Article Text

Abstract
With an increasingly ageing population, osteoporosis and osteoporosis-related fractures is fast becoming an important public health problem placing a considerable economic burden on health service resources. This does not account for the substantial pain, disability and indeed mortality incurred after a fracture, particularly a hip fracture. Osteoporosis is a systemic skeletal disorder which results from an imbalance in bone remodeling. This leads to a reduction in bone strength and increased susceptibility to fracture. It affects up to 1 in 2 women and 1 in 5 men. In the past 2 decades, there have been significant advances in bone biology which have helped in the understanding of the pathogenesis of osteoporosis and have led to improved therapies. In developing strategies for fracture prevention, it is important to identify those individuals with the highest fracture risk who will require pharmacological intervention. Treatment is aimed at fracture prevention and includes modification of general lifestyle factors which have been linked to fractures in epidemiological studies and ensuring optimum calcium and vitamin D intake as adjunct to active anti-fracture therapy. A number of drugs are now approved for the treatment of osteoporosis. This review article will describe the pathogenesis of osteoporosis and focus on the methods currently in use for the identification of patients at high fracture risk and will highlight their usefulness and limitations. The existing anti-fracture pharmacotherapies and those in development will be reviewed. Assessment of their effectiveness including the use of biochemical markers of bone turnover in this clinical context will be reviewed.
- Bone
- chemical pathology
Statistics from Altmetric.com
Introduction
Osteoporosis is a systemic skeletal disorder which results from an imbalance in bone remodelling, leading to a reduction in bone strength, with microarchitectural disruption and skeletal fragility, increasing fracture susceptibility.1 ,2 Bone strength is a function of both bone density and quality. Bone quality refers to a composite of factors that determine bone resistance to fracture such as its microarchitecture.1 ,3 Osteoporosis is a major public health and financial problem. In the UK, one in two women and one in five men will suffer a fracture after the age of 50, with an annual cost to the health services of around £2 billion.4–7 Hip fracture is the most serious consequence of osteoporosis and, like other osteoporotic fractures, is associated with increased mortality risk and reduced quality of life, with up to 50% of patients left with a permanent impaired mobility.8–11 A recent meta-analysis showed that among older men and women, the rate of death from any cause is increased by a factor of 5 to 8 during the first 3 months after a hip fracture.12 Increased mortality risk persisted for 5 to 10 years following all low trauma fractures in a prospective cohort study of men and women aged >60 years.13 Therefore, prevention of fractures is the primary goal of intervention.
Pathogenesis
Osteoporosis can occur because of (1) failure to achieve peak bone mass and (2) excessive bone resorption and/or decreased bone formation during remodelling. All these processes are likely to contribute, in varying degrees, to osteoporosis.
Achievement of peak bone mass
Attainment of peak bone mass is of prime importance in preventing osteoporosis and subsequent fractures in adulthood. Hip fracture can be reduced by 30% with an increase in peak bone mass of 10%. Genetic factors are major determinants of peak bone mass and bone loss, contributing as much as 80% to peak bone mass variability based upon twin studies. Genome-wide association studies have identified several genetic variants that regulate bone mass, including low-density lipoprotein receptor-related protein 5 (LRP5), sclerostin (SOST), osteoprotegerin (OPG), oestrogen receptor 1 and receptor activator of NF-κβ (RANK) pathway genes.14 So far, 20 genes have been identified that predispose to osteoporosis, but they each contribute to only a small amount of the genetic variance in susceptibility to the disease.15 This could be because genome-wide association studies are geared towards identification of common variants of small effects rather than rare variants of large effects. Further work is in progress to determine rare polymorphisms in other candidate genes which could have larger effects.16 However, at present, not enough is known about the genetics of osteoporosis to influence clinical decision making. Bone mass accretion in childhood and early adulthood is also influenced by hormonal status, particularly oestrogen. Environmental factors such as nutrition, exercise and smoking play important roles in achievement of peak bone mass.17 ,18 It is now known that modulation of peak bone mass can occur during intrauterine life and is affected by maternal nutrition, smoking and level of exercise.19
Imbalance of bone resorption and bone formation
In adulthood, the bone remodelling process is pivotal for bone health maintenance as it repairs areas of microdamage. This is a cellular process involving coordinated actions of osteoclasts (bone resorbing cells) and osteoblasts (bone forming cells), which form the bone multicellular unit. The OPG/RANK and its ligand (RANKL) are the most important mediators of osteoclast activity, whereas LRP5 is one of the most important mediators of osteoblast activity.20 ,21 Other cells contribute to the bone remodelling process and include the terminally differentiated osteoblasts, osteocytes and vascular elements forming the bone remodelling compartment. Bone resorption is stimulated through production of RANKL by cells of the osteoblastic lineage. Binding of RANKL to its cognate receptor RANK results in activation of complex intracellular pathways including NF-κβ, which results in induction of osteoclastogenic genes. OPG acts as a decoy receptor, preventing RANKL binding to RANK. Proteins called Wnt's activate the LRP5 pathway, which stimulates bone formation and inhibits bone resorption. A variety of inhibitors of LRP5 signalling have been identified including SOST, which is produced by osteocytes and likely acts as a mediator of the effects of mechanical loading on the skeleton.22
The OPG/RANKL ratio is a key factor in maintenance of normal bone turnover and bone mass/strength. Numerous hormones, growth factors (TGF-β, IGF-1, BMP2), cytokines (IL-1, IL-6, TNF-α, prostaglandins E2) and drugs influence the expression of OPG/RANKL and therefore bone turnover23–26 (table 1). It is well established that imbalance in bone remodelling at the menopause is due to oestrogen deficiency.27 In men, although there is a slower reduction in serum testosterone with advancing age, bioavailability diminishes progressively, particularly after age 80, resulting in bone loss, though much of the effect of testosterone is mediated by aromatisation to oestradiol.28
Effect of several hormones on OPG/RANKL ratio
Although it seems likely that increased bone resorption has the greatest impact on bone loss and fracture risk,29 ,30 impaired bone formation in response to increased bone resorption rate is an important component of the pathogenesis of osteoporosis. This is thought to be due to a reduction in the number of osteoprogenitor/pre-osteoblastic cells and/or an age-related defect in their proliferative and differentiation abilities. With increasing age, bone formation falls more than bone resorption, presumably due to a preferential differentiation of bone marrow stromal cells into adipocytes rather than osteoblasts.
Age and menopause-related bone losses are clearly important factors for osteoporosis, with genetic factors likely explaining the wide variations in skeletal integrity in older persons of the same age.31 In addition, age-related factors such as visual acuity, muscle strength, poor balance and drugs that affect balance will interact with bone density in an important way to determine fracture risk.
Diagnosis and investigation
A major problem of osteoporosis management is that majority of those at high fracture risk are not diagnosed or treated, despite availability of safe and effective diagnostic tools and therapies.32 ,33 This paucity of care applies to both women and men, although more evident in men.
Measurement of BMD
Diagnosis of osteoporosis is based on measurement of bone mineral density (BMD), using dual X-ray absorptiometry (DXA), which is considered the gold standard. However, a personal history of fragility fracture is consistent with a clinical diagnosis of osteoporosis, regardless of BMD, in the absence of other causes of skeletal fragility. BMD results are reported as a comparison to a sex-matched young healthy adult (T-score) or a sex-matched and age-matched healthy population (Z-score) and is expressed in standard deviations. The WHO has defined osteoporosis as a T-score of less or equal to −2.5 and osteopenia as a T-score between −1.0 and −2.5.34 The T-score criteria are used for postmenopausal women and men aged 50 years or older. Outside this demographic group, the T-score is less accurate as a predictive tool for fracture risk. The International Society for Clinical Densitometry recommend using the Z-score instead of BMD to be measured in premenopausal women and men younger than 50 years of age, with a score less than or equal to −2.0 indicative of a bone density that is below the expected range for age.35 BMD is measured at both the spine and hip. The forearm (33% radius) is recommended if the hip and/or spine cannot be measured or interpreted, in hyperparathyroidism and in obese patients who are over the weight limit for DXA table. BMD is a specific predictor of fracture risk as demonstrated in several studies in men and women. Individuals with T-scores below −2.5 have progressively higher fracture risk. However, patients with T-scores above −2.5 may still be at high risk of fracture. It has been estimated that over 50% of patients with hip fractures and 35% with vertebral fractures have a T-score above −2.5.36–38 Hence, a combination of BMD and clinical risk factors for fracture predicts fracture risk better than BMD alone.
Assessment of clinical risk factors and fracture risk
Fracture is the outcome of multiple risk factors, and this multiplicity should be taken into account in assessment of fracture risk for an individual. Several important clinical risk factors have been identified through epidemiological studies, including age, falls and history of fragility fractures (box 1).39–41 In addition, several disorders and drugs can lead to increased bone loss and are important secondary causes of osteoporosis. Differential diagnosis includes a thorough medical history, physical examination and a range of investigative tests which may be case-dependent (box 2).
Clinical risk factors for osteoporosis and fractures
-
Age*
-
Sex*
-
Ethnicity
-
Femoral neck bone mineral density*
-
Body weight*
-
History of prior fractures*
-
Height*
-
Parental history of hip fracture*
-
Current smoking*
-
Glucocorticoid therapy* †
-
Alcohol consumption (3 or more units per day)*
-
Rheumatoid arthritis*
-
History of falls
-
Secondary osteoporosis (eg, hyperthyroidism, hypogonadism or premature menopause, malabsorption, chronic liver disease, inflammatory bowel disease)*
-
Medications (eg, immunosuppressants, antiseizure medications, heparin, chemotherapy)
*Clinical risk factors included in the FRAX algorithm
†Past or present exposure to prednisone equivalent dose of 5 mg or more for more than 3 months.
Laboratory evaluation for secondary causes of osteoporosis
Initial laboratory tests
-
Renal profile (Urea, Creatinine)
-
Calcium, phosphorus, magnesium
-
Liver function tests
-
Full blood count
-
25 Hydroxyvitamin D
-
Thyroid stimulating hormone
-
Parathyroid hormone
Additional laboratory tests if indicated
-
Sex hormones (Testosterone, Oestradiol, LH, FSH)
-
Coeliac serology
-
Serum/Urine protein electrophoresis
-
Erythrocyte sedimentation rate
-
24-h Urine calcium/Creatinine
-
Bone turnover markers
-
24-h Urine free cortisol
-
Prolactin
-
Iron studies
-
Serum tryptase and histamine levels
-
Homocysteine
-
Rheumatoid factor
-
Skin biopsy for connective tissue disorders
LH, luteinising hormone; FSH, follicular stimulating hormone.
In order to assist clinicians in their clinical management process, the WHO task force has developed and introduced a country-specific Fracture Risk Assessment Tool (FRAX), based upon data collected from large international cohorts in which clinical risk factors, BMD and fractures were evaluated. The tool combines BMD measurement and clinical risk factors to derive a 10-year probability of hip fracture or major osteoporotic fracture (combined hip, spine, humerus or wrist), thus allowing identification of individuals at high fracture risk.42 Those with probabilities above the intervention threshold will require pharmacological intervention (National Osteoporosis Guideline Group). Absolute risk assessment is now recognised as a preferred approach to guide treatment decision as opposed to RR, which is a comparison between different risk levels and not a reflection of the individual's actual risk. The FRAX tool is particularly useful in identification of patients with osteopenia who are at higher risk of fracture. Though the FRAX algorithm is useful in assessing an individual's absolute fracture risk and hence individualising treatment, it has some limitations which prevent it from being the gold standard. First, it has been designed for postmenopausal women and men older than 40 years of age who have not previously been on bone protective treatment. Second, it does not take into account dose–responses for several risk factors including glucocorticoid use. Third, falls or increased propensity to falls is not included in the algorithm. Fourth, femoral neck BMD only is used to compute fracture risk; therefore, absolute fracture risk may not be accurate in those patients who have lowest BMD at the spine. In addition, it is country-specific and has to be used cautiously in countries where there is no representation.
Clinical management/therapeutic interventions
Treatment is aimed at reducing future fracture risk and should be tailored to the individual patient. The emphasis should be on early recognition and effective management of patients at high fracture risk.
Non-pharmacological intervention
This includes modification of general lifestyle factors, such as a balanced diet containing calcium and vitamin D, smoking cessation and avoidance of heavy alcohol use. A regular exercise routine should be encouraged, including weight-bearing and muscle-strengthening exercises.43 ,44 In a Cochrane analysis of 18 randomised-controlled trials examining the effectiveness of exercise therapy in preventing bone loss in postmenopausal women, aerobics, weight bearing and resistance exercises were all effective on the BMD of the spine.45 Walking was effective on both BMD of the spine and the hip and should be recommended as it is the easiest and simplest program to implement. Long-term studies to determine fracture data are required. Falls prevention is integral in fracture prevention. Interventions suitable for falls reduction has been summarised in a Cochrane review and include an exercise program incorporating balance, gait and strength training.46 There is also evidence to support correcting of vision impairment as part of a multifactorial approach.47
The role of calcium and vitamin D supplementation in reducing falls and fractures is not clear. A reduction in either calcium intake or absorption and/or vitamin D deficiency/insufficiency leads to secondary hyperparathyroidism, which contributes to accelerated bone loss in the elderly.48 A meta-analysis concluded supplementation for people aged 50 years or more conferred a reduced risk of any fracture of 12% (RR=0.88, 95% CI 0.83 to 0.95), the greatest effect being with a daily dose of 1200 mg calcium and 800 IU vitamin D.49 The antifracture effect of vitamin D is more pronounced in the vitamin-D-deficient institutionalised elderly and involves, in part, its effect on muscle strength and therefore in falls prevention.50 ,51 Vitamin D deficiency impairs neuromuscular function, increasing falls risk (figure 1). As calcium was given along with vitamin D in many of the positive trials, it has become routine clinical practice to replete both calcium and vitamin D. Indeed, all trials of antifracture therapies have been carried out in subjects given both calcium and vitamin D as adjunct. It can be concluded therefore that the antifracture abilities of these drugs apply to calcium-replete and vitamin-D-replete individuals.52

Consequences of vitamin D deficiency/insufficiency. The reduction in intestinal calcium absorption associated with vitamin D inadequacy triggers the release of parathyroid hormone, which mediates the mobilisation of calcium from bone, resulting in a reduction in bone mineral density. This homoeostatic response to vitamin D inadequacy may increase the risk of fractures. Another important consequence of vitamin D inadequacy is a decrease in neuromuscular function.
What constitutes optimum vitamin D status is still a subject of debate and is defined in some studies as a serum 25-hydroxyvitamin D (25OHD) concentration of >50 or 75 nmol/l.53 ,54 Several criteria have been used to define ‘sufficient’ 25OHD level, including the level associated with optimal suppression of parathyroid hormone (PTH), greatest calcium absorption, highest BMD, lowest rates of bone loss, lowest rates of falling and lowest fracture rates. Defining optimal 25OHD concentration is further complicated by differences in assay methodologies and standardisation which needs addressing to assist design of population supplementation strategies. Based on available evidence, it has been suggested that although estimates of serum 25OHD level needed for optimal suppression of PTH varied widely, optimal vitamin D status clusters in the 75 to 80 nmol/l range with a lower risk of fracture at serum levels >75 nmol/l.55 ,56 Calcium absorption is considered to be impaired under conditions of vitamin D deficiency, though it is uncertain at what vitamin D status, calcium absorption is fully normalised. In an analysis of two randomised cross-over studies, mean calcium absorption was 65% higher at serum 25OHD levels averaging 86.5 nmol/l than at levels averaging 50 nmol/l.57 A recent histomorphometry study of 675 German adults showed a surprisingly high incidence of osteomalacia but no evidence of osteomalacia with 25OHD concentrations >75 nmol/l, suggesting this may be an appropriate cut-off for optimal bone health.58 Serum 25OHD below these concentrations are highly prevalent in the UK, particularly in the elderly where a significant proportion have serum 25OHD concentrations <25 nmol/l which constitutes vitamin D deficiency. Though there is a consensus to maintain 25OHD levels >25 nmol/l in the UK, there is uncertainty regarding the strength of evidence for aiming for substantially higher 25OHD concentrations.59
Supplementation with calcium in osteoporosis prevention is currently in question following a recent meta-analysis which showed calcium supplements to be associated with about a 30% increased risk of myocardial infarction.60 In contrast, there appears to be an association between a low 25OHD status and increased CVD risk.61 A meta-analysis showed decreased total mortality rates with vitamin D supplementation, with no change in RR with the addition of calcium supplements.62 The main concern with excessive vitamin D is hypercalciuria and hypercalcaemia. However, there is a relatively large therapeutic window for vitamin D, with hypercalcemia not reported with blood 25OHD levels <220 nmol/l and generally not reported until blood levels reach 500 nmol/l.63
We would recommend aiming for a serum 25OHD of 75 nmol/l in high-risk population, such as the housebound and institutionalised elderly; however, this may be difficult to achieve with the current recommended vitamin D intake of 800–1000 IU, which is more a maintenance dose. On average, 25OHD rises by approximately 0.7 nmol/l for each microgram (40 IU)/day of supplemental vitamin D3 to reach a plateau at about 8 weeks.64 With regard to calcium, we would recommend a daily intake of 1000–1200 mg daily, with supplements suggested only if dietary intake is inadequate. Compliance is an issue; hence, side effects of supplements need to be taken into account. With calcium supplements, side effects such as constipation may reduce overall compliance with all medications and hence limit treatment effectiveness.
Pharmacological intervention
Significant advances in bone biology in the past two decades have helped in understanding the pathogenesis of osteoporosis, leading to better therapies. A number of drugs are now approved for treatment of osteoporosis (table 2), but there is a lack of high-quality head-to-head drug comparison trials to determine the relative efficacy of individual drugs. A systematic review of 76 randomised trials and 24 meta-analyses confirmed efficacy of multiple agents compared with placebo in fracture prevention.65 The bisphosphonates (alendronate, risedronate, zoledronate) and oestrogen reduced risk of vertebral, non-vertebral and hip fractures. However, the Women's Health Initiative, concluded the benefits of hormone replacement therapy (HRT) such as fracture prevention and colon cancer, were outweighed by the risks of breast cancer, coronary heart disease, stroke and thromboembolism,66 thus greatly diminishing use of oestrogen in prevention and treatment of osteoporosis. There is, however, a more favourable risk/benefit ratio of HRT in postmenopausal women <60 years of age and in women with early menopause. In this group, HRT is recommended by the National Osteoporosis Society (UK) particularly if menopausal symptoms are present, provided there are no risk factors for breast cancer, stroke, heart disease or venous thromboembolism.
Therapeutic agents available for osteoporosis, mode of action and fracture efficacy
Bisphosphonates are synthetic analogues of pyrophosphate which have a high affinity for bone mineral and reduce osteoclastic activity. All bisphosphonates are approved for treatment in postmenopausal osteoporosis with alendronate, risedronate and zoledronate approved for men and glucocorticoid-induced osteoporosis. In the absence of randomised trial data that ibandronate reduces hip fracture risk, alendronate or risedronate are the initial choices for oral bisphosphonates,67 ,68 with alendronate recommended as first choice based on the National Institute of Clinical Excellence (NICE) guidelines, as there are generic versions available making it cost effective. Intravenous zoledronate is used for individuals with gastrointestinal intolerance to or those who have failed treatment with oral bisphosphonates as is ibandronate. There has been a decrease in mortality by about 28% demonstrated with zoledronate following hip fractures.69 ,70
The association between bisphosphonate use and the rare complication of osteonecrosis of the jaw has been described recently, mainly in patients receiving high-dose bisphosphonates for metastatic cancer and undergoing invasive dental procedures.71 ,72 The risk is low in patients treated for osteoporosis, in the range of 1 in 10 000 to 10 000 patient years. Nevertheless, patients receiving oral bisphosphonates should have good oral hygiene and see their dentists regularly. In addition, there have been case reports of association of bisphosphonate use with atypical femoral fractures.73 In some of these cases, bone biopsies were done and showed severely suppressed bone turnover and delayed healing.74 However, there is no definitive evidence with recent reports suggesting no relationship between bisphosphonate and fractures, warranting ongoing investigation.75 ,76 More recent studies have shown a possible association between oral bisphosphonates and increased risk of oesophageal cancer, mainly in patients who have been on bisphosphonates for more than 5 years, though this remains unproven.77 ,78
Optimal duration of bisphosphonate therapy remains uncertain. There is evidence of ongoing fracture risk reduction if treatment is continued at least for 10 years in patients on alendronate 67 ,79 and 7 years in patients on risedronate,68 with no new safety concerns. However, it is becoming routine clinical practice to recommend a ‘drug holiday’ (time off bisphosphonate) in patients on long-term bisphosphonate due to potential concerns that long-term suppression of bone turnover may eventually lead to adverse events. The duration of therapy and length of holiday should be individualised, taking into account fracture risk and binding affinity for the bisphosphonate used, with lower affinity agents having a shorter residence time in bone if treatment is stopped. Rank order for binding affinity is zoledronate > alendronate > ibandronate > risedronate.80 Based on available evidence, discontinuing therapy after 5 years appears not to be harmful.79 ,81 Because of the long skeletal retention time of bisphosphonates, antifracture benefits still persist despite discontinuation for 12–18 months. However, in patients with a high risk of fracture, it is recommended that a non-bisphosphonate treatment be commenced, such as raloxifene or teriparatide during the holiday from the bisphosphonate.82
Other available antiresorptives include the selective oestrogen receptor modulators such as raloxifene, which is somewhat less effective than bisphosphonates, though direct comparison trials are lacking.83 Raloxifene is associated with an increased risk of venous thromboembolic events, particularly during the first 4 months of treatment, and it can cause or exacerbate vasomotor symptoms associated with menopause. While there are data to suggest raloxifene may be effective in men, it is not currently recommended for use in men.84 In the UK, raloxifene is not recommended for primary prevention of postmenopausal osteoporosis but can be used in secondary prevention as alternative treatment to patients intolerant to or who have contraindications to bisphosphonate.
Strontium ranelate has weak effects on bone resorption and bone formation. However, its mechanism of action is not fully understood, and it is likely that its antifracture efficacy is mediated by its effects on bone material properties rather than its rather weak effect on skeletal remodelling.85 A meta-analysis of four trials concluded that there is reasonable evidence strontium ranelate is effective for reducing the risk of vertebral fractures and, to a lesser extent, non-vertebral fractures in women.86 A small increase in the risk of venous thromboembolism was seen in clinical trials. Strontium has not been studied in men. In the UK, strontium is recommended as an alternative to bisphosphonates in the prevention/treatment of osteoporosis if patients are unable to comply with administration of are intolerant or have a contraindication to the bisphosphonates.
Intermittent administration of the bone anabolic agent, recombinant human parathyroid hormone (PTH: full length 1–84 or fragment 1–34) stimulates bone formation, which results in improvement in trabecular numbers and connectivity and increased cortical thickness and bone strength.87 Larger increases in bone mass, particularly at the lumbar spine, are seen with intermittent PTH than with antiresorptives.88 ,89 Duration of treatment is limited to 24 months. Candidates for treatment are those with very low BMD, at very high risk of fracture and who have failed previous therapy with antiresorptives. Recombinant PTH is also approved for men and postmenopausal women receiving glucocorticoids who are at increased risk of fracture. Sequential therapy with bisphosphonate is required following cessation of PTH.
For women, treatment agents include tibolone, a synthetic steroid used for osteoporosis management in postmenopausal women in some countries.90 ,91 For men with osteoporosis and hypogonadism who do not have any contraindications to testosterone therapy, testosterone replacement therapy is beneficial.92–94
Newer therapies available include the humanised monoclonal antibody, denosumab. This binds RANKL, thus reducing osteoclastogenesis. Data from the multicenter FREEDOM trial show that treatment with denosumab in 60- to 90-year-old women over 3 years led to statistically significant increases in BMD and reductions in bone resorption.95 It has been shown to reduce the incidence of new vertebral, hip and non-vertebral fractures in postmenopausal women. In the UK, it is approved for both primary and secondary prevention of postmenopausal osteoporosis.96
Emerging therapies under investigation for the treatment of osteoporosis include: oral calcium sensing receptor antagonists which leads to a transient rise in endogenous PTH; SOST inhibitors (SOST is produced by osteocytes and inhibits bone formation), which increases bone mass in animal studies97; integrin antagonists (integrins mediate the adhesion of osteoclasts to the bone surface, an important initial step for bone resorption)98; cathepsin-K inhibitors (cathepsin K is a protease that may play a role in osteoclast-mediated bone resorption).99
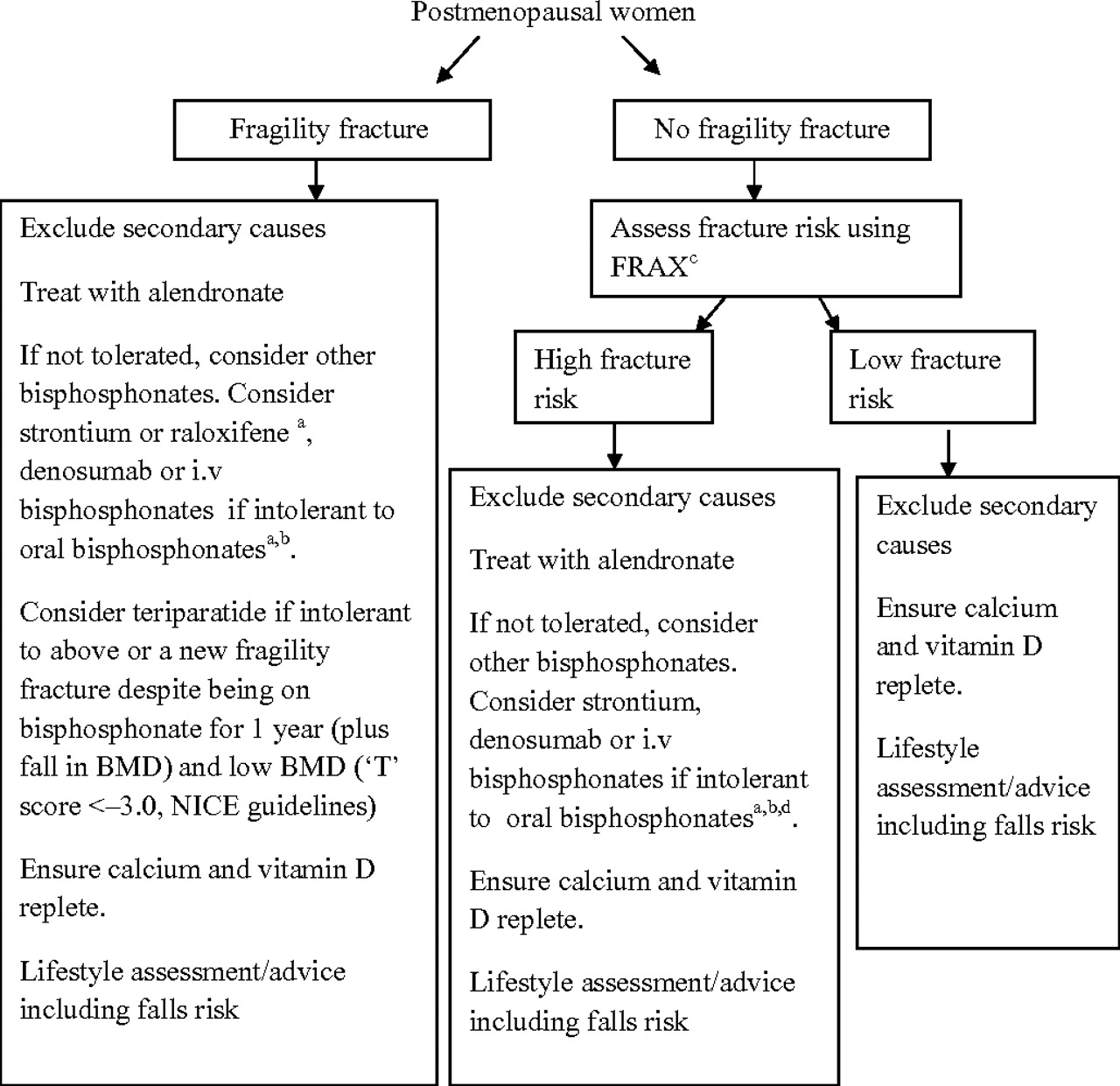
Our recommendation for a management approach when treating osteoporosis in postmenopausal women is shown in figure 2. This takes into account the NICE guidelines.
{kind=link}
{kind=link}
Proposed algorithm for management of osteoporosis in postmenopausal women. (A) Owing to lack of evidence of efficacy in non-vertebral fractures, including hip fractures, we would recommend avoiding ibandronate or raloxifene in patients with non-vertebral fractures or low BMD in non-vertebral sites (not in the NICE guidelines). (B) Consider intravenous bisphosphonates if intolerant to oral bisphosphonates or if treatment failure (not in the NICE guidelines). (C) FRAX not included in the NICE guidelines. (D) Raloxifene is not recommended as a treatment option for primary prevention of osteoporotic fragility fractures in postmenopausal women according the NICE guidelines.
Treatment follow-up and monitoring
Monitoring response to therapy is important for identifying patients who may require a change in therapy; however, there is no consensus on the optimal strategy for this.
Assessment of changes in BMD
Some studies suggest that BMD increase during therapy correlate with reduction in fracture risk.100–102 A meta-analysis of 12 clinical trials concluded that improvement in spine BMD with therapy accounts for a predictable but relatively small part of reduction in fracture risk, explaining only 16% of fracture risk reduction, suggesting contribution of other non-BMD effects of therapy.103 In order for a change in BMD to be considered significant, it should be greater than the ‘least significant change’ (LSC) for the densitometer in question. Precision error of the DXA scan should be determined and the LSC calculated so as to determine whether an apparent change in BMD represents a likely biological change or is simply within the range of measurement error. The short-term precision error expressed as coefficient of variation (CV) ranges from 1.9% to 2.5% in elderly women at the lumbar spine and hip, respectively. Follow-up BMD measurements play a role in clinical management. BMD that is stable or improving is evidence for treatment response. Finding of a clinically significant decrease in BMD in a treated patient should trigger additional evaluation for contributing factors, which may include poor adherence to therapy. The International Society for Clinical Densitometry recommends follow-up BMD testing (DXA spine and hip) when the expected change in BMD is likely to equal or exceed the LSC, typically 1–2 years after initiation or change of therapy, with longer intervals once therapeutic effect is established. In conditions associated with rapid bone loss, such as glucocorticoid therapy, testing more frequently is appropriate.104
Use of BTMs
Use of biochemical bone turnover markers (BTMs) in clinical trials has been helpful in understanding mechanism of action of therapeutic agents. A list of commonly used BTMs is shown in table 3. Their routine use, however, remains a challenge on account of their wide biological and analytical variability, which may be as much as a 7.3-fold difference.105 Discordant results are sometimes obtained because of differences in assay techniques, inappropriate collection and timing of sample. The analytical variability can be reduced with automation and improved standardisation between assays and standardisation of sample collection.106 ,107 In general, intraindividual variability is lower for serum or plasma than urine markers. Circulating C-terminal cross-linked telopeptide (CTX) can be measured in either plasma or serum and is dependent on the assay used. It is preferable to use plasma when the Roche automated (β-crosslaps) assay is used. The CV for plasma CTX and N-terminal cross-linked telopeptide (NTX) is reportedly half that for urine CTX or NTX with CV of 10% for plasma markers and between 15% and 25% for urine markers. The use of well-defined reference ranges can minimise the variability associated with several uncontrollable factors—for example, age, gender, pregnancy, lactation, fracture status and other diseases. Recommendations for establishing reference ranges should be defined and standardised with emphasis on sample size and age range of the population.108
List of biochemical markers of bone turnover commonly used in clinical practice
The best established clinical use for BTMs is in monitoring treatment efficacy and compliance. Antiresorptive agents such as bisphosphonates, oestrogens, selective oestrogen receptor modulators and denusomab rapidly decrease BTMs.70 ,109–113 Significant reductions in bone resorption markers, particularly urine NTX or plasma/serum CTX, are seen after 1 month of treatment and reach a plateau from 3 months onwards. Relative plasma or serum CTX reductions of 50–70% after 3 months of treatment have been reported for several bisphosphonates.111 The decrease in bone formation markers is delayed compared to bone resorption markers, reaching a plateau after 6–12 months of treatment. Anabolic agents such as Teriparatide (PTH analogue) stimulates bone turnover. Procollagen type 1 N-terminal propeptide starts to increase as early as 1 month with a peak at 6 months. Increases of >200% have been documented.114–116
The LSC for each marker should be derived in order to determine whether changes in BTMs are of clinical significance in an individual patient.117 Changes of >30% for plasma or serum-based markers should be of clinical significance as these changes exceeds the LSC which is between 25% and 30% for these markers. On average, BTMs change by 50% following antifracture treatment, making it easier to use in monitoring treatment efficacy at earlier time points than BMD changes. Insufficient BTMs reduction after a period of antiresorptive therapy with oral bisphosphonates may indicate lack of drug absorption or issues surrounding patient adherence. In the individual patient, where the change in BTMs is equivocal, another measurement is recommended 3 months later as caution should be exercised before changing treatment on the basis of an insufficient BTM response. Sequential BTMs measurements should be obtained on more than two separate occasions before such a clinical decision is made. The variability of the BTMs has improved significantly in recent years, and we propose that these markers, particularly plasma CTX and Procollagen type 1 N-terminal propeptide measured on automated platforms, can be used in routine clinical practice to assess treatment response.
Summary
In summary, osteoporosis is a multifactorial disease that is an important public health and financial problem, associated with increased mortality and morbidity. Recently released fracture risk prognostic tools incorporate BMD and other independent clinical risk factors to estimate an individual's absolute fracture risk, thus aiding treatment decisions. Management should address investigation for secondary causes of osteoporosis and correction of this where possible. Treatment should focus on both non-pharmacological and pharmacological measures. Bisphosphonates are currently recommended as first choice treatment to postmenopausal women and men aged more than 50 years, in accordance with the NICE guidelines, due to its cost effectiveness and broad spectrum fracture efficacy data. To date, there is no consensus on best practice when it comes to treatment monitoring. Both BMD and BTMs, when used appropriately, are clinically useful surrogates of antifracture effectiveness; however, limitations and benefits of both should be taken into account.
Take-home messages
-
Osteoporosis and osteoporosis-related fractures is a common disorder which affects 1 in 2 women and 1 in 5 men. It is a systemic skeletal disorder which occurs as a result of an imbalance between bone formation and bone resorption.
-
The WHO- designed fracture risk assessment tool (FRAX) calculates the 10-year probability of an osteoporotic fracture. This is computed from multiple extra-skeletal clinical risk factors with and without BMD at the femoral neck. It provides an aid in the assessment of an individual's fracture risk and in determining whether therapeutic intervention is required.
-
Osteoporosis is preventable and treatable. Treatment includes non-pharmacological as well as pharmacological intervention.
-
Non-pharmacological intervention includes modification of general lifestyle factors such as smoking cessation, avoidance of heavy alcohol use, ensuring regular weight-bearing exercise and optimum calcium/vitamin D intake.
-
Bisphosphonates and Denosumab are anti-resorptive agents. They decrease vertebral fractures as well as non-vertebral fractures. PTH analogues are anabolic and used in patients at very high risk of fracture who have failed therapy with anti-resorptives.
-
Monitoring response to therapy is important. Bone turnover markers, particularly serum-based markers such as serum CTX and P1NP have a role to play in assessing treatment efficacy and compliance.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.