Article Text

Abstract
Aim Traditional serrated adenoma (TSA) is an uncommon type of serrated adenoma that can be a precursor to biologically aggressive colorectal cancer that invokes the serrated (accelerated) pathway. The purpose of this review is to address some of the more contentious issues around nomenclature, diagnostic criteria, histological variants, coexistence with other polyp types, the occurrence of dysplasia and the differential diagnosis.
Results While the vast majority of TSAs are exophytic villiform polyps composed of deeply eosinophilic cells, flat top luminal serrations and numerous ectopic crypt foci, histological variants include flat TSA, filiform TSA and one composed of large numbers of mucin-containing cells. It is unlikely that there is any biological difference between the histological variants. There is a contention that TSAs are not dysplastic ab initio and that the majority do not show cytological atypia. Two types of dysplasia are associated with TSA. Serrated dysplasia is less well recognised and less commonly encountered than adenomatous dysplasia. TSA with dysplasia must be separated from TSA with coexisting conventional adenoma.
Conclusions TSA is a characteristic polyp that may be extremely exophytic, flat or composed of mucin-rich cells and is typified by numerous ectopic crypt foci. They may coexist with other serrated polyps and conventional adenomas. Approximately 20–25% will be accompanied by adenomatous dysplasia.
- GASTROINTESTINAL DISEASE
- COLON
- NEOPLASMS
Statistics from Altmetric.com
Traditional serrated adenomas (TSAs) are the least common of the three serrated colonic polyps: occurring in frequency after hyperplastic polyps (HPs) and sessile serrated adenomas/polyps (SSA/Ps) and accounting for only about 5% of serrated polyps. However, the current estimate is likely to increase with the widespread implementation of bowel cancer screening programmes, better endoscopy and increasing awareness of TSA among diagnostic pathologists. It is therefore reasonable to anticipate that TSA will be encountered more frequently.
In the last few years several studies have been performed on TSA highlighting morphological features and molecular aspects that have shed valuable insight into the pathogenesis and diagnostic features of these polyps. Despite this, there remains a degree of uncertainty around some of the morphological aspects and features of TSA. With this in mind, the purpose of this overview is to discuss some of the more controversial and slightly nebulous issues surrounding TSA.
Is traditional serrated adenoma a good term?
This term is based on the original description by Longacre and Fenoglio-Preiser1 who described in essence, a conventional adenoma with a serrated luminal profile. The key features that overlapped with and resembled conventional adenoma were elongated, penicillate slightly hyperchromatic nuclei. The ‘traditional’ appellation was introduced to separate these polyps from and avoid confusion with SSA/P while still alluding to the original entity of ‘serrated adenoma’. Most polyps are designated on the basis of their gross appearance and/or histological or morphological features. Hence, polyps in general are sessile or pedunculated; tubular, tubulovillous or villous in architecture. In contrast to SSA/Ps (sessile) and HPs (semi-sessile), TSAs are protuberant, exophytic, villous and serrated. Perhaps exophytic eosinophilic serrated polyp/adenoma would be more descriptive and account for the vast majority of TSAs, rare morphological variants that are not exophytic or eosinophilic may be encountered (see later). While the term ‘traditional serrated adenoma’ only describes one of the morphological features of a TSA (luminal serration), the term is now somewhat entrenched in the literature, most pathologists are aware of the term and as such, should remain.
What are the diagnostic criteria?
As with most polyps there are architectural and cytological considerations that form a constellation of features that typify TSA. As mentioned above, the vast majority of TSAs are exophytic, tubulovillous or villous polypoid lesions (variants are discussed later) and this is the key, low-power architectural impression. In concert with this growth pattern, there is a constellation of characteristic cytological/histological features: striking granular eosinophilic cytoplasm, luminal serrations, presence of ectopic crypt foci (ECF) and elongated, penicillate nuclei with evenly dispersed coarse chromatin and small inconspicuous nucleoli (one to two). In about half the cases, smooth nuclear membranes and contours and occasionally, longitudinal nuclear grooves may be discerned.
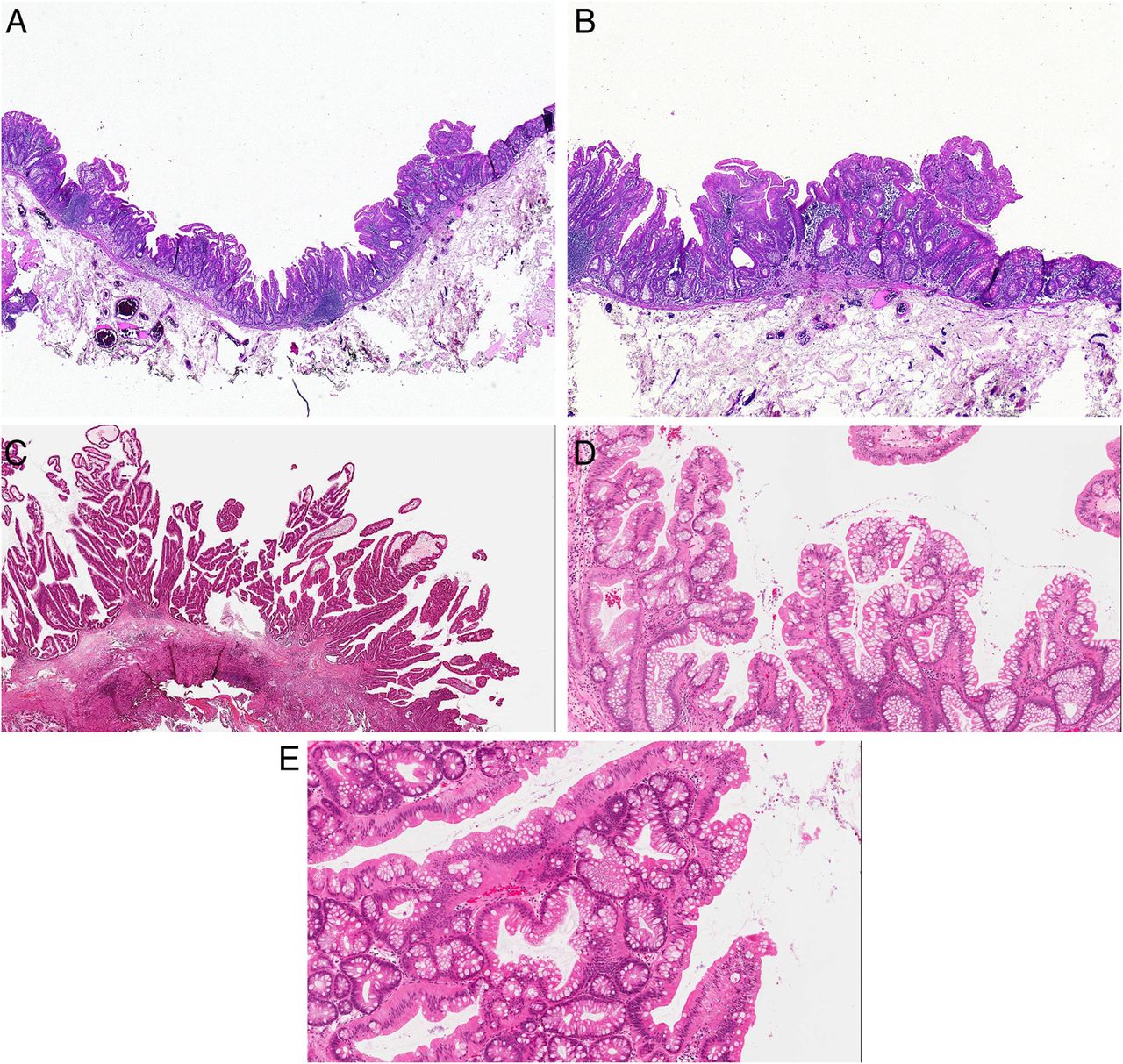
Cytoplasmic eosinophilia is a consistent feature and can be appreciated even at low power (figure 1A). There is often an abrupt transition between cells with eosinophilic cytoplasm and the non-polyp mucosa. In many cases, the luminal aspect of the eosinophilic cells displays a brush border.

(A) Intense cytoplasmic granular eosinophilia typifies the vast majority of the constituent cells of a traditional serrated adenoma (TSA) and this together with the villiform architecture is the immediate low power clue to the diagnosis. (B) The luminal serrations in a TSA have a flat top (arrows) rather than saw-toothed or more pointed as in hyperplastic or sessile serrated polyps. There are deep invaginations that impart this appearance that is reminiscent of the sides of small intestinal villi. (C) Ectopic crypt foci (arrows) are the hallmark lesion of TSA. These enigmatic foci appear as eddies or swirls at the base of the lining epithelium and are not anchored to the underlying muscularis mucosae. Although seen in tubulovillous adenomas occasionally, they are most frequent in TSA.
The luminal serrations encountered in TSA are unique among other serrated polyps (figure 1B). It is described as deep clefts, indentations and slit-like spaces, leading to broad luminal fronds that protrude into the gland lumen or from surface of a papillary frond often in a broad flat-topped, mushroom-like or jigsaw puzzle-like appearance. Depending on the plane of section, some of the projections may be more pointed rather than flat topped. This appearance together with the presence of cytoplasmic eosinophilia and an apical brush border is very reminiscent of small bowel mucosa and in particular, the sides of villi.
ECF are enigmatic lesions that are present in the mucosa lining the papillary structures, form whorled clusters, ball-like aggregates or swirling buds that are present at the basement membrane of the mucosa (even in glandular invaginations of the mucosa) and are not anchored to or reaching the muscularis mucosae (in other words, they are ‘abortive’ or ‘incomplete’ crypts) (figure 1C). Sometimes ECF may occur at the base or crevice of the surface serration. It should be borne in mind that some of the smaller TSAs and the flat variant (see below), may not show well developed or any ECF. ECF have been touted as the diagnostic tocsin or hallmark of TSA, but it is now known that ECFs do not occur in all TSAs (with as little as 62% of TSAs noted to contain ECF in one study; while others have documented incidence rates of 79.4%, Bettington et al observed ECF in 94% of TSAs larger than 10 mm and 78% of those smaller than 10 mm).2–4 ECF are also seen in conventional tubulovillous adenomas and this has been documented to occur in 34% of tubulovillous adenomas in a recent study.5 To the best of my knowledge, ECF have not been described in pure, bona fide SSA/P or HP. Thus ECF, although not exclusively seen in TSA, are far more numerous and most frequently encountered in TSA compared with tubulovillous adenomas.
Of the three key histological features: cytoplasmic eosinophilia, characteristic serration and ECF, it appears that only the characteristic serration pattern is unique to TSA and not seen in other types of polyps. As such, this would therefore be the most reproducible and recurring feature of typical TSAs and histological variants. Thus, if minimum criteria need to be established then the characteristic pattern of serration could be regarded as the most distinctive/recurring feature of TSA. However, it is extremely rare to encounter a TSA without at least two of the three above-mentioned histological criteria being present. It is prudent to say that no single histological feature makes the diagnosis and it is usually an assessment of the constellation of microscopic features that formulate the final diagnosis of TSA.
What are the morphological variants?
Three variants are recognised: flat, filiform and mucin-rich.
Flat TSA
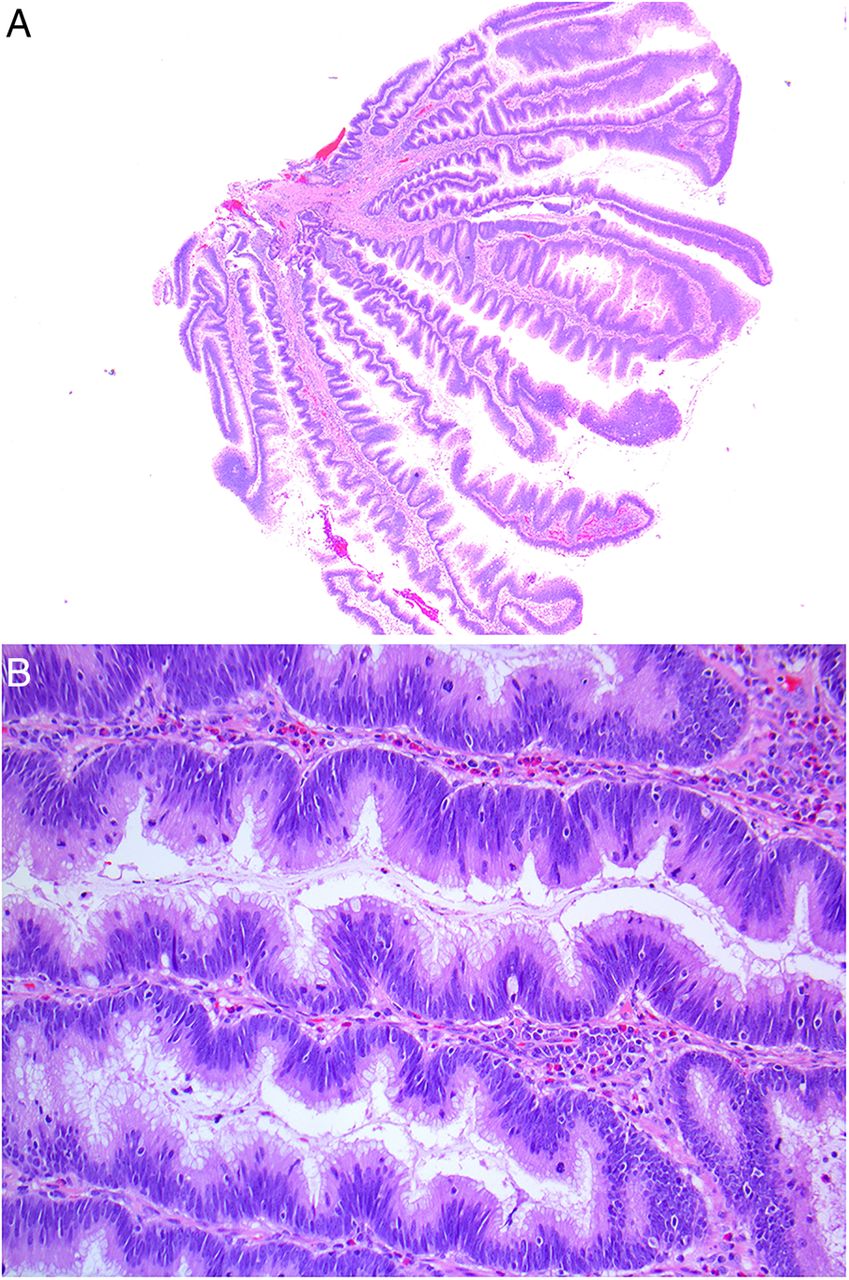
The description of the flat variant of TSA is ascribed to Bettington et al4 who suggested that the height of a flat TSA should not be more than twice the height of adjacent normal mucosa, and that there is an absence of prominent villiform projections (figure 2A, B). Using these criteria, in their analysis of 200 TSAs, Bettington et al4 found that 38% of cases fulfilled the criteria for categorisation as a flat TSA. In terms of total numbers, flat TSAs were encountered equally between right and left sides of the colon; however overall, flat TSAs accounted for the majority of all right-sided TSAs in their series (37 of 59 right-sided TSAs were the flat variant). They also observed that flat TSAs arose within or were admixed with SSA/P. Approximately 25% of flat TSAs in the series reported by Bettington et al,4 did not contain ECF. Additionally, flat TSAs harboured more BRAF than KRAS mutations. These authors concluded that the flat versus protuberant morphology was location dependent rather than being due to any intrinsic feature of TSA.4 Other than the flat morphology/growth pattern, the cytological features are similar to classic TSA.

(A and B) Flat traditional serrated adenoma (TSA) should not project more than twice the height of adjacent normal mucosa (Figures provided courtesy of Dr Mark Bettington).
Filiform TSA
This unusual variant was first described in 2007 by Yantiss et al6 as a discrete variant of TSA, ‘filiform serrated adenoma’. This filiform variant of TSA is composed of longer villous processes that the usual TSA or conventional tubulovillous adenoma. The villous processes are characterised by stromal oedema that results in the tips of the processes having a bulbous or drumstick appearance (figure 2C). The lining cells were columnar, contained eosinophilic cytoplasm with an admixture of goblet cells and the serrated pattern of typical TSA was also present. However, they tended to be larger than typical TSA. In addition, some of these polyps were admixed with HP and SSAs. It is interesting to note that there is no mention of ECF in the pathological description of these polyps in the initial paper by Yantiss et al.6 In a more recent description of filiform serrated adenoma by Ha et al, again no mention is made of ECF but from the illustrations, it appears as if ECFs are indeed present. The filiform variant is molecularly similar to the usual type of TSA, although Ha et al7 observed that cases in their series showed less frequent methylation of HLH1.
Typical TSA is an exophytic, villiform lesion and the filiform variant displays an exaggerated villiform pattern with bulbous tips of the processes, and this appears to be the only point of separation. It is extremely unlikely that there is any biological difference in behaviour between this variant and the more typical TSA, even though Ha et al7 postulated that the filiform variant is less aggressive.
Mucin-rich or goblet cell-rich cells
While the archetypical TSA is characterised by most, if not all, constituent cells displaying intense cytoplasmic eosinophilia, the mucin-rich variant merely contains several goblet cells or mucin-rich/goblet cell- rich columnar cells (accounting for at least 50% of the constituent cells) interspersed with fewer eosinophilic cells (figure 2D, E). Architecturally and even biologically (at this point), this variant is no different from the usual TSA and perhaps is just a histological nuance. However, an unpublished observation is that fewer ECF seem to be apparent in TSAs with a large population of mucin-rich or goblet-cell rich cells.
Are all TSAs dysplastic?
Dysplasia and the type of dysplasia are probably the most controversial aspects of TSA. For historical reasons, based on the seminal description by Longacre and Fenoglio-Preiser,1 serrated adenomas or TSA were regarded as being inherently dysplastic (showing conventional adenomatous dysplasia) on the basis of the nuclear resemblance to those encountered in tubular or tubulovillous adenomas. However, this paradigm was questioned by Bettington et al4 in their detailed analysis of 200 TSAs. They advanced three reasons why the standard TSA cytology did NOT represent a dysplastic state ab initio: (1) the usual TSA cytology was not overtly atypical (2) mitoses were infrequent/absent and there is a low Ki-67 proliferation index, and (3) ancillary immunohistochemical stains for β-catenin and p53 were negative while p16 was retained.4 If this is accepted, and personal observation would tend to concur that a large proportion (the majority) of TSAs are devoid of cytological atypia in the form of mitoses, hyperchromatic crowded nuclei displaying pleomorphism, loss of polarity, pseudostratification reaching the luminal aspects of the lining cells, or the architectural features of dysplasia: crowding of glands, back to backing arrangement or cribriform patterns.
At this juncture, it is worth pointing out that two forms of dysplasia have been associated with serrated polyps in general. The first and better recognised is adenomatous dysplasia that attends conventional tubular and tubulovillous adenomas. This form of dysplasia is recognised by the cytological and architectural features outlined above and are graded into low-grade and high-grade. This is ingrained and entrenched in routine diagnostic practice and as such is readily recognisable. There are four major studies of TSAs wherein adenomatous dysplasia was assessed. The study conducted by Kim et al3 noted conventional dysplasia in 23 of 107 TSAs (21.5%) and Bettington et al4 encountered 38 of 200 ‘advanced’ TSAs (19%). This latter category included cases of overt dysplasia and/or carcinoma within a TSA. In the series reported by Tsai et al,8 25 of 60 TSAs were dysplastic (42%) while Wiland et al2 noted dysplasia in 16 of 55 cases (29%), 14 of these 16 cases displaying low-grade dysplasia.
The assessment of adenomatous dysplasia within TSA can be hampered by the presence of mixed TSA and conventional adenomatous polyps but if these mixtures are excluded, approximately 20–30% of pure TSA should contain areas of adenomatous dysplasia, usually low-grade (figure 3A, B).

(A and B) Low-grade adenomatous dysplasia within a traditional serrated adenoma (TSA) has the same appearance as the dysplasia accompanying a conventional tubular or tubulovillous adenoma; elongated, penicillate with nuclear hyperchromasia, stratification and mitoses.
The second, perhaps more controversial and less well recognised form of dysplasia associated with serrated polyps including TSA, is so-called serrated dysplasia.
What is serrated dysplasia?
This form of dysplasia has not received much attention even though Lazarus et al9 and then subsequently Goldstein,10 described the cytological features over a decade ago. A proportion of serrated polyps (SSA/P, HP and TSA) are united by serrated dysplasia and the serrated molecular pathway. There is increasing acceptance of a molecular transition from the microvesicular HP through to SSA/P to TSA to serrated adenocarcinoma, this continuum being underpinned by the serrated molecular pathway. The cytological features described by Lazarus et al9 for serrated dysplasia potentially can be seen in all three forms of serrated polyps depending on the dominant mutation in that particular polyp. BRAF mutations are felt to initiate the serrated pathway and hence, serrated dysplasia. Serrated dysplasia was graded as mild, moderate and severe on the basis of cytological and architectural criteria.9 The cytological features were gauged along the length of the crypt starting from the base, ascending to the mid-crypt and then to the surface. Nuclear features of serrated dysplasia suggested by Lazarus et al included: enlargement, variation in size and shape, stratification and loss of polarity. Goldstein10 refined these criteria, collapsing mild and moderate dysplasia into low-grade serrated dysplasia and added the following features: lining cells were cuboidal to short columnar, the nuclei were round to oval, chromatin pattern was vesicular and open, a prominent large macronucleoli and decreased amounts of eosinophilic cytoplasm (figure 4A). As regards mitotic activity, this was noted in the mid and upper crypt as opposed to being restricted to the normal proliferative compartment in the crypt base (figure 4B). These cytological features when fully fledged and prominent would qualify for high-grade serrated dysplasia, and are accompanied by architectural complexity.

(A and B) Low-grade serrated dysplasia, on the other hand, is characterised by ovoid enlarged nuclei, vesicular dispersed chromatin and occasional mitoses. (C) As part of the serrated dysplastic process is a dysmaturation phenomenon with uneven distribution of goblet cells within crypts and the presence of so-called ‘inverted’ goblet cells (arrow). (D) So-called ‘floating’ goblet cells are seen irregularly distributed within the lining and not luminally oriented as in normal mature mucosa (arrows).
The architectural changes increase with evolution and progression of the serrated pathway: luminal serration, budding, branching, crowding and fusion of glands, surface villosity (the extreme example of this being the exophytic appearance of TSA). The architectural complexity increases from a simple HP to a SSA/P (which is defined by its architectural features primarily), and eventually in a TSA.
While the term ‘dysplasia’ was appended to this constellation of changes, there is a clear association with a ‘dysmaturation’ or, abnormal proliferation and maturation process.11 The dysmaturation process is evidenced by the presence of ‘immature’ or dystrophic goblet cells, seen especially in HP and SSA/P. These cells have cytoplasmic vacuoles of mucin and large, round nuclei often with a nucleolus oriented towards the luminal aspect of the cell. In other words, these dystrophic goblet cells have an inverted pattern: instead of apical mucin vacuoles and basal nuclei, they are characterised by basal mucin and apically (luminally) oriented nuclei (figure 4C). Furthermore, these dystrophic goblet cells (and mature goblet cells) are distributed irregularly and asymmetrically along the crypt, reflecting the dysmaturation process that is inherent in serrated dysplasia (figure 4D).
Specific to TSA, a smaller proportion display serrated dysplasia compared with adenomatous dysplasia (exact incidences are not known). TSAs exhibiting serrated dysplasia harbour BRAF mutations and result in serrated adenocarcinoma via the accelerated serrated molecular pathway, while those with adenomatous dysplasia have KRAS mutations and in all likelihood are not associated with precursor or antecedent HPs or SSPs.
The biological significance of low-grade serrated dysplasia is not well understood and with this in mind, several have advocated that this feature not be reported. High-grade serrated dysplasia is recognisable histologically because of the extreme cytological and architectural atypia and as such should be documented. If one believes that high-grade serrated dysplasia is a manifestation of the serrated pathway which causes polyps to pursue an aggressive accelerated course to cancer, then it makes sense that these polyps are flagged and the patients be treated and/or managed differently. Thus, for practical purposes, high-grade serrated dysplasia should be recognised and reported as a form of high-grade dysplasia, and at this juncture it does not warrant being reported specifically as serrated high-grade dysplasia; simply high-grade dysplasia not otherwise specified will suffice.
With regards to low-grade serrated dysplasia, this too should not be reported routinely (this is in keeping with adenomatous polyp reporting guidelines wherein the presence of low-grade dysplasia is commented on; rather a comment of ‘negative for high-grade dysplasia’ is the usual accompaniment). Making a diagnosis of SSP implies the de facto presence of low-grade serrated dysplasia.
Since conventional adenomatous dysplasia is more common than serrated dysplasia in SSA/P and TSA, this form of dysplasia (low or high), if present, should be commented on in pathology reports. If not present, then the appropriate comment is ‘negative for dysplasia’. It is assumed, currently, that any dysplasia encountered in serrated polyps is adenomatous rather than serrated.
What is the differential diagnosis and can TSA coexist with other polyps?
When fully developed and displaying all three defining cytological features together with the usual exophytic growth pattern, there is no real diagnostic dilemma. This applies to the vast majority TSAs when the aforementioned features are predominant. Diagnostic difficulty and a degree of confusion arise when TSA is admixed with HP, SSA/P or tubulovillous adenomas. HP and SSA/P are regarded as precursor lesions and have been noted to coexist within and immediately adjacent to TSA. In a detailed analysis of 149 TSAs (the dominant histological features in the polyps were of a TSA), 78 (52.34%) showed histological evidence of another polyp. The most common coexistent polyp was low-grade tubular/tubulovillous adenomas (32 cases), followed by 28 HPs and 18 were SSA/Ps.12 An important observation from this study was that the tubular/tubulovillous adenomas were always found adjacent to the TSA while the HPs and SSAs were intimately admixed with the TSA. This occurrence lends credence to the common molecular heritage of serrated polyps. Others have also examined the presence of other serrated polyps or ‘precursor’ lesions occurring with TSA. Wiland et al2 noted that 24% of TSAs in their series were accompanied by another serrated polyp, usually an HP. Kim et al3 found SSA/P to be more commonly associated with TSA (31% of TSAs had another serrated polyp). In a more recent study in 2013, Kim et al13 describe 52% of their TSAs with HP (the majority) and SSA/P. Bettington et al4 noted that 38% of the 200 TSAs in their series were accompanied by HP/SSA/P, with the vast majority being SSA/P. Finally, in an earlier study by Torlakovic et al11 in 2008, 6 of 18 (30%) TSAs were accompanied by HP. Hence, the occurrence of HP, SSA/P and conventional adenomas are not uncommonly admixed with or adjacent to TSA, ranging in frequency from 24% to 52% of cases.
While some have referred to these ‘hybrid’ serrated polyps as mixed, it is probably best to refrain from using the term mixed as this has been used previously to describe adenomatous polyps occurring with HP. In the context of coexistent serrated polyps, it appears logical to name the polyp after the most dominant histological type of polyp present. In other words, reports should be phrased: ‘TSA with admixed HP’, or ‘TSA with SSP’ and an accompanying comment on the presence or absence of dysplasia. Whatever way the nomenclature is used it should certainly convey what the dominant polyp is whether there is accompanying dysplasia or not.
It should also be borne in mind that minor, microscopic foci of TSA histology (all three key features together) can be discerned frequently within other serrated polyps and tubular/tubulovillous adenomas. In addition, cells with deeply eosinophilic cytoplasm can be encountered in bona fide HP, SSA/P and conventional adenomas, while ECF may be seen in conventional adenomas. Again, for practical purposes, both these scenarios should be ignored in the final pathology report.
Recently, Bettington et al14 have described a so-called serrated tubulovillous adenoma. This polyp resembles a conventional tubulovillous adenoma cytologically in terms of dysplasia but is typified by projections that are probably best described as ‘undulating’ or festooned rather than the usual serrated pattern seen in TSA, HP or SSA/P (figure 5A, B). The undulations imparted a maze-like appearance to the polyps and by definition occupied at least 50% of the architecture.14 In addition, these polyps displayed ECF, again reflecting that ECF are not the sole preserve of TSA. Despite the similarity in name, the exophytic architecture and the presence of ECF, serrated tubulovillous adenomas did not show deeply eosinophilic or the very typical serrated pattern that characterise a prototype TSA. Bettington et al14 contend that serrated tubulovillous adenomas are a distinct variant of conventional tubulovillous adenoma characterised by and differing from their conventional counterparts by: the unique pattern of serration occupying more than 50% of the polyp, more proximal location, larger size, having more CpG island methylation and more frequent KRAS mutations. One of the objectives of the study by Bettington et al14 was to prevent misdiagnosis of these polyps as TSA. While concurring that there are sufficient features to discriminate serrated tubulovillous adenoma from conventional tubulovillous adenoma and TSA, the appellation ‘serrated’ is perhaps unfortunate and may create confusion. Other possible descriptive terms such as ‘sinuous’, ‘festooned’ or ‘serpentine’ may better describe the pattern of serration in so-called serrated tubulovillous adenoma, thus avoiding confusion with true serrated polyps (especially the histological scenario when TSA coexists with conventional tubulovillous adenoma) that are underpinned for the most part by the serrated molecular pathway.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A and B) Serrated or undulating tubulovillous adenoma is a potential lookalike of traditional serrated adenoma (TSA). However, these are really tubulovillous adenomas with a luminal pattern of undulations rather than the characteristic serration pattern of a TSA.
Take home messages
Traditional serrated adenoma (TSA) represents a unique polyp that falls within the spectrum of serrated polyps.
It has a very characteristic constellation of morphological features with an exophytic growth pattern, cytoplasmic eosinophilia and ectopic crypt foci being characteristic.
Morphological variants are flat, filiform and mucin-rich.
Coexistence with other polyp types can occur.
Not all TSAs show adenomatous dysplasia.
It is controversial whether all TSA contain serrated dysplasia ab initio.
References
Footnotes
Handling editor Cheok Soon Lee.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.