Article Text

Abstract
Aims Activating mutations in the gene encoding epidermal growth factor receptor (EGFR) can confer sensitivity to EGFR tyrosine kinase inhibitors such as gefitinib in patients with advanced non-small-cell lung cancer. Testing for mutations in EGFR is therefore an important step in the treatment-decision pathway. We reviewed reported methods for EGFR mutation testing in patients with lung cancer, initially focusing on studies involving standard tumour tissue samples. We also evaluated data on the use of cytology samples in order to determine their suitability for EGFR mutation analysis.
Methods We searched the MEDLINE database for studies reporting on EGFR mutation testing methods in patients with lung cancer.
Results Various methods have been investigated as potential alternatives to the historical standard for EGFR mutation testing, direct DNA sequencing. Many of these are targeted methods that specifically detect the most common EGFR mutations. The development of targeted mutation testing methods and commercially available test kits has enabled sensitive, rapid and robust analysis of clinical samples. The use of screening methods, subsequent to sample micro dissection, has also ensured that identification of more rare, uncommon mutations is now feasible. Cytology samples including fine needle aspirate and pleural effusion can be used successfully to determine EGFR mutation status provided that sensitive testing methods are employed.
Conclusions Several different testing methods offer a more sensitive alternative to direct sequencing for the detection of common EGFR mutations. Evidence published to date suggests cytology samples are viable alternatives for mutation testing when tumour tissue samples are not available.
- EGFR
- Lung Cancer
- Cytology
- Methodology
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
Lung cancer is the most frequently diagnosed of all cancers and is responsible for approximately 1.38 million deaths each year worldwide.1 Non-small-cell lung cancer (NSCLC) is the most common form of lung cancer and first-line treatment of advanced NSCLC often involves platinum-based combination chemotherapy.2 However, for patients with advanced NSCLC harbouring an activating mutation in the tyrosine kinase (TK) domain of the epidermal growth factor receptor (EGFR), targeted treatment is available in the form of the EGFR TK inhibitors (TKIs) gefitinib and erlotinib.
Activating somatic mutations in the EGFR gene conferring sensitivity to EGFR TKIs were first reported in 2004.3–5 Since then, the efficacy of first-line gefitinib and erlotinib in patients with EGFR mutation-positive advanced NSCLC has been demonstrated in a number of Phase III trials.6–11 In the Iressa Pan-Asia Study, progression-free survival (PFS) was significantly longer with gefitinib than carboplatin/paclitaxel for patients whose tumours harboured activating EGFR mutations. In patients with wild-type EGFR, carboplatin/paclitaxel was associated with significantly longer PFS than gefitinib.8 The conformational change seen in the TK domain of mutated EGFRs increases the activation of the domain and its affinity for ATP (and EGFR TKIs) compared with wild-type EGFR.3The resulting increase in binding of EGFR TKIs produces greater inhibition of the domain and blocking of signal transduction pathways implicated in the proliferation and survival of cancer cells. Gefitinib also improved PFS versus chemotherapy in two Phase III trials performed solely in patients with EGFR mutation-positive advanced NSCLC.6 ,7 In addition, in two Phase III erlotinib trials that recruited EGFR mutation-positive patients, PFS was significantly increased with first-line erlotinib relative to chemotherapy.9 ,10 As a result of these data, the accurate identification of patients who might benefit from EGFR TKI therapy has become an important step in the treatment-decision pathway for advanced NSCLC.9 ,12
Mutations associated with enhanced sensitivity to EGFR TKIs are found in exons 18–21 of the TK domain of EGFR.3 ,4 Two types of mutation—short in-frame deletions in exon 19, clustered around the amino-acid residues 747–750 and a specific exon 21 point mutation (L858R)—have been reported to comprise up to 90% of all activating EGFR mutations.3 ,4 ,13 Other activating mutations include point mutations in exon 18 (including mutations in codon 719) and point mutations and in-frame insertions in exon 20 (including T790M). The prevalence of EGFR mutations differs according to ethnicity; approximately 10–12% of non-Asian patients with advanced NSCLC harbour these mutations compared with 30–40% of Asian patients.14–16
Historically, the standard for EGFR mutation testing involved direct sequencing of DNA extracted from samples of tumour tissue gathered during biopsy or resection, usually in the form of formalin-fixed paraffin-embedded (FFPE) diagnostic blocks. Direct sequencing, however, has low sensitivity (ie, only detects mutations when sufficient levels of mutant DNA are present), can be complex and time-consuming, and is not standardised in terms of laboratory practice.17 ,18 A number of alternative methods for mutation testing have been developed and used over recent years, many with improved sensitivity and turnaround times. Another area of active research has been the evaluation of alternative sources of tumour material. As many patients with lung cancer are not identified until they have advanced disease, the procedures required to obtain a tumour biopsy sample for diagnosis may not always be possible due to co-morbidities or other reasons. Instead, cytology samples can be collected as they are adequate for the diagnosis and staging of the disease, and the procedures used to obtain these samples are generally less invasive than those used to obtain a biopsy sample. In this regard, the use of cytology samples collected for diagnostic purposes or as a result of disease complications (eg, pleural effusion (PLE)) has attracted particular attention.19
The first objective of this review was to identify and compare reported methods for EGFR mutation testing in patients with lung cancer. We focused on studies involving samples of biopsied or resected tumour tissue for this purpose because, in comparison with other sources of tumour DNA, such samples have traditionally been considered the standard for mutation testing. Our second objective was to evaluate published data on EGFR mutation testing in cytology samples when used to diagnose lung cancer in an effort to determine whether such specimens are viable alternatives to standard tumour tissue samples.
Literature search methodology
A MEDLINE database search was performed on 27 April 2012 to identify original study articles reporting on methods for EGFR mutation testing in patients with lung cancer. The following search terms and criteria were used: (mutation detection methods lung (All fields) AND EGFR (Title/Abstract) AND mutation (Title/Abstract)) OR (EGFR (Title/Abstract) AND mutation (Title) AND lung (Title/Abstract) AND methods (Title/Abstract)) OR (EGFR mutation testing lung (All fields)) OR (EGFR (Title/Abstract) AND mutation (Title/Abstract) AND cytology (Title/Abstract)). Search results were filtered to exclude non-English language and review articles and the titles of the remaining 284 articles were reviewed to identify potentially relevant articles. Abstracts of such articles (n=106) were reviewed and 59 studies that met one or both of the following criteria were selected for inclusion: (1) studies using ‘standard’ tumour tissue samples that assessed an EGFR mutation testing method and one or more ‘comparator’ methods; (2) studies reporting the use of cytology samples for EGFR mutation testing. Both groups excluded studies that only investigated non-TKI-sensitive EGFR mutations (ie, the exon 20 point mutation T790M alone) and those involving fewer than 20 samples.
EGFR mutation testing methods in tumour tissue samples
Our literature search identified 30 studies that assessed the utility of an EGFR mutation testing method and comparator method(s) using 20 or more tumour tissue samples (table 1). Methods were assigned into one of two broad categories: ‘screening’ methods that detect all mutations, including novel variants, in exons 18–21 and 'targeted’ methods that detect specific, known mutations. The advantages and disadvantages of screening and targeted testing methods are summarised in table 2.
Studies of EGFR mutation testing methods using ‘standard’ tissue samples collected from patients with lung cancer
Advantages and disadvantages of screening and targeted methods for EGFR mutation testing
Screening methods
Table 1 includes six studies investigating the use of screening methods as alternatives to direct sequencing. In the study of Sueoka and colleagues, mutation testing results obtained by denaturing high-performance liquid chromatography (dHPLC) analysis of frozen tissue samples were consistent with those obtained by direct sequencing.20 These authors reported that the analysis time for dHPLC was a quarter of that for direct sequencing. When combined with a DNA endonuclease-based technique, HPLC was shown to have 100% analytical sensitivity and negative predictive value relative to direct sequencing.21 A technique related to dHPLC, high-resolution melting analysis (HRMA), exhibited 100% sensitivity and 90% specificity versus direct sequencing.22 Similarly high sensitivity and specificity versus sequencing was reported for HRMA by Takano and colleagues, although this group used HRMA as a targeted method.23 Another study utilising HRMA reported identical EGFR mutation frequency rates to direct sequencing.24 An alternative next-generation sequencing methodology, massively parallel sequencing, was validated in a study by Querings and colleagues.25 This group reported a 100% success rate of this method to detect low-frequency EGFR mutations compared with 89% for pyrosequencing—a non-electrophoretic sequencing technology employing luminometric detection—and 67% for direct sequencing.25
Targeted methods
The results of 24 studies that assessed targeted methods for detection of common EGFR mutations are shown in table 1. The majority of these studies investigated the use of PCR-based methods to specifically detect exon 19 deletions, the exon 21 L858R point mutation, and, in some cases, other less common but known EGFR mutations.26–40 In these studies, which varied in their use of frozen and/or FFPE tissue samples, virtually all samples testing positive for known mutations by direct sequencing were also detected by the PCR-based screening methods under investigation. Moreover, the targeted methods detected mutations in samples that had tested negative by direct sequencing. For example, the Amplification Refractory Mutation System (ARMS)—a commonly used method that discriminates between mutated and wild-type DNA by selectively amplifying mutation-containing target sequences—detected over twice as many exon 19 deletions and L858R mutations than direct sequencing in a study by our group.31 However, direct sequencing detected additional mutations not designed to be identified by the specific ARMS reactions. Another method commonly used is fragment length analysis; in the study of Pan and colleagues, this method detected more exon 19 deletions than direct sequencing.36 Pyrosequencing has also shown higher analytical sensitivity than direct sequencing for the two most common EGFR mutations; the accuracy of this method, however, was only maintained when samples contained at least 20% tumour cells.38 One novel technique adapted for PCR-based mutation detection is cationic conjugated polymer (CCP)-based fluorescence resonance energy transfer (FRET).40 This method, in which FRET probes bind to nested PCR-amplified products, detected EGFR mutations with comparable sensitivity (95%) and specificity (96%) to direct sequencing and RT-PCR.40
Non-PCR-based targeted methods listed in table 1 include Smart Amplification Process (SmartAMP), a one-step mutation-detection technology that enables precise amplification of only target sequences.42 In a study by Hoshi and colleagues, SmartAMP and direct sequencing showed high concordance when used to assess frozen clinical samples for the two most common EGFR mutations and the exon 18 G719S point mutation.41 A modification of this technique, peptide nucleic acid (PNA)-clamp SmartAmp2, in which oligomers of PNA (a synthetic DNA analogue) bind to wild-type DNA sequences spanning mutational hotspots, preferentially allowing for mutant DNA amplification,39 has been investigated in two studies.42 ,43 One study found that PNA-clamp SmartAmp2 was more sensitive than direct sequencing at detecting the two main EGFR mutations using both frozen and FFPE tissue samples.42 Similarly, a second study reported greater sensitivity of this technique compared with direct sequencing, PNA-enriched sequencing, and conventional SmartAmp2.43
Several of the studies listed in table 1 used immunohistochemistry (IHC) for the targeted mutation analysis of tissue samples.44–49 These studies utilised two mutant-specific rabbit monoclonal antibodies directed against the exon 19 A746_A750 deletion and L858R, and most reported high sensitivity and specificity for mutant-specific IHC versus direct sequencing and/or other comparator methods.
Use of cytology samples for EGFR mutation testing
In total, 33 original studies reporting the use of cytology samples for EGFR mutation testing were identified by our literature search (table 3). Commonly tested cytology samples included tissue samples collected during diagnosis (eg, fine needle aspirate (FNA) samples acquired via minimally invasive biopsy procedures, which often contain high proportions of tumour cells) or liquid-based samples obtained from patients experiencing common complications of lung cancer (eg, PLE, which often have low tumour cell content). Use of sensitive mutation testing methods is warranted when cytology samples with low tumour content are used. In two separate studies, EGFR mutations detected by mutant-enriched PCR in some PLE samples were not detected by non-enriched assays.29 ,50 Similarly, the sensitive ARMS technique has been shown to detect mutations in PLE samples not identified via direct sequencing.51 Interestingly, the detection rate of EGFR mutations with direct sequencing improved from 45% when using genomic DNA to 67% when using tumour-derived RNA isolated from PLE samples as an alternative source.52 ARMS was also more sensitive than direct sequencing in studies utilising transbronchial FNA.53 Our search showed that the use of FNA for detection of EGFR mutations has been relatively widely investigated (table 3). Several FNA-generating techniques used for the diagnosis and staging of lung cancers have attracted particular interest in this regard: endobronchial ultrasound-guided fine needle aspiration (EBUS-FNA), trans-oesophageal ultrasound-guided fine needle aspiration (EUS-FNA), and CT-guided FNA. Cytology samples obtained via these techniques were successfully assessed for EGFR mutations using direct sequencing.54 ,55 Other studies have reported the successful use of EBUS-FNA and/or EUS-FNA samples with real-time PCR,56 ,57 COLD-PCR,58 PNA-locked nucleic acid (LNA) PCR clamp,59 or loop-hybrid mobility shift assay.60
Studies of EGFR mutation testing methods using cytology samples collected from patients with lung cancer
Discussion and future perspectives
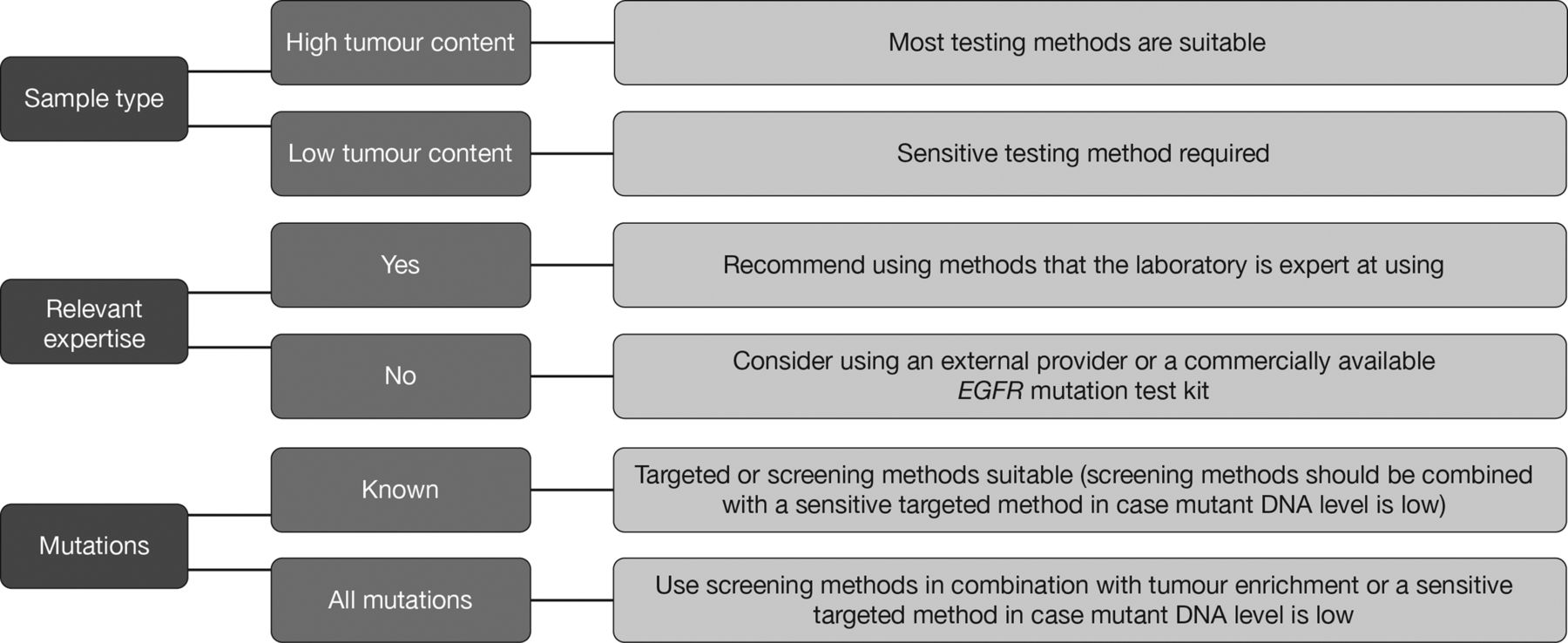
A variety of methods have been employed as potential alternatives to the historical standard for EGFR mutation testing, direct sequencing. In practice, the choice of testing method should be based primarily on the nature of the sample to be tested including tumour content (particularly for cytology material), the testing laboratory's expertise and available equipment, and whether detection of known activating EGFR mutations only is considered sufficient (figure 1).
{kind=link}
Factors determining the choice of EGFR mutation testing method.
Reflecting its position as the historical standard, direct sequencing was used as the comparator method in many of the studies identified by our search. The variability observed between studies when comparing sequencing to other mutation testing methods may be due to technical differences, such as primers or reagents used by individual laboratories. Perhaps the primary limitation of direct sequencing is its low sensitivity; indeed, a mutation should generally be present in approximately 20% of all DNA in a sample to be reliably detected by this method.78 ,79 In our experience, the approximate tumour content of lung tissue samples can range from 5 to 100%. Therefore, a limit of detection of 20% means that direct sequencing may offer insufficient sensitivity.80 Preparation of samples by macro-dissection or laser capture micro-dissection prior to DNA extraction, however, can enrich tumour cell content and thereby increase the utility of sequencing as a routine pre-treatment test.81 While relatively cost-effective from a reagent perspective compared with targeted methods,82 these preparatory enrichment methods are labour intensive and time consuming and provide a relatively marginal improvement. Alternative screening methods to direct sequencing include dHPLC and HRMA. Although dHPLC appears to have higher analytical sensitivity than direct sequencing,20 dHPLC requires extra processing steps after PCR amplification and the use of expensive instrumentation.22 HRMA has been proposed as an alternative, and is able to detect mutant genes at levels of 2.5–10%.22 ,24 HRMA is relatively inexpensive; however, samples testing positive by HRMA must then be analysed by direct sequencing to ensure that mutations are properly identified.24 This can be problematic when levels of mutant DNA do not permit analysis by direct sequencing.
Targeted methods, which detect specific mutations only, tend to be more sensitive in terms of limit of detection than screening techniques. ARMS, for example, is a simple PCR-based testing method shown to be more sensitive and robust than direct sequencing for the assessment of common EGFR mutations in FFPE tumour tissue.31 One other targeted method to be validated is fragment length analysis. While fragment length analysis is used widely in practice, it can only detect insertions or deletions and does not allow detection of point mutations in EGFR. Compared with some other methods, mutant-specific IHC is fast, cost-effective, and can be performed in most pathology laboratories.44 IHC, however, has not been widely adopted for EGFR mutation analysis amid concerns that it is not as sensitive or as specific as DNA-based molecular techniques. A study comparing EGFR mutation testing between 15 centres in France (the Evaluation of the EGFR Mutation Status for the Administration of EGFR-TKIs in Non-Small Cell Lung Carcinoma (ERMETIC) project) suggested that detection accuracy is dependent upon sample quality rather than the sequencing method used, highlighting the importance of good sample collection and processing techniques.83 For poor quality samples, care must be taken to ensure the selection of tumour cells, in addition to the DNA concentration, as test results are frequently dependent on both these parameters.
The availability of targeted methods with high sensitivity offers the potential for accurate, rapid, and high-throughput analysis of clinical samples. The main theoretical drawback of these techniques is their inability to detect all activating EGFR mutations. The majority of clinical evidence to date robustly supports the use of EGFR TKIs in patients with the two most common activating mutations in EGFR (exon 19 deletions and the L858R point mutation in exon 21), and most targeted methods are specifically designed to detect these mutations. However, clinical data on less common mutations are emerging and further research is required to fully inform predictable outcomes on EGFR TKIs, aided by the use of sample micro dissection followed by screening methods, to ensure identification of all known mutations.18 While targeted methods can fail to detect some of the rare mutations which are detected by screening, it is anticipated that rare mutations demonstrated to have therapeutic implications will subsequently be included in targeted screening approaches, thus ensuring all patients will benefit from the appropriate therapy. Both screening and targeted methods have been used to identify EGFR mutations in clinical trials of EGFR TKIs in patients with advanced NSCLC.6–10 14–16 ,84 These trials were not identified by our search due to our focus on method comparison studies. In practice, laboratories can opt to use commercially available kits or to develop their own tests. Testing kits such as those utilising the ARMS method have the advantages of being validated, ready for use and quality controlled. Laboratory-developed tests, many of which were identified by our search, may be less expensive, but take time to develop and validate and may have limited quality control. If procedures for EGFR mutation testing are not established at a local level, use of one of a number of global testing laboratories may be considered. Such laboratories use a variety of methods for EGFR mutation testing including commercially available kits and laboratory-developed tests.
Our literature search confirmed that cytology samples are suitable testing material for EGFR mutation testing and that detection rates appear to be as high as those obtained with traditional tissue samples. The suitability of cytology samples for routine clinical practice has been recognised in published recommendations for EGFR mutation testing.85 Of note, in the recent study of Goto and colleagues, published after we performed our literature search, five different EGFR testing methods (PCR-Invader, PNA-LNA-PCR clamp, PCR-direct sequencing, cycleave PCR, and ARMS) showed comparable performance in the assessment of tissue and cytology samples. Furthermore, the concordance between matched tumour and cytology samples was extremely high.86
There is a growing trend toward the extensive molecular characterisation of tumours so that the most appropriate therapy can be selected. This is exemplified in the Biomarker-integrated Approaches of Targeted Therapy for Lung cancer Elimination trial, in which patients are adaptively randomised to various treatments based on relevant molecular biomarkers.87 This approach has been made possible by the availability of methods such as Sequenom MassArray,88 SNaPshot,89–91 and arrays of mutation-specific PCR assays (eg, qBiomarker Somatic Mutation PCR Array), and through the use of next-generation sequencing. These methods can rapidly and sensitively detect many known mutations in a relatively small amount of DNA. Using such gene panel approaches will no doubt increase our knowledge of pharmacogenetic predictive biomarkers and therefore improve patient outcomes by ensuring that each patient is given a treatment with the most likely chance of success. To date, no point-of-care devices are available for EGFR mutation testing; the future development of such devices would be welcome and would help ensure that treatment is not delayed while test results are awaited.
Conclusions
The EGFR mutation testing landscape is varied and includes a number of screening and targeted methods. Each method has its own benefits and limitations and the choice of method used in practice should be made according to the nature of the sample to be tested, the testing laboratory's expertise and access to equipment, and whether detection of known activating EGFR mutations only or all possible mutations is required. Cytology samples can be used to reliably detect EGFR mutations. Mutation detection rates with cytology samples are comparable with those achieved with traditional tissue samples obtained by biopsy or resection.
Key messages
-
The development of targeted EGFR mutation testing methods and commercially available test kits has enabled sensitive, rapid and robust analysis of clinical samples from patients with NSCLC.
-
The use of screening methods, either used alone or in conjunction with targeted methods, enables the detection of more rare and novel EGFR mutations.
-
Evidence published to date suggests cytology samples (including fine needle aspirate and pleural effusion) are viable alternatives for mutation testing when tumour tissue samples are not available.
-
The choice of method used in practice should be made according to the nature of the sample to be tested, the testing laboratory’s expertise and access to equipment, and whether detection of known activating EGFR mutations only or all possible mutations is required.
Acknowledgments
Medical writing support was provided by Rick Flemming, PhD, CMPP and Annette Smith, PhD of Complete Medical Communications, and was funded by AstraZeneca.
References
Footnotes
-
Contributors All authors made substantial contributions to the conception, design and execution of the review and interpretation of the data. All authors contributed to the intellectual content of the manuscript, reviewed and critically revised it and approved of the final submitted version.
-
Funding This study, including design, collection/analysis/interpretation of data, writing, and decision to submit this manuscript for publication was supported by AstraZeneca.
-
Competing interests GE, GZ, AM, SD, GS, and RM are full-time employees of AstraZeneca. GE, SD, GS, and RM are holders of AstraZeneca shares.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/