Article Text

Abstract
Aims Endotoxin detection assays are not validated for use in end-stage kidney disease (ESKD). We investigated the accuracy and precision of the kinetic turbidimetric Limulus amoebocyte lysate (LAL) assay to detect endotoxin in plasma from patients with ESKD. Optimisation of endotoxin recovery from plasma using the detergent Tween 80 was also explored.
Methods Plasma samples from 7 patients with ESKD and 7 healthy subjects were spiked with different concentrations of endotoxin. Repeated measurements for endotoxin at each level of spike were performed to assess the accuracy and precision of spike recovery. Endotoxin recovery in plasma samples diluted in Tween 80 and water was compared.
Results Mean endotoxin spike recovery was 111.6% and 125.2% in ESKD and healthy subjects, respectively. There was no statistical difference in spike recovery between ESKD and healthy plasma. Precision of the LAL assay in plasma spiked with low (0.05 EU/mL) and high (0.5 EU/mL) concentration of endotoxin spikes was 24.1% and 8.9%, respectively. The use of Tween 80 as a diluent for plasma significantly improved spike recovery in ESKD plasma (100.1% vs 70.4%, p<0.001).
Conclusions The kinetic LAL turbidimetric assay is a valid tool for the detection of blood endotoxin in patients with ESKD, although in blood specimens with low-level endotoxemia (≤0.05 EU/mL) the assay may be less accurate and precise. Tween 80 can be used as a diluent to optimise recovery of endotoxin in ESKD plasma.
- ENDOTOXIN
- RENAL
- NEPHROLOGY
Statistics from Altmetric.com
Introduction
Endotoxins (bacterial lipopolysaccharide) are proposed to be a major contributory factor to the chronic inflammatory state seen in patients with end-stage kidney disease (ESKD), and particularly in those on dialysis therapy.1 ,2 Chronic inflammation is associated with poor prognosis in dialysis patients3 and endotoxin-lowering strategies could potentially be useful in improving clinical outcomes in this population. However, blood endotoxin detection is difficult and no endotoxin detection assay has been validated for use in patients with ESKD. The optimum method of endotoxin detection needs to be determined in patients with ESKD to facilitate the development of endotoxin-lowering strategies in the future. Endotoxins can be detected using the Limulus amoebocyte lysate (LAL) assay.4 We aim to determine whether the LAL assay can be used for endotoxin detection in patients with ESKD. This will be the first study to determine the accuracy and precision of the LAL assay in advanced uraemia.
The principle of the LAL assay depends on the interaction of the lipid A component of bacterial endotoxins with proclotting enzymes present in the haemolymph of the horseshoe crab (Limulus polyphemus) activating a coagulation cascade and eventually gel formation culminating in a clot. The rate of increase in turbidity is measured using a spectrophotometer. This technique is known as the kinetic turbidimetric method, a variation of this technique involves the addition of chromogenic substrates to the LAL which undergo a colour change when the coagulation cascade is activated by the presence of endotoxin. It is not known whether turbidimetric or chromogenic method is superior for the detection of blood endotoxin, although the kinetic turbidimetric assay has the advantages of being more economical.5 The chromogenic assay may suffer from interference as plasma or serum samples can absorb light at the measured 405 nm wavelength, potentially interfering with assay results.6
The clinical interpretation of absolute blood endotoxin concentration is complicated by the variable levels of endotoxemia reported in the dialysis literature2 with some studies reporting extremely high7 or no detectable blood endotoxin in dialysis patients.8 ,9 The conflicting data reported in the literature may be due to different variations of the LAL method used, inadvertent contamination of blood samples during the blood collection process or an inherent inhibitory or activating effect of uraemic toxins on the LAL assay. Blood endotoxin detection is difficult due to the presence of poorly understood factors present in plasma that may activate or inhibit the LAL assay. Patients with ESKD are known to accumulate a variety of ‘uraemic toxins’ of different molecular sizes such as urea, leptin, guanidines, phenols and indoles. Larger molecular weight toxins and protein-bound molecules are not removed by dialysis therapy.10 It is not known whether the presence of these uraemic toxins affect the accuracy of the LAL assay. There are no published studies of the effect of uraemic toxins on the LAL assay.
Previous studies in patients with alcoholic liver disease have reported that binding of endotoxin to plasma proteins or its aggregation into large micelles11–14 may result in endotoxin being ‘hidden’ from detection.15 The use of the detergent, Tween 80, to dilute plasma samples improved recovery of blood endotoxins in patients with liver cirrhosis and gastrointestinal bleeding.16 The use of detergents may be helpful in detecting low-level endotoxins in samples with high protein content, such as plasma.
The purpose of this study is to determine the accuracy and precision of the kinetic turbidimetric LAL assay in patients with ESKD by comparison with healthy control samples. A secondary aim was to determine whether endotoxin spike recovery in patients with ESKD could be optimised by use of Tween 80 as a diluent.
Materials and methods
Overall study design
Plasma samples from non-inflamed patients with ESKD and healthy subjects were collected and spiked with different concentrations of standard endotoxin in the range reported in the dialysis literature.2 Accuracy of the turbidimetric LAL assay was assessed by comparison of measured endotoxin concentration in spiked samples with the expected concentration.
Precision of the technique was assessed by spiking plasma samples with known amounts of standard endotoxin at two concentrations across the expected range and repeated assays were carried on same samples to calculate a coefficient of variation (CV).
To determine the effect of Tween 80 on endotoxin recovery in plasma, ESKD and healthy control plasma samples were spiked with two concentrations of standard endotoxin across the expected range and spike recovery compared with and without Tween 80.
Patient recruitment
The study participants consisted of seven clinically stable patients undergoing outpatient haemodialysis at the Lister Renal unit and seven healthy controls recruited from volunteers and healthcare workers at the Lister Renal Unit, Stevenage, UK in June 2014. Ethical approval was granted by the local ethics committee and informed written consent was obtained from all study participants.
For inclusion in the study, all subjects were required to be clinically well at time of venesection with no evidence of infection or inflammation. There is no consensus in the literature that defines a ‘cut-off’ point of C reactive protein (CRP) to define inflammation.17 A CRP of 5 mg/L was defined as the upper reference interval in our hospital laboratory. Haemodialysis patients recruited were required to have two consecutive CRP concentrations <5 mg/L in the last 3 months.
Exclusion criteria were moderate anaemia (Hb<10 g/L), liver dysfunction, congestive cardiac failure and history of any gastrointestinal disease.
Venesection and processing of plasma samples
Blood was collected from study subjects using aseptic technique in sterile Terumo Venoject II heparinised tubes (Project KBF, Tokyo) and kept chilled on ice. In haemodialysis patients, blood was drawn predialysis through the arteriovenous fistula needle. Blood samples were centrifuged at 250g for 10 min at 4°C within 15 min of blood collection to obtain platelet-rich plasma. Plasma samples were divided into aliquots and stored in sterile, pyrogen-free Eppendorf Biopur Safe-Lock tubes and immediately frozen at −80°C.
All apparatus used for blood collection including syringes and blood collection tubes were checked for endotoxin contamination by random batch testing. Endotoxin contamination was checked using the standard method defined by the Association for Advancement of Medical Instrumentation by testing solutions that are allowed to dwell in medical devices for 1 h at 37°C for endotoxin.18 Endotoxin extracting solution (Wako Chemicals, USA) was used in replacement of pyrogen-free water as a rinsing solution because endotoxin recovery from devices using water may be less efficient.19 All apparatus tested had no detectable endotoxin (<0.005 EU/mL).
To ensure the absence of factors in blood storage and collection tubes that could interfere with endotoxin spike recovery, Terumo Venoject II heparinised tubes and Eppendorf Biopur Safe-Lock tubes were filled with LAL reagent water spiked with 0.5 EU/mL control standard endotoxin (Escherichia coli 055:B5) and allowed to dwell for 1 h at 37°C and then assayed for endotoxin. Spike recovery was consistently in the range 88%–172%. Samples are considered to be free of interfering factors if spike recovery is between 50% and 200%.20
Endotoxin assays: evaluation of Tween 80 on endotoxin spike recovery
Plasma samples from five healthy subjects and five subjects with ESKD were divided into aliquots and spiked with three different concentrations of control standard E coli 055:B55 endotoxin (0 (unspiked sample), 0.1 and 2.5 EU/mL). Samples were incubated at room temperature (20–25°C) for 15 min and diluted 1:10 with either 0.1% Tween 80 or LAL reagent water. The dilutions were heated to 70°C for 10 min, allowed to cool to room temperature and tested for endotoxin content in duplicate assays to assess spike recovery. Each batch of 0.1% Tween 80 was reconstituted using LAL reagent water (Charles River Laboratories, Ecully, France) and Tween 80 (Merck Chemicals, Darmstadt, Germany). Batches of 0.1% Tween 80 were consistently found to have no detectable endotoxin. There was no inhibition or enhancement effect of 0.1% Tween 80 on the LAL assay, spike recoveries ranged from 94% to 106%.
Differences in spike recovery between samples diluted in 0.1% Tween 80 and LAL reagent water were compared using paired t test. Endotoxin concentration between groups was compared using Wilcoxon signed-rank test or Mann–Whitney U test.
Endotoxin assays: assessment of accuracy
Plasma samples from healthy and ESKD subjects were divided into aliquots and spiked with five concentrations of control standard E coli 055: B5 endotoxin (0, 0.05, 0.1, 0.5 and 2.5 EU/mL). Plasma samples were incubated at room temperature for 15 min and diluted 1:10 with 0.1% Tween 80 and heated at 70°C for 10 min and allowed to cool to room temperature. Each spiked plasma sample was tested for endotoxin content in sextuplicate by the kinetic turbidimetric LAL assay (Endosafe KTA2 lysate; Charles River Laboratories, France) on sterile 96-well microplates (manufacturer certified to <0.001 EU/mL). Analysis of each microplate included duplicate wells containing LAL reagent water to act as a negative control. Plates were analysed using a Biotek ELx808 absorbance microplate reader with manufacturer supplied software (Endoscan-V V.4.0; Charles River Laboratories, France). A standard curve was constructed using the onset reaction times of standard dilutions of control standard endotoxin. A six-point standard curve was constructed for each microplate analysis (10–0.0025 EU/mL). All standard curves constructed had a correlation coefficient >0.98, as required for valid extrapolation of reaction times.20 Due to the 1:10 dilution factor, the lowest limit of detection in plasma samples was 0.025 EU/mL.
Bubble formation in plasma samples that introduced artefact in the optical density graphs was discarded from the study. Each spiked plasma sample had between four and six repeated measures for endotoxin content. A valid recovery was considered to be between 50% and 200%.20
Measured endotoxin spike recovery in plasma was compared with expected spike recovery using the Bland–Altman technique21 for ESKD and healthy controls. Difference in mean bias of spike recovery in ESKD and healthy plasma were compared using t tests for independent samples.
Endotoxin assays: assessment of precision
Plasma from two patients with ESKD and two healthy controls were pooled separately. Aliquots of pooled ESKD plasma and healthy plasma were spiked with two different concentrations of standard endotoxin (0.05 and 0.5 EU/mL) and subjected to 25 repeated measures for endotoxin content. CV was calculated for the onset reaction time. The onset reaction times for each individual assay was converted into endotoxin units per mL (EU/mL) using a linear regression equation derived from the standard curve. CV was also calculated for the measured endotoxin concentration (EU/mL) of each assay. There is no industry guidance on a minimum CV, although most manufacturers impose a CV of 10%–20% for results to be considered valid.22
Results
Effect of Tween 80 on endotoxin recovery in patients with ESKD and healthy controls
Ten patients were recruited for this study, comprising five patients with ESKD (mean age 58 years) and five healthy adults (mean age 44 years). Endotoxin recovery was similar in both ESKD and healthy subjects spiked with a low concentration of endotoxin (0.1 EU/mL). In plasma spiked with high concentration of endotoxin (2.5 EU/mL), the use of Tween 80 significantly improved recovery in both patients with ESKD (100.1% vs 70.4%; p<0.001; figure 1) and healthy controls (90.4% vs 59.8%; p=0.002; figure 2). In patients with ESKD, dilution of unspiked plasma samples with 0.1% Tween 80 yielded a higher concentration of endotoxin content than in plasma samples diluted with water only (0.04 vs 0.036 EU/mL; p=0.046; figure 3). Endotoxemia was detected in four of five patients with ESKD and the median endotoxin level was 0.041 EU/mL (95% CI 0 to 0.1 EU/mL). In healthy controls, low-level endotoxemia was detected in only one subject (0.027 EU/mL).
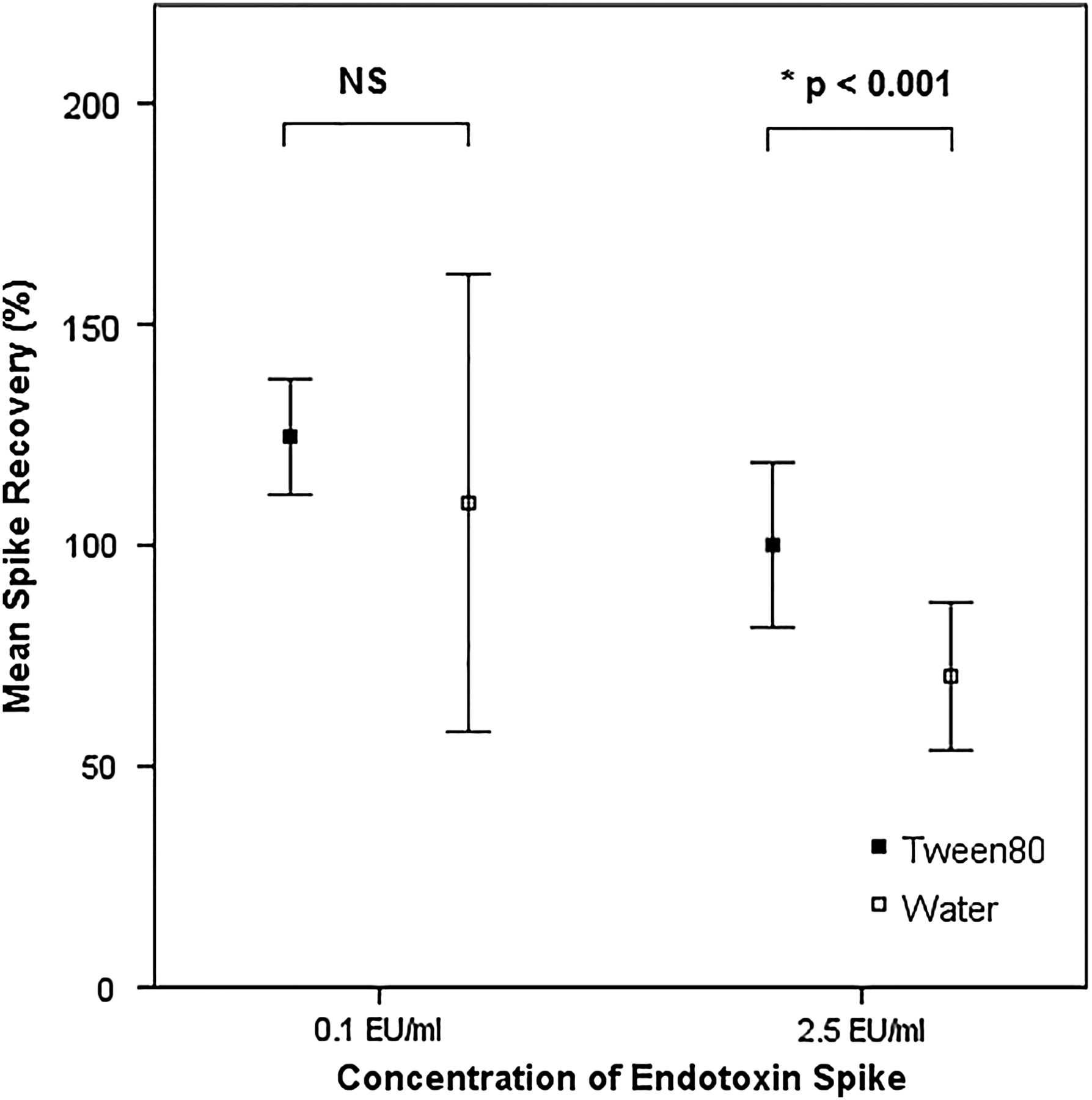
Mean endotoxin spike recovery in end-stage kidney disease plasma diluted with 0.1% Tween 80 and water.

Mean endotoxin spike recovery in healthy plasma diluted with 0.1% Tween 80 and water.

Baseline endotoxin content in plasma of subjects with end-stage kidney disease diluted with 0.1% Tween 80 and water.
Although valid spike recoveries of between 50% and 200% was obtained using both Tween 80 and water, recovery was significantly less in samples with high endotoxin content that were diluted in water. Baseline endotoxin content was also significantly higher in ESKD plasma diluted with 0.1% Tween 80. Due to this finding, 0.1% Tween 80 was used as a diluent for plasma samples for subsequent spike recovery experiments.
Endotoxin spike recovery in patients with ESKD and healthy controls
Overall mean endotoxin spike recovery was 111.6% and 125.2% in patients with ESKD and healthy subjects, respectively. There was no statistical difference in spike recovery between ESKD and healthy plasma. Recovery was within the recommended 50%–200% limit for all four different levels of endotoxin spike (table 1).
Mean spike recovery in patients with ESKD and healthy controls
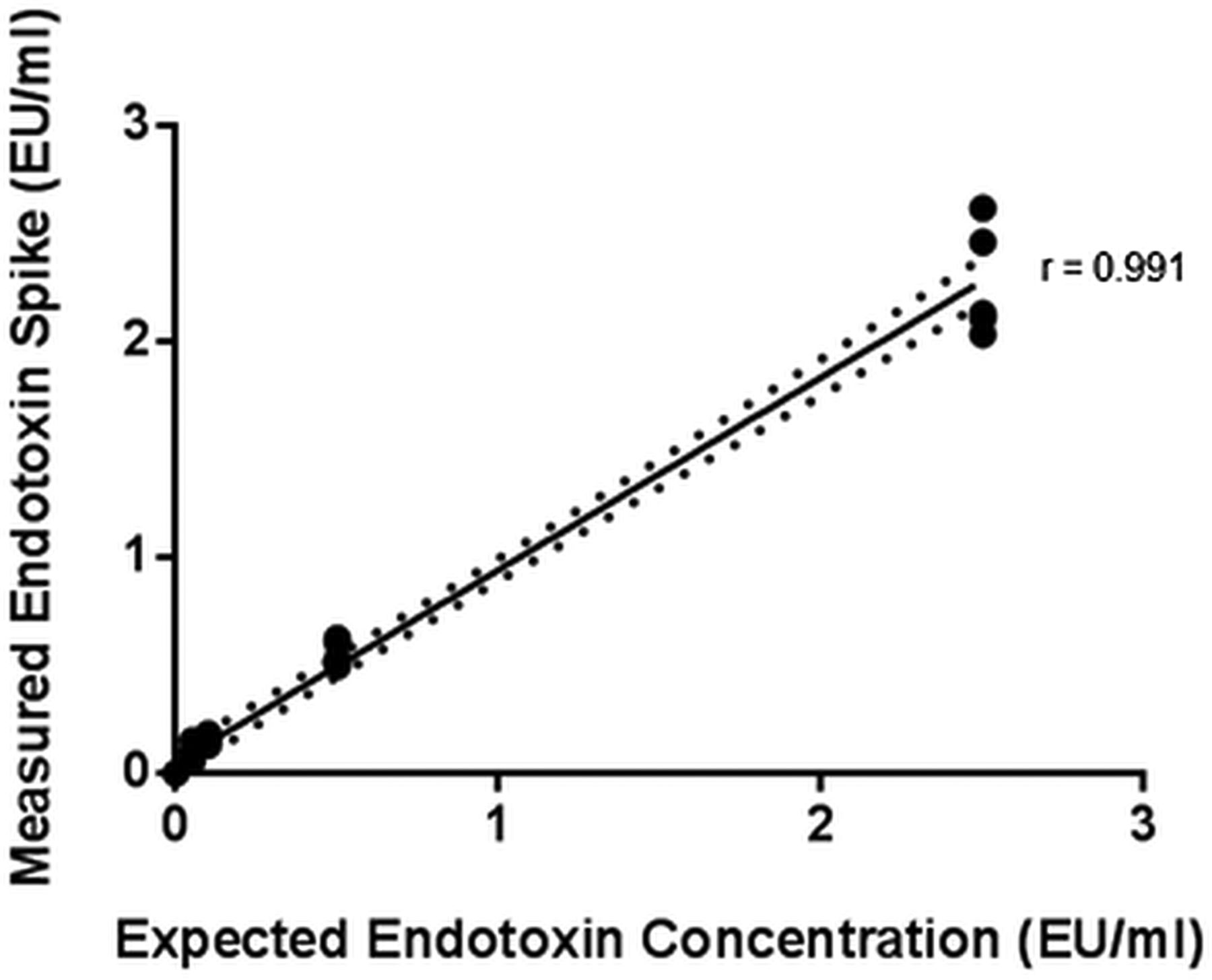
Mean observed endotoxin levels in spiked samples correlated well with the expected endotoxin concentration. Correlation coefficient was 0.98 and 0.99 for patients with ESKD and healthy subjects, respectively (figures 4 and 5).

Measured versus expected endotoxin concentration in healthy subjects. Each data point represents a mean of four to six assays for an individual subject.

Measured versus expected endotoxin concentration in subjects with end-stage kidney disease. Each data point represents a mean of four to six assays for an individual subject.
Bland–Altman plots comparing observed and expected endotoxin concentration in patients with ESKD and healthy controls are shown in figure 6. In subjects with ESKD, mean bias of the kinetic turbidimetric LAL assay was 0.039 EU/mL (95% CI −0.05 to 0.128) with limits of agreement from −0.385 to 4.633. In healthy subjects, mean bias was −0.017 EU/mL (95% CI −0.077 to 0.044), with limits of agreement from −0.392 to 0.287 (figure 6). There was no significant differences in mean bias between patients with ESKD and healthy subjects (p=0.302).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bland–Altman analysis of measured endotoxin levels compared with the expected value in patients with end-stage kidney disease (ESKD) and healthy subjects.
Precision of the kinetic turbidimetric LAL assay in uraemic and non-uraemic plasma
CV calculated from the onset reaction time was ≤5% for both patients with ESKD and healthy subjects. CV calculated from the observed endotoxin concentration was higher than that calculated from onset reaction time, but ≤10% except for ESKD plasma that was spiked with low level of endotoxin (0.05 EU/mL; CV 24.1%; table 2).
CV from 25 repeated measures of pooled ESKD and healthy plasma spiked with two different concentrations of endotoxin
Discussion
This is the first published study looking at the accuracy and precision of the LAL assay in the setting of ESKD. Our study indicates that the presence of uraemic toxins do not significantly inhibit or enhance the activity of the LAL assay. With appropriate plasma pretreatment conditions, the kinetic turbidimetric LAL assay is able to accurately recover endotoxin across a wide range of endotoxin concentration (0.05–2.5 EU/mL). Variability in LAL testing is a well-recognised phenomenon due to differences in assay sensitivity, manufacturer reagents and the different methods of the LAL testing available such as the gel-clot, end-point and kinetic techniques. Variability may also be introduced due to differences in collection tubes, glassware, microplates and sample pretreatment procedures.23 ,24 Due to this variation, industry guidance allows a twofold error and spike recovery of 50%–200% in endotoxin testing.20 ,25 Spike recovery in ESKD and healthy plasma in our study was comparable well within the recommended 50%–200% limit. Correlation of measured endotoxin spike with the expected concentration was high (r>0.97); however, there is a potential bias of ±0.039 EU/mL using the LAL turbidimetric assay in ESKD plasma which can be significant when interpreting endotoxin concentration in blood specimens with low-level endotoxemia.
The precision of the kinetic turbidimetric LAL assay was high in both ESKD and healthy plasma. Precision based on CV calculated from onset reaction times was ≤5% in uraemic and non-uraemic groups. CV calculated using the observed endotoxin concentration was higher and in ESKD plasma spiked with a low-concentration endotoxin, the CV was 24.1%, but improved to 8.9% with a high-concentration endotoxin spike. The calculation of CV is a contentious issue in LAL endotoxin testing due to the lack of industry guidance.22 Depending on the manufacturer, the CV may be calculated from the onset reaction time or the mean endotoxin concentration of samples (EU/mL). It has been suggested that using the mean endotoxin concentration for statistical analysis may be a more robust measure of assay precision.22 Our study results suggest that the kinetic LAL turbidimetric assay is a valid assay for detection of endotoxemia in patients with ESKD, but with the caveat that at low levels of endotoxemia (≤0.05 EU/mL) it is both less precise and accurate.
To our knowledge, this is the first report on the use of detergent to successfully optimise endotoxin recovery in plasma from patients with ESKD. Endotoxin molecules are known to form aggregates and micelles due to their amphipathic nature,26 which may prevent their detection. In high protein solutions, detergents such as Tween 80 are able to release lipopolysaccharide monomers from aggregates,27 which may explain our observations. The use of detergent as a diluent for plasma samples may be a useful adjunct for accurately assessing blood endotoxin particularly in patients with high-level endotoxemia. However, this may not be applicable universally since our study included only non-infected, non-inflamed, clinically well patients. The effect of detergent on spike recovery in low protein content plasma samples, seen in septic, malnourished or hypoalbuminaemic patients will need further investigation.
In our study, we verified the quality of phlebotomy and blood/plasma storage apparatus to exclude the possibility of endotoxin contamination and interfering factors. Blood sampling, processing and plasma pretreatment to remove interfering factors were performed rapidly to avoid any potential endotoxin inactivation in untreated plasma.28 These preanalytical factors have not been reported as meticulously in previous manuscripts.7 ,29–34 We selected patients with ESKD who were clinically well and blood was taken from arteriovenous fistulas predialysis, avoiding the possibility of sample contamination from bacterial biofilms that may be present in venous catheters and dialysis circuits. In conventional kinetic methods, testing samples for inhibition or enhancement is performed by measuring recovery of pretreated sample (ie, diluted and heated samples) spiked with endotoxin with a concentration that falls near the mid-point of standard calibration curves. However, endotoxins can be lost during the dilution or heating procedure and recovery may not be universal at different concentrations of endotoxin. Consequently, we chose to spike whole plasma before heat-dilution treatment and with different levels of spike, which we argue is a more robust measure of spike recovery.
The limitations of this study are the relatively small number of study participants and the use of control standard endotoxin to assess spike recovery. Although spike recovery was good in uraemic plasma, control standard endotoxin are usually stabilised in preservatives such as lactose and polyethylene glycol26 and behave differently to naturally occurring endotoxin. However, native endotoxins are difficult to standardise and many other published studies also use control standard endotoxin to assess recovery.16 ,28 ,35–37 Baseline interference of the LAL assay in untreated healthy and ESKD plasma was not studied and optimal plasma pretreatment methods were not explored in this study. Plasma pretreatment methods have been reviewed extensively by Hurley et al.28 A tenfold dilution and heating plasma samples at 70°C for 10 min was recommended to remove interfering factors, but different heating temperatures and dilution factor may result in better spike recoveries in ESKD plasma.
The LAL assay is currently not licensed by the Food and Drug Administration for ‘detecting endotoxemia in man’ and blood endotoxin detection is restricted to research use only. This decision was heavily influenced by several studies which concluded that the clinical use of the LAL assay to detect endotoxin in septic patients with bacteraemia was poor.38–40 Although it has been argued that the use of the positive blood culture for Gram-negative bacteria as a ‘gold’ standard may not be appropriate given the low sensitivity of blood cultures in identifying patients with sepsis.40 ,41 In addition, bacteraemia and endotoxemia are not necessarily related events,40 and these early clinical studies employed the use of insensitive gel-clot LAL assays and technically difficult chloroform extraction procedures to remove plasma inhibitors.39 ,40
In summary, endotoxemia may be a clinically significant problem in patients with ESKD29 ,30 ,42 contributing to chronic inflammation but its measurement is with LAL assays has limitations that need to be recognised. Our study suggests that with appropriate preanalytical handling and treatment of plasma samples, the kinetic turbidimetric LAL assay is a valid tool for the detection of endotoxemia in advanced uraemia though the accuracy and precision is more limited below 0.05 EU/mL. Development of quantitative assays for plasma measurement would facilitate the development of endotoxin-lowering strategies in the future which may lead to patient benefit.
Take home messages
-
The kinetic turbidimetric Limulus amoebocyte lysate (LAL) assay can be used to detect plasma endotoxin in patients with end-stage kidney disease.
-
Detergents such as Tween 80 may optimise endotoxin recovery from plasma samples with high endotoxin content in patients with end-stage kidney disease.
-
In plasma specimens with low-level endotoxemia (≤0.05 EU/mL), the LAL assay may be less accurate and precise.
Acknowledgments
The authors would like to thank the patients who participated in this project. They also thank Matthew Reynolds, Senior Specialist in Endotoxin and Microbial Detection at Charles River for technical advice with the project.
References
Footnotes
-
Contributors JW conducted all endotoxin assays and wrote the manuscript. HJ, AV, EV and KF reviewed and edited the final manuscript and provided technical and statistical advice to the manuscript.
-
Funding This project was funded from the Lister Renal Research Fund. JW has received a travel grant from the Great Britain Sasakawa Foundation.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval NHS Health Research Authority—NRES Committee South Central—Berkshire B.
-
Provenance and peer review Not commissioned; externally peer reviewed.