Article Text

Abstract
Aims The goal of this study is to create an objective pathological diagnostic system for blood and lymphatic vessel invasion (BLI).
Methods 1450 surgically resected colorectal cancer specimens from eight hospitals were reviewed. Our first step was to compare the current practice of pathology assessment among eight hospitals. Then, H&E stained slides with or without histochemical/immunohistochemical staining were assessed by eight pathologists and concordance of BLI diagnosis was checked. In addition, histological findings associated with BLI having good concordance were reviewed. Based on these results, framework for developing diagnostic criterion was developed, using the Delphi method. The new criterion was evaluated using 40 colorectal cancer specimens.
Results Frequency of BLI diagnoses, number of blocks obtained and stained for assessment of BLI varied among eight hospitals. Concordance was low for BLI diagnosis and was not any better when histochemical/immunohistochemical staining was provided. All histological findings associated with BLI from H&E staining were poor in agreement. However, observation of elastica-stained internal elastic membrane covering more than half of the circumference surrounding the tumour cluster as well as the presence of D2-40-stained endothelial cells covering more than half of the circumference surrounding the tumour cluster showed high concordance. Based on this observation, we developed a framework for pathological diagnostic criterion, using the Delphi method. This criterion was found to be useful in improving concordance of BLI diagnosis.
Conclusions A framework for pathological diagnostic criterion was developed by reviewing concordance and using the Delphi method. The criterion developed may serve as the basis for creating a standardised procedure for pathological diagnosis.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Blood and lymphatic vessel invasion (BLI) in colorectal cancer (CRC) are known to be strong risk factors correlated with poor outcome. Since it was first reported by Brown et al in 1938, numerous studies have been conducted on BLI. BLI is adopted in TNM Classification of Malignant Tumours and College of American Pathologists Consensus Statement in pathology reports.1–4 Assessment of BLI enables identifying patients with high risk within the same TNM stage and therapeutic strategy can be tailored accordingly, especially for patients with Stage II CRC and patients with endoscopically resected pT1.5–7 Observation of BLI, however, is also known for its weakness, which is high interobserver variability. Many articles report poor interobserver concordance of BLI assessment and no solution has been offered so far.8–10 One solution may be to use elastica for histochemical staining or D2-40 for immunohistochemical staining of internal elastic lamina of vessel and lymphatic endothelium.11–15 Another solution may be to take a conventional approach to develop a framework for diagnostic criterion, through formal procedure to reach consensus, gain support and understanding of pathologists worldwide.16 It was under this concept that pathologists belonging to the Japanese Society for Cancer of the Colon and Rectum decided to join hands and took a comprehensive approach as follows: (1) review current practice of pathologists’ assessment including sampling methods, staining methods and BLI in different medical institutions (2) evaluate concordance of BLI diagnosis and histological findings associated with BLI (3) develop a framework for diagnostic criterion using the Delphi method, with data from current practice and (4) conduct a concordance study to evaluate the usefulness of the new criterion. Our attempt was to develop a framework for an objective criterion to assess BLI, in order to improve concordance in all settings.
Materials and methods
Multicentre, retrospective review of pathological assessment at different departments of pathology
A total of 1450 patients with CRC who underwent surgical resection in 2003 from eight institutions under the Japanese Society for Cancer of the Colon and Rectum were reviewed. Clinicopathological factors including the TNM stage according to the fifth edition of TNM classification,3 the presence of BLI, number of paraffin blocks taken to examine primary tumours, use of megablock, tangential tissue sectioning, histochemical staining and immunohistochemical staining were reviewed and compared.17 The range of histochemical staining and antibody used for immunohistochemical staining were also reviewed.
Interobserver study
Eighty consecutive, surgically resected specimens of Stage II CRC according to the seventh edition of TNM classification4 between 2003 and 2005 from the National Cancer Center Hospital East were used for the interobserver study. Eight pathologists from eight institutions assessed the slides. Specimens for pathological assessment were divided into six cohorts as follows (table 1) and concordance of diagnosis was reviewed. Cohort 1: H&E-stained slides without any guiding criteria. Cohort 2: H&E-stained slides without any criteria, but focus on designated area of lesion. Assessment was later checked to see which histological findings associated with BLI had good agreement. Concordance of assessment for designated area was also reviewed (figure 1). Cohort 3: H&E-stained, elastica-stained and D2-40-stained slides. Histochemical and immunohistochemical staining without any guiding criteria. Cohort 4: H&E-stained, elastica-stained and D2-40-stained slides. Histochemical and immunohistochemical staining without any guiding criteria but focus on designated area of lesion (figure 1). Observation was later checked to determine which slides of H&E, histochemical or immunohistochemical staining associated with BLI diagnosis had good concordance. Concordance of assessment for designated area of lesion was also reviewed. Cohort 5: H&E-stained, elastic-stained and D2-40-stained slides. Histochemical and immunohistochemical staining and our new criterion were used for assessment. Finally, for Cohort 6, the same H&E-stained, elastic-stained and D2-40-stained slides used in Cohort 3 were assessed by the pathologists (who were unaware of reviewing the same slides) to check diagnostic agreement of histochemical and immunohistochemical staining using our new criterion. Cohorts 1, 3, 5 and 6 each consisted of 20 CRC specimens and Cohorts 2 and 4 each consisted of 10 CRC specimens. H&E-stained slides and slides of largest slice from blocks of specimen including the deepest invasive area of tumour were used in Cohorts 1, 3, 5 and 6, while one representative slide of the tumour was used in Cohorts 2 and 4. In Cohorts 2 and 4, assessment of designated area was reviewed to evaluate the agreement of BLI diagnosis. Three areas of lesion containing histological tumour cluster surrounded by some space or fibrous rim-like vascular structure were chosen randomly and marked with ink. Since the designated area was very small, virtual slides were used to indicate with an arrow where assessment should be made (figure 1). In Cohorts 1, 3, 5 and 6 the ‘presence’ or ‘absence’ of BLI was reported. In Cohorts 2 and 4, assessment of designated area was made as ‘blood vessel invasion’, ‘lymphatic vessel invasion’ or ‘neither’. In Cohorts 2 and 4, histological findings associated with the diagnosis of BLI were collected. This was reviewed thoroughly in a meeting and was recorded in the survey sheet, as either ‘present’ or ‘absent’ (table 2).
Details of cohorts and concordance of blood and lymphatic vessel invasion (BLI)
Concordance of histological findings associated with the blood and lymphatic vessel invasion

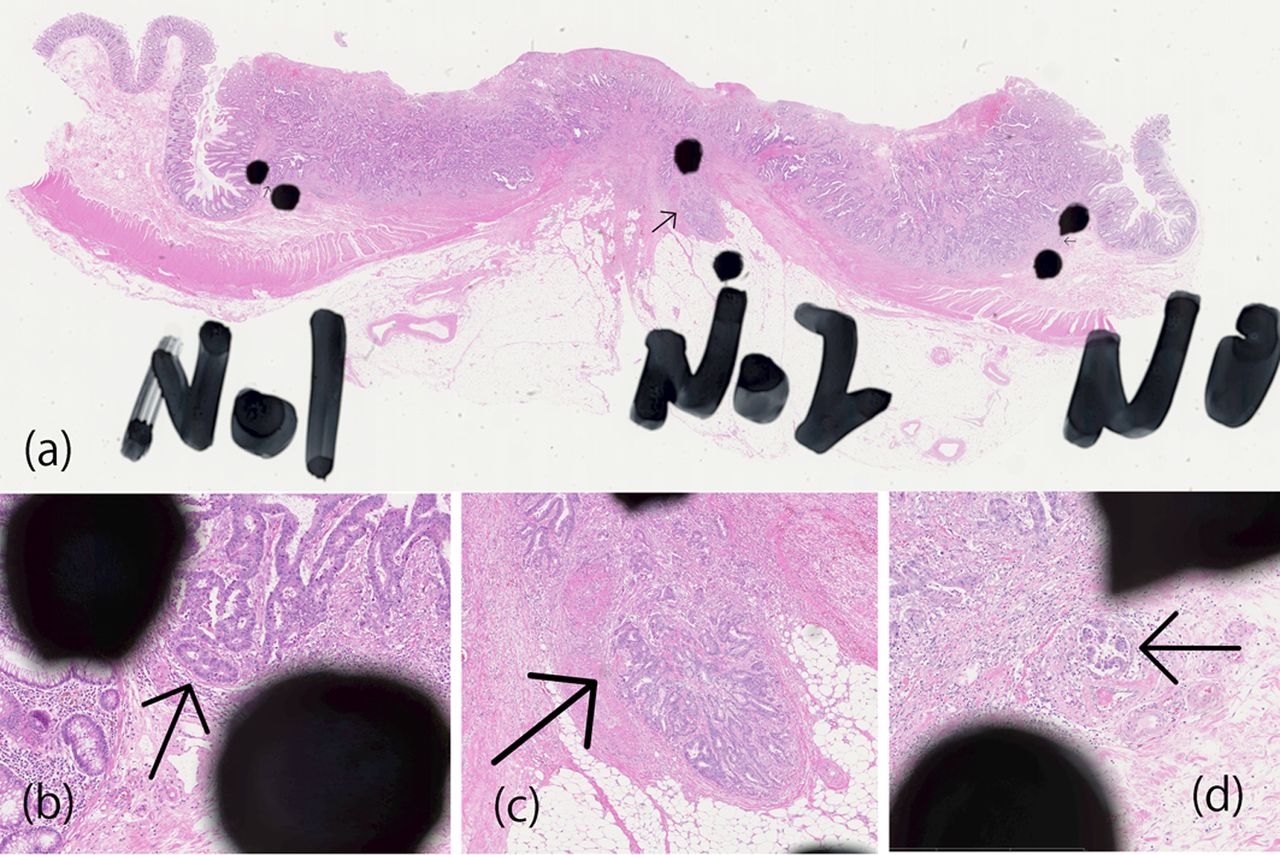
(A–D) A case from Cohort 2. In Cohorts 2, 4, three regions of interest within the histological tumour cluster with surrounding space or fibrous rim-like vascular structure were chosen randomly and marked with ink near the lesion (A). The lesion to be reviewed was indicated with an arrow on the virtual slides (B–D). Eight pathologists reviewed the slides. The assessment for each of the indicated lesions was reported as ‘blood vessel invasion’, ‘lymphatic vessel invasion’ or ‘neither’. Furthermore, pathological findings associated with the diagnosis of blood and lymphatic vessel invasion were studied. Reviewers recorded their interpretations of the indicated lesion using the query sheet, answering the questions as ‘present’ or ‘absent’.
Developing diagnostic criteria using the Delphi method
Four rounds of consensus meetings, participated by eight pathologists were held as shown in figure 2. Before the meeting, a survey on histological, histochemical and immunohistochemical diagnostic criteria of BLI was prepared. All pathologists were requested to answer the survey anonymously and send it by mail after the meeting.16 There were a total of 34 questions: 2 on the definition of BLI, 7 on the assessment of BLI, 4 on the use of histochemical and immunohistochemical staining, 8 on assessment of blood vessel invasion and 13 on the assessment of lymphatic vessel invasion (table 3). Scoring was based on 1 to 6 Likert scale (1=strong disagreement, 2=moderate disagreement, 3=some disagreement, 4=some agreement, 5=moderate agreement, 6=strong agreement), maximum score being 6 points. Scores of 5 and 6 were regarded as ‘agreement’. Consensus was considered to be achieved when over 80% of the participants’ scores resulted in ‘agreement’, based on the previously described scoring method.18–20 Four rounds of meetings with active discussion took place and surveys were conducted three times, after the second and third rounds of meetings, as shown in figure 2. At the beginning of the second and third rounds of meetings, interim results of survey were reported to the participants to facilitate building consensus on key histological findings with high concordance. For findings that failed to present immediate agreement, further discussion took place and the next vote was performed. Consistent with the Delphi method, some questions in the survey were modified to enable building general agreement.18 After the third round of meetings, the findings for which consensus had been reached were summarised and new diagnostic criterion was developed.
Queries and consensus-building using the Delphi method

Time flow for consensus development.
Statistical analysis
The concordance reached by pathologists on rating tumour invasion was evaluated using κ coefficients. Using %mκ SAS macro, we estimated the Fleiss type multi-rater κ coefficient and corresponding 95% CI.21 All statistical analyses was performed with SAS Release V.9.3 (SAS Institute, Inc, Cary, North Carolina, USA).
Results
Multicentre retrospective review of current practice of pathological assessments
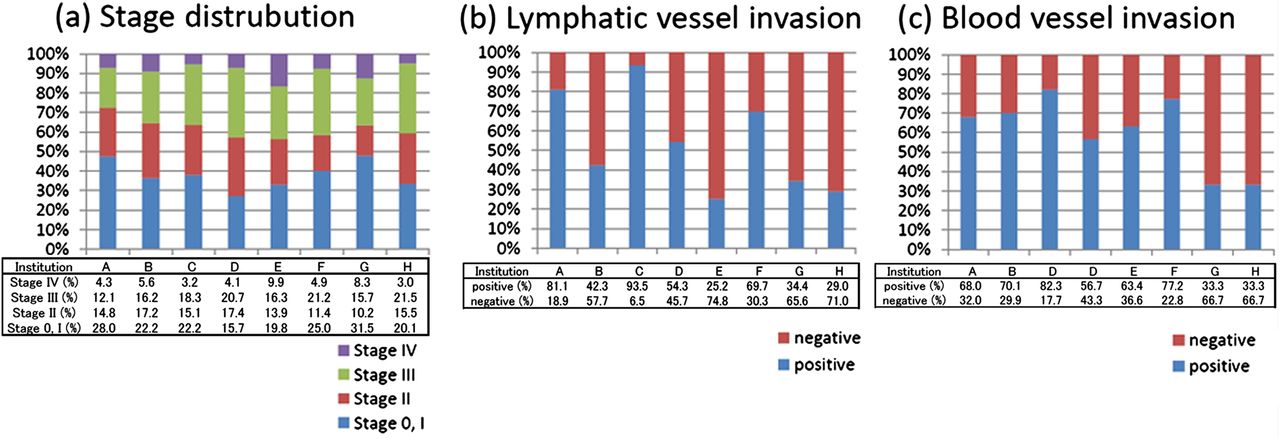
The result of the study is shown in table 4 and figure 3. The total number of cases reviewed in this study by eight institutions ranged from 54 to 441, of which 51.0–72.5% were colon cancer, 53.5–68.0% were male patients, and their average age was between 63 years and 68 years. The average number of paraffin blocks used for primary tumour pathological assessment varied widely among institutions, ranging from 4.8 blocks to 34.4 blocks. Use of histochemical staining and immunostaining was also different among eight institutions. And the range of histochemical staining performed was also different. Antibody used in immunohistochemical staining was D2-40 in three institutions. And one institution used D2-40 and alpha-smooth muscle actin (SMA). Figure 3 shows the results of a retrospective review of the stage and assessment of BLI. Although the stage distributions were similar among the eight institutions (Stage 0, I; 19.8–28.0%, Stage II; 10.2–17.4%, Stage III; 12.1–21.5% and Stage IV; 3.0–9.9%), substantial difference was noted on the presence of BLI (lymphatic vessel invasion; 18.9–74.8%, blood vessel invasion; 17.7–66.7%). None of the institutions in this study used megablock or tangential sectioning.
Current practice of pathological assessment at the department of pathology in different medical institutions in 2003
{kind=link}
{kind=link}
{kind=link}
(A) Stage distribution of 1450 surgically resected colorectal cancer (CRC) cases among eight hospitals. (B) Distribution of positive cases of lymphatic vessel invasion among 1450 surgically resected CRC cases from eight hospitals. (C) Distribution of positive cases of blood vessel invasion among 1450 surgically resected CRC cases from eight hospitals.
Interobserver study and development of diagnostic criterion using the Delphi method
The result of the interobserver study is shown in table 1. After the first round of meeting, Cohorts 1 and 2 were given only H&E stained slides without any additional staining or guiding criteria. The concordance of assessment of blood vessel invasion was moderate and it was low for lymphatic vessel invasion. This was not any better when pathologists in Cohort 2 were asked to focus on the designated area. Furthermore, the concordance of all histological findings associated with BLI was low in Cohort 2 (table 2). Diagnosis of BLI is based on multiple histological findings considered to be associated with BLI, most of which were included in this study as shown in table 2. Consistent diagnosis of BLI only with H&E-stained slides seemed to be difficult to achieve and this was informed to the pathologists during the second round of meetings. It was then decided to distribute H&E-stained slides as well as the histochemical and immunohistochemical staining, without any guiding criteria (Cohorts 3 and 4). Although this increased positive findings of blood vessel invasion in Cohort 3, it did not improve the concordance of BLI diagnosis. In Cohort 4, concordance improved for the designated area. Interestingly, we found few histochemical and immunohistochemical findings associated with the diagnosis of BLI having good agreement (table 2). This was reported to pathologists during the third round of meetings and it was agreed that they should be included in the diagnostic criteria of BLI (table 3). Pathologists summarised the findings which they were able to agree upon and new diagnostic criterion was developed with active discussion (box 1). Finally, the use of the new criterion was evaluated with Cohorts 5 and 6. There was a remarkable improvement in concordance in Cohort 5 (κ=0.547 for blood vessel invasion, κ=0.492 for lymphatic vessel invasion), as well as in Cohort 6 (κ=0.617 for blood vessel invasion, κ=0.618 for lymphatic vessel invasion), which used the same slide as in Cohort 3 (κ=0.502 for blood vessel invasion, κ=0.153 for lymphatic vessel invasion). This serves as direct evidence on the usefulness of new criterion in improving agreement in BLI diagnosis (table 1).
Discussion
The need for a diagnostic criterion which enables a standardised and objective diagnosis is clear. Our attempt was to provide a framework for developing a consensus-based criterion to be used in different pathological settings through this study. BLI are distinct pathological factors and have different clinicopathological implications.22 There are, however, some common morphologies such as the presence of endothelium or cavity, and distinct identification of small venules and lymphatic vessel is often difficult. There is also the problem of interobserver variability.2 BLIs are strong risk factors in many types of cancer. In CRC, BLIs can be used as a criterion to determine the need for adjuvant therapy in Stage II cases, which account for a significant proportion of CRC cases (27.1% in this study). For endscopically resected pT1 cases, BLIs are reported to be risk factors of lymph node metastasis and can be used as a criterion for making a decision of surgical resection. In this study, we tried to solve interobserver variabilities in BLI. The criterion that we developed may be useful for achieving more consistent diagnosis. Pathological assessment is generally inexpensive and is available at many hospitals. So introducing a standardised pathological diagnosis can be a major contribution to current medical practice. So far, poor agreement has been reported on BLI diagnosis in many organs and conducting a multicentre study using BLI may be difficult. There are some criteria suggested by pathologists on vascular invasion and some of them were incorporated into our criterion.23 ,24 While findings of H&E-stained slides should be further reviewed to search for findings with high concordance, developing objective criteria based only on H&E staining may be difficult. BLI and many pathological diagnoses are based on multiple associated histological findings. Therefore, investigation of the concordance in the histological findings associated with the diagnosis of BLI in our framework was an important step. And the problem of diagnostic threshold or retraction artefacts remains unsolved and may be one of the reasons for poor concordance.9 Elastica- staining and D2-40 staining have been reported to be useful in detecting BLI but may not always be associated with the detection of patients with higher risk.14 ,25 Review of histochemical and immunohistochemical findings in this study suggested key findings with high concordance which may improve the quality of pathological diagnosis. Although the use of these stains alone may be insufficient, it can be used in combination with diagnostic criterion. D2-40 immunostaining was seen in lymphatic endothelium and in fibroblasts. D2-40-positive endothelial cells (but not D2-40 positive cells) was another important finding with high concordance.26 Although histological variation was reported in blood vessel invasion, elastica-stained internal elastic membrane is the most important feature having consistent results.27 Careful attention should be paid, however, to the lesion such as myenteric plexus ganglia invasion mimicking blood vessel invasion so as not to misdiagnose as blood vessel invasion in H&E staining. Use of some additional markers may be beneficial to reduce misdiagnosis of BLI without D2-40 expression or internal elastic membrane in the future.
Most pathological criteria to date have been developed through an informal approach by group experts in various scientific committees. A more standardised approach needs to be taken to develop pathological criteria to be used in all kinds of clinical or pathological settings. By analysing the current practice of pathologists and using the Delphi method, we have developed a framework for a new pathological diagnostic criterion. Although it still may not be sufficient to be used in multicentre trials, significant improvement over current practice is expected. We invite other pathologists’ comment for its further revision and refinement. Routine elastica staining is low in cost and can be easily adopted by pathologists at different sites.28 The applications of the present study's criterion to the daily diagnosis of BLI will likely result in the accumulation of more consistent results regarding blood vessel invasion. Although routine use of our criteria of lymphatic vessel invasion may not be feasible for advanced CRC where multiple immunostaining is required for the assessment, it may be useful for endoscopically resected pT1 CRC which is small in size and only few blocks are required.29 The present report gives a set of criteria hopefully allowing a more consistent identification and reporting of BLI in CRC, and gives a template for the development of such diagnostic criteria that can be used in other areas of diagnostic pathology. Based on the framework that we propose, a more objective and consensus-based pathological diagnostic system can be created in many areas of diagnostic pathology.
Take home messages
-
Current practice of pathology assessment was varied among institutions in Japan.
-
Concordance was low for the pathological diagnosis of blood and lymphatic vessel invasion (BLI) in colorectal cancer, and was not any better when histochemical/immunohistochemical staining was provided.
-
All histological findings associated with BLI from H&E staining were poor in agreement. However, observation of elastica-stained internal elastic membrane covering more than half of the circumference surrounding the tumour cluster as well as the presence of D2-40-stained endothelial cells covering more than half of the circumference surrounding the tumour cluster showed high concordance.
-
Based on this observation, we developed a framework for pathological diagnostic criterion, using the Delphi method, which may serve as the basis for creating a standardised procedure for pathological diagnosis.
Established diagnostic criterion of blood and lymphatic vessel invasion (BLI) in Japanese society for cancer of the colon and rectum (JSSCR)
Definition
-
Lymphatic vessel invasion is defined as invasion of tumour cells into lymphatic vessels.
-
Blood vessel invasion is defined as invasion of tumour cells into blood vessels.
Assessment
-
Scanning at 4× magnification should be used to identify the suspected lesion. Then, further assessment should be made at higher magnification.
-
BLI should not be determined in lesions presenting spicula between the tumour nest and stroma.
Assessment of lymphatic vessel invasion
-
D2-40 positive vessel invasion should be determined as lymphatic vessel invasion, and the presence of D2-40 positive endothelial cells covering more than half of the circumference surrounding the tumour cluster should be the basis for diagnosis.
-
An indistinguishable lesion should not be determined as lymphatic vessel invasion.
Blood vessel invasion
-
In elastica staining, thick arteries surrounded by the tumour cluster should be identified. If elastica-stained internal elastic membrane covering more than half of the circumference surrounding the tumour cluster is present, the lesion should be diagnosed as blood vessel invasion.
-
Elastica positive vessel invasion should be determined as blood vessel invasion, and the presence of elastic-stained internal elastic membrane covering more than half of the circumference surrounding the tumour cluster should be the basis for diagnosis.
-
When the presence of elastica-stained internal elastic membrane covering more than half of the circumference surrounding the tumour cluster is identified, the lesion should be diagnosed as blood vessel invasion, even in the absence of accompanying artery, vascular structure or space.
Acknowledgments
The authors thank Sachiko Fukuda for her excellent technical assistance. We also thank Yoshiko Ohnuma and Motoko Suzaki for their secretarial help with the consensus meetings and the distribution of the slides. We also thank Mari Kanai and Yuri Kitayama for excellent English support.
References
Footnotes
-
Contributors Conception and design: MK, SN and AO. Administrative support: MK and AO. Collection and assembly of data: MK, SN and AO. Data analysis and interpretation: All authors. Manuscript writing: All authors. Final approval of manuscript: All authors
-
Funding This work was supported by the Japanese Society for Cancer of the Colon and Rectum (JSCCR).
-
Competing interests None.
-
Ethics approval This study was approved by the local research ethics committee of the National Cancer Center Hospital (No. 2010-100).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/