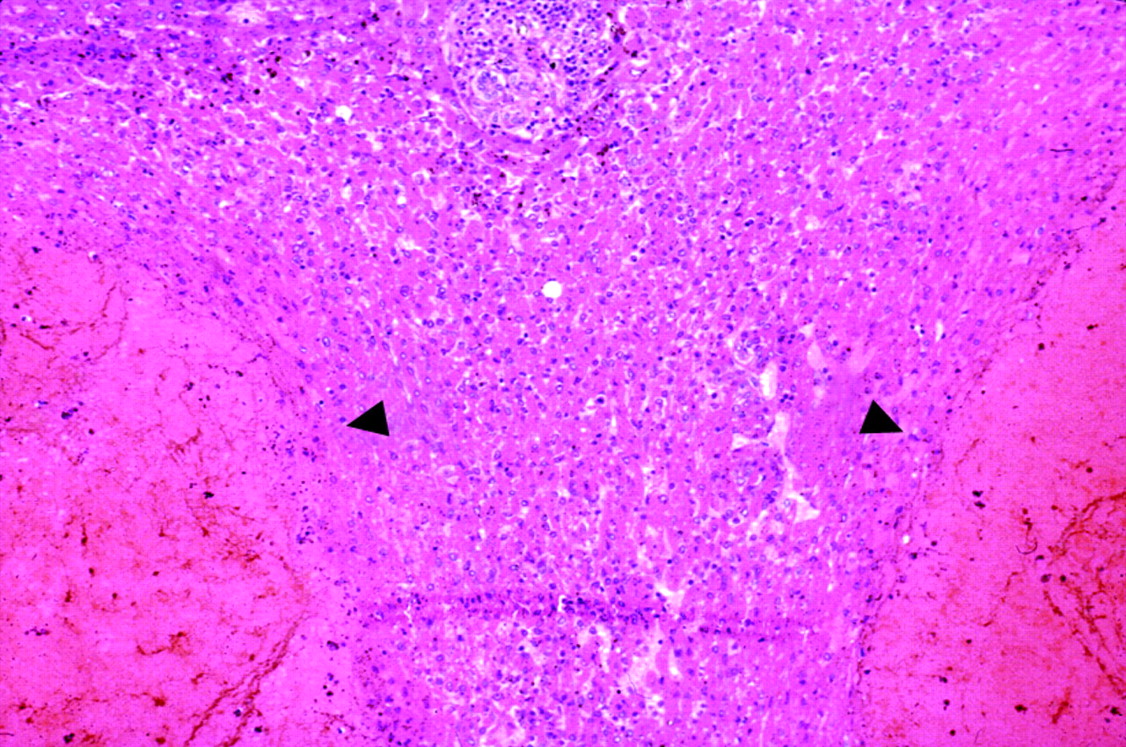
Peliosis. The hepatic parenchyma contains blood-filled cavities that lack an endothelial lining (arrows). H&E, ×66. (Image courtesy of Dr Linda Ferrell, University of California, San Francisco, California, USA.)
Hepatic vein thrombosis
Hepatic vein thrombosis is a rare complication of some drugs, including oral contraceptives112 113 and dacarbazine,114 and presents clinically as Budd-Chiari syndrome.
Other patterns
Stellate cell lipidosis
Hepatic stellate cells (Ito cells) are modified fibroblasts that store lipids and vitamin A in the normal liver. They are located in the space of Disse between the sinusoidal endothelium and the hepatocytes but generally are not easily visible.115 In certain conditions, especially hypervitaminosis A, excessive lipid gets stored in the stellate cells (stellate cell lipidosis, fig 16). The nuclei of stellate cells are crescent shaped, dark staining, and indented by the lipid droplets. Thin strands of cytoplasm separate the lipid droplets. These lipid-laden cells easily can be mistaken for hepatocytes with steatosis. Their characteristic morphology and location along the sinusoids between the hepatic plates distinguishes them from steatotic hepatocytes.116

Stellate cell (Ito cell) lipidosis. Fat-laden stellate cells showing multiple lipid vacuoles with indentation of the nucleus. Note the location of Ito cells along the sinusoids in the space of Disse. H&E, ×400.
Hypervitaminosis A results from excess dietary/supplementary vitamin A intake or use of oral/topical retinoids (such as etretinate for acne). Stellate cell lipidosis also has been reported with methotrexate, valproate and steroids, as well as in other clinical settings such as cholestasis, alcoholic liver disease and hepatitis C.
It is important to recognise this condition, as activation of stellate cells can lead to fibrosis, non-cirrhotic portal hypertension and, rarely, cirrhosis. One case of liver transplantation for subacute vitamin A toxicity has been reported.117 Early recognition can prompt reduced intake of vitamin A to avert progression and fibrosis. The contribution of stellate cell lipidosis to disease progression when present with other disease processes such as alcoholic liver disease and chronic hepatitis C is unknown.
Cytoplasmic inclusions
Ground glass change in the cytoplasm occurs in a minority of patients with hepatitis B and is characterised by pale eosinophilic cytoplasmic inclusions in hepatocytes. Similar changes (often termed “pseudo ground glass change”, fig 17) can be seen with drugs such as cyanamide, a drug used in alcohol treatment programs.118 119 This phenomenon has also been described with other drugs such as barbiturates and diazepam, diabetic patients on insulin, and transplant patients on multiple immunosuppressive drugs such as steroids, tacrolimus and mycophenolate mofetil.119 120 Similar to hepatitis B, this change reflects hypertrophy of smooth endoplasmic reticulum with use of drugs such as barbiturates, while most other drug-induced cases are due to accumulation of abnormal glycogen.118–120 Rare metabolic disorders such as type IV glycogenosis, hypofibrinogenaemia, and Lafora disease can lead to the same morphological findings.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ground-glass hepatocytes. This change can be seen with drugs such as cyanamide (used for treating alcohol abuse), diazepam and barbiturates, and in patients on insulin or intravenous glucose therapy. H&E, ×200.
Take-home messages
Drug-induced liver injury can mimic any pattern of primary liver disease. A thorough clinical history, including exposure to herbal, over-the-counter agents and toxins, along with a systematic literature search, is critical to establish the diagnosis.
Acute hepatitis, with or without cholestasis, is the most common histological pattern of drug-induced liver injury. Drugs such as acetaminophen are the most common cause of acute liver failure in the USA.
Drug-induced chronic hepatitis is rare, but fibrosis and cirrhosis can occur with drugs such as methotrexate, while autoimmune hepatitis-like disease can result with drugs such as minocycline.
In some instances, drug-related cholestatic injury can be prolonged and can lead to ductopenia.
Drug-induced steatohepatitis is a rare phenomenon, but is well known to occur with amiodarone and irinotecan. Many drugs, such as tamoxifen, oestrogenic drugs and nifedipine, can precipitate or exacerbate steatohepatitis in the presence of other risk factors.
Interactive multiple choice questions
This JCP best practice article has an accompanying set of multiple choice questions (MCQs).
To access the questions, click on BMJ Learning: take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://jcp.bmj.com/education Please note: the MCQs are hosted on BMJ Learning – the best available learning website for medical professionals from the BMJ Group.
If prompted, subscribers must sign into JCP with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Pigments
Some drugs/toxins such as gold, titanium and thorium dioxide (Thorotrast) can be deposited as pigments in the liver. Drugs that cause prolonged cholestasis can lead to copper accumulation in periportal hepatocytes. Lipofuscin, a lysosomal pigment often seen in centrizonal hepatocytes, can be increased with exposure to anticonvulsant drugs such as phenothiazine and phenacetin.
Hepar lobatum
This term generally refers to liver abnormalities in tertiary syphilis. In some instances, chemotherapy for metastatic liver cancer (especially from the breast) can lead to similar changes. The liver shows a lobulated contour with capsular indentations from which fibrous septa extend deep into the parenchyma.121 The fibrous septa can surround the degenerated centre of tumour nodules and may contain macrophages and residual tumour. Typical features of cirrhosis such as regenerative nodules are not observed. These features probably result from tissue collapse due to chemotherapy-related tumour regression that is followed by an organising phase of healing and scar contraction.121
Drug-related neoplasms
The association of oral contraceptives and hepatic adenomas is well recognised.122 Association with focal nodular hyperplasia and hepatocellular carcinoma also has been reported,123 124 but the link is less convincing. Other agents such as anabolic steroids used by sportsmen, clomiphene, danazol and carbamazepine have also been associated with hepatic adenoma.125 126
Exposure to vinyl chloride (an industrial chemical) and thorium dioxide (a discontinued radiographic contrast agent) can lead to angiosarcoma, sometimes after long latent periods exceeding 20 years.127 Hepatocellular carcinoma and cholangiocarcinoma also have been reported with thorium dioxide.128
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- PostScript