Article Text

Statistics from Altmetric.com
Keratocystoma of the parotid gland was first defined and reported as an unusual pathological entity in 2002.1 It was not listed as an independent pathological entity in the revised World Health Organization (WHO) classification of salivary gland tumours published in 2005.2 Recently, the designation of keratocystoma of the parotid gland was introduced as a newly recognised diagnosis.3 Here, we present a case of a benign tumour of the parotid gland diagnosed as a keratocystoma.
Case report
A 37-year-old man presented with a painless circumscribed nodule that had been gradually enlarging in the left parotid gland area for six years. No cervical lymphadenopathy was detected. A subtotal parotidectomy was performed and a tumour was excised. No tumour recurrence was observed 18 months after the surgery.
Grossly, the tumour was completely circumscribed within the parotid gland, measuring 20×18×15 mm in size. The cut surface revealed multilocular cystic spaces. No bleeding or necrosis was detected in the tumour.
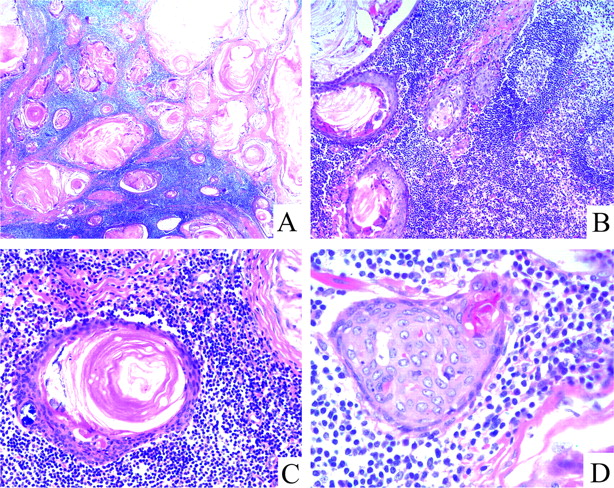
Histologically, the tumour consisted mainly of multiple cystic formations lined with stratified squamous epithelium lacking a granular layer, but containing keratin material and calcification (figure 1). There was no evidence of cytological atypia or abnormal mitotic activity in the epithelium. No tubules, duct-like glandular structures, or sebaceous differentiation were observed. No evidence of skin appendages was found beneath the epithelium. The stroma of the tumour was predominantly a dense lymphoid element. The tumour cells stained negatively with periodic acid-Schiff (PAS) and Alcian blue.
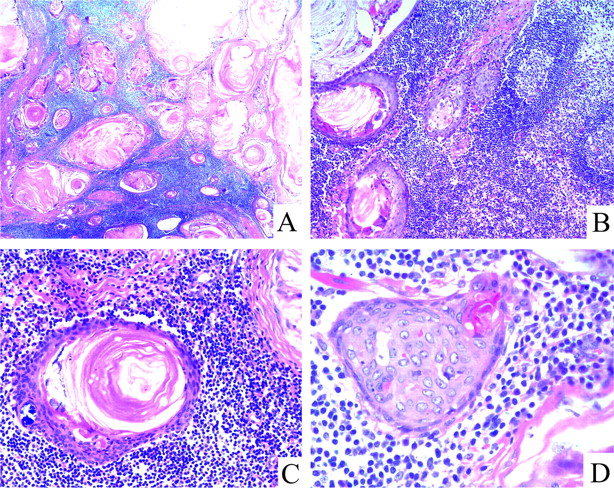
H&E stained sections showing the keratocystoma morphology. (A) Characteristic tumour view consisting of variably sized and shaped cystic lesions filled with lamellar keratin material and calcification (×20). (B) The stroma of the tumour showing predominantly a dense lymphoid element (×100). (C) The stratified squamous epithelium lacking a granular layer filled with lamellar keratin material (×200). (D) Solid squamous cell islands exhibiting uniform, bland nuclei and abundant eosinophilic cytoplasm (×400).
By immunohistochemistry, the tumour cells were diffusely positive for cytokeratins AE1/AE3 and 5/6, focally positive for cytokeratin 7, and stained strongly for p63, but weakly for p53 (figure 2). The basal cells of the stratified epithelium were partially positive for cytokeratin 19. The tumour cells were completely negative for cytokeratins 8/18 and 20. Less than 1% of all tumour cells were Ki-67 positive.

{kind=link}
{kind=link}
Immunohistochemical findings in the keratocystoma specimen. The tumour cells strongly stained for AE1/AE3 (A), CK5/6 (B), and p63 (C), or weakly stained for p53 (D) in the keratocystoma case. Inset images show positive cells in the region. All sections are counterstained with haematoxylin (×200).
Discussion
Keratocystoma is a rare benign tumour of salivary gland origin whose nomenclature remains to be confirmed. To the best of our knowledge, only four cases, including the present case, have been reported in the English literature.1–4
This type of tumour needs to be differentially diagnosed with several tumours of the parotid gland containing squamous cells, including primary and metastatic squamous cell carcinomas, mucoepidermoid carcinoma, squamous metaplasia in certain benign neoplasias and conditions, and cysts.1 In this case there is no evidence of cytological atypia or abnormal mitotic activity in the squamous cell, which is different from squamous cell carcinoma. The absence of incorporated mucous cells by the mucicarmine stain (Alcian blue) and the presence of marked keratinisation are important for separating this tumour from mucoepidermoid carcinoma. The histology of the tumour is different from Warthin's tumour, which presents with cystic spaces surrounded by two uniform rows of cells with centrally placed pyknotic nuclei. The first banchial cleft cyst can involve the parotid gland. The cystic spaces are usually lined with squamous epithelium with keratin material filling the lumen, but pseudo-stratified columnar epithelium can also be seen. Sebaceous lymphadenoma and non-sebaceous lymphadenoma of the parotid gland need to be excluded. Overexpression of p63 and p53 in the tumour support neoplastic proliferation. We believe that this type of tumour is a true benign cystic neoplasm, not a christoma or trichoadenoma, based on its morphological and immunohistochemical findings.
Take-home messages
A rare case of a benign tumour of the parotid gland, presenting as a keratocystoma, is described.
It is believed that only four cases, including the present case, have been reported in the English literature.
Histologically, the tumour consisted mainly of variably sized and shaped cystic lesions filled with lamellar keratin material and calcification.
By immunohistochemistry, the tumour cells were positive for cytokeratins, p63 and p53.
Acknowledgments
We thank J K C Chan (Department of Pathology, Queen Elizabeth Hospital, Hong Kong) for consultation about the present case.
Footnotes
Funding The National Natural Science Foundation of China (No. 30471960 and No. 30973506).
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Independent Ethics Committee of the Cancer Center of Sun Yat-Sen University.
Provenance and peer review Not commissioned; externally peer reviewed.