Article Text

Abstract
Aims Ki-67 is a prognostic marker in breast cancer; however, the use of the Ki-67 labelling index (LI) in clinical practice requires a consistent and easily accessible scoring method. The present study evaluated the use of the free internet-based image analysis program ImmunoRatio to score Ki-67 LI in breast cancer in comparison with manual counting.
Methods Ki-67 immunohistochemical detection was performed in 577 breast cancer cases, and the Ki-67 LI was determined by ImmunoRatio and manual counting.
Results The Ki-67 LI determined by ImmunoRatio correlated well with that obtained by manual counting. The concordance rate between ImmunoRatio and manual counting was excellent (κ coefficient of 0.881) at a Ki-67 LI cut-off value of 20%. Cases with high Ki-67 LI by ImmunoRatio were associated with poor overall survival, in particular in the hormone receptor positive group.
Conclusions The web-based automated image analysis program ImmunoRatio is an attractive alternative to manual counting to determine the Ki-67 LI in breast cancer.
- BREAST CANCER
- DIGITAL PATHOLOGY
- PROLIFERATION
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Ki-67 is a nuclear antigen linked to the cell cycle that is commonly used to measure cellular proliferation rate. Ki-67 immunohistochemistry is used to evaluate proliferative activity in breast cancer and is a prognostic biomarker for relapse and survival in patients with breast cancer.1–3 Ki-67 expression is also a predictive marker of treatment response in preoperative chemotherapy for breast cancer.4 ,5 Ki-67 labelling index (LI) is the standard criterion for breast cancer classification according to the St. Gallen International Breast Cancer Conference.6 Ki-67 LI and expression of the oestrogen receptor (ER), progesterone receptor (PR) and HER2/neu are used to categorise patients with breast cancer similar to intrinsic molecular subtypes, and these classifications help guide therapeutic decisions.6
Ki-67 expression is an important biomarker in breast cancer, and a reliable and consistent measurement and scoring method is required. However, interlaboratory, interobserver and intraobserver variability limit the accuracy of Ki-67 scoring and its clinical application.7 The recommended guidelines for Ki-67 assessment aim to minimise preanalytical variability in Ki-67 immunohistochemistry of breast cancer specimens.1 Quantitative analysis of digital images for scoring Ki-67 LI can reduce interobserver and intraobserver variability and provides consistent counting for Ki-67 positivity.8 However, most automated image analysers require expensive equipment or software installation and a technician for the operating program. The internet-based application ImmunoRatio is a free image analysis program for scoring immunostained slides. ImmunoRatio is easily accessible and has no requirements regarding equipment or software installation.
The aim of the present study was to validate the ImmunoRatio program for Ki-67 LI scoring in breast cancer. The Ki-67 LI was determined using the ImmunoRatio method and compared with that obtained by manual counting, and the prognostic significance of the Ki-67 LI in breast cancer was evaluated.
Method
Patient selection and Ki-67 immunohistochemistry
A total of 589 patients who underwent surgical resection for breast cancer between January 2003 and December 2007 were selected from the archives of Seoul St. Mary's Hospital. All patients had participated in a previous study by Cho et al9 and the same tissue microarray (TMA) blocks were used in the present study. Briefly, H&E stained slides, immunohistochemical staining (ER, PR, HER2/neu and Ki-67), and HER2/neu silver-enhanced in situ hybridisation data were pathologically reviewed. The results were scored and classified into intrinsic breast cancer subtypes as described previously.9 ,10 Clinical records including breast cancer-specific overall survival were reviewed. This study was approved by the Institutional Review Board of Seoul St. Mary's Hospital (KC14SISI0544).
TMAs containing representative or invasive tumour fronts were constructed using formalin-fixed paraffin-embedded breast cancer specimens with a 2.0 mm core. TMAs were sectioned on precoated glass slides. Immunohistochemical staining for Ki-67 (MIB-1; 1:50, Dako, Glostrup, Denmark) was performed using the Ventana NX automated immunohistochemistry system (Ventana Medical Systems, Tucson, Arizona, USA).
Assessment of Ki-67 labelling index
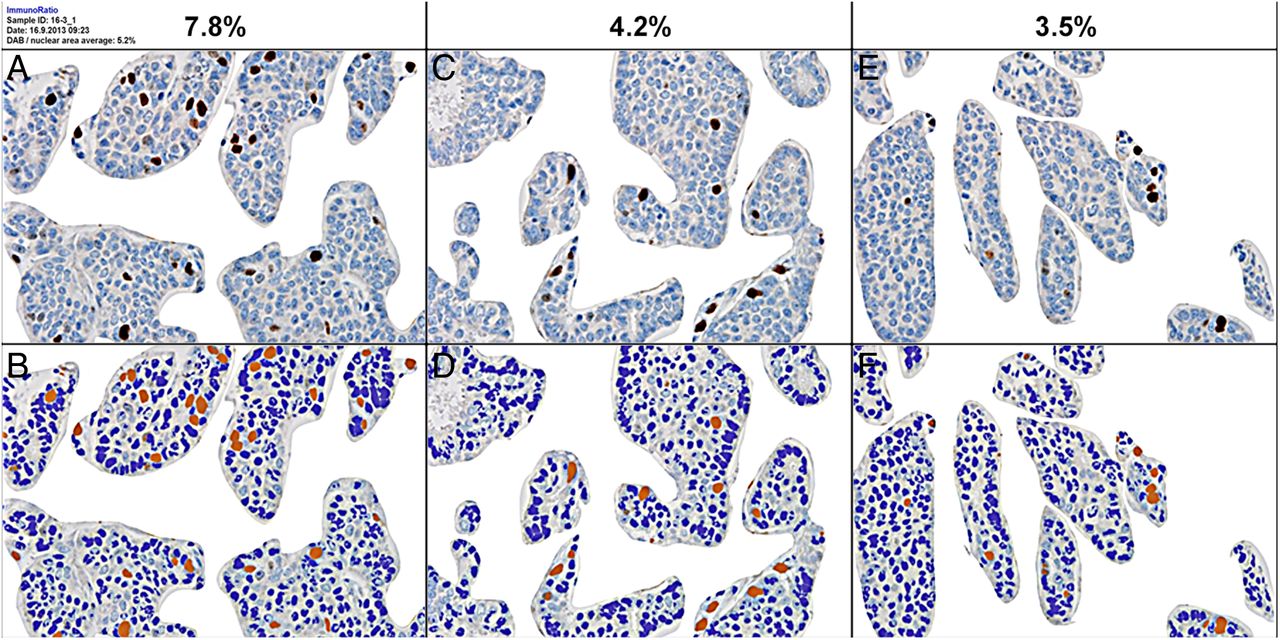
Ki-67 immunohistochemistry was scored using ImmunoRatio and by manual counting. At least three different fields representing the area of highest Ki-67-positive tumour cell density (hot spot) and two areas of average Ki-67-positive tumour cell density within the invasive component were selected, and more than 1000 malignant cells were counted. Ki-67 stained slides were scanned using an Olympus BX51 microscope equipped with an Olympus DP72 digital camera. The ImmunoRatio program can be freely accessed online for image analysis and scoring of immunostained slides (http://153.1.200.58:8080/immunoratio/). Prior to using the ImmunoRatio program, all captured images were edited to exclude stromal tissue from tumour nests (figure 1). The edited images of TMAs with one blank field were uploaded and the ImmunoRatio program was used in ‘Advanced mode’. The brown and blue threshold adjustments were set at 30 and −3. Diaminobenzidine (DAB)-stained and haematoxylin-stained nuclei were segmented by colour threshold, and the uploaded image generated a pseudo-coloured (montage) image matching the area segmented with the percentage of Ki-67 LI (figure 2). A total of 589 cases were analysed using ImmunoRatio and 12 cases could not be interpreted (see online supplementary figure S1).

Ki-67 immunohistochemically stained slides were scanned and edited to remove stromal tissue from the tumour nest before the use of ImmunoRatio (A→B, C→D).

Uploaded Ki-67 images were convoluted to ImmunoRatio pseudocoloured (montage) images (A→B, C→D and E→F). ImmunoRatio recognised diaminobenzidine (DAB) and haematoxylin staining separately and scored the Ki-67 labelling index (LI).
supplementary figure
The manual counting data for Ki-67 was performed as described by Cho et al.9 In short, manual counting of Ki-67 was performed on a computer monitor using scanned images. All tumour nuclei and Ki-67 positively stained nuclei were identified with the naked eye and cells were counted by clicking on the images. The Photoshop program (Adobe Photoshop CS5 extended) was used to count the number of cells tracked by the number of clicks and the running total was displayed in the measurement log panel.
Statistical analysis
The correlation between Ki-67 LI using ImmunoRatio and manual counting was evaluated by parametric and non-parametric methods with Spearman's ρ. Consistency using Ki-67 cut-offs between ImmunoRatio and manual counting was analysed with κ statistics (κ with >0.80, very good; 0.60–0.79, good; 0.40–0.59, moderate agreement).11 Kaplan-Meier survival with the log-rank test was used to compare breast cancer-specific overall survival. All statistical analyses were performed using SPSS V.22.0 (SPSS, Chicago, Illinois, USA) and statistical significance was assumed when p<0.05.
Result
Clinical and pathological characteristics
Of the 577 cases evaluated, most were women (99.5%) and the median age was 49 years (range 21–83). The majority of cases presented with moderately differentiated (48.4%) and intermediate nuclear grade (55.1%) breast cancer. There were 315 cases (54.6%) with stage T1 disease, and lymph node metastasis was present in 251 cases (43.5%). Subtype classification showed that 79.9% of cases were luminal type A or B, 4.9% were HER2/neu type and 15.3% were basal-like type. The mean follow-up period was 75.8 months (range 2–130), and the 5-year survival was 90.0%.
Comparison of Ki-67 LI using ImmunoRatio and manual counting
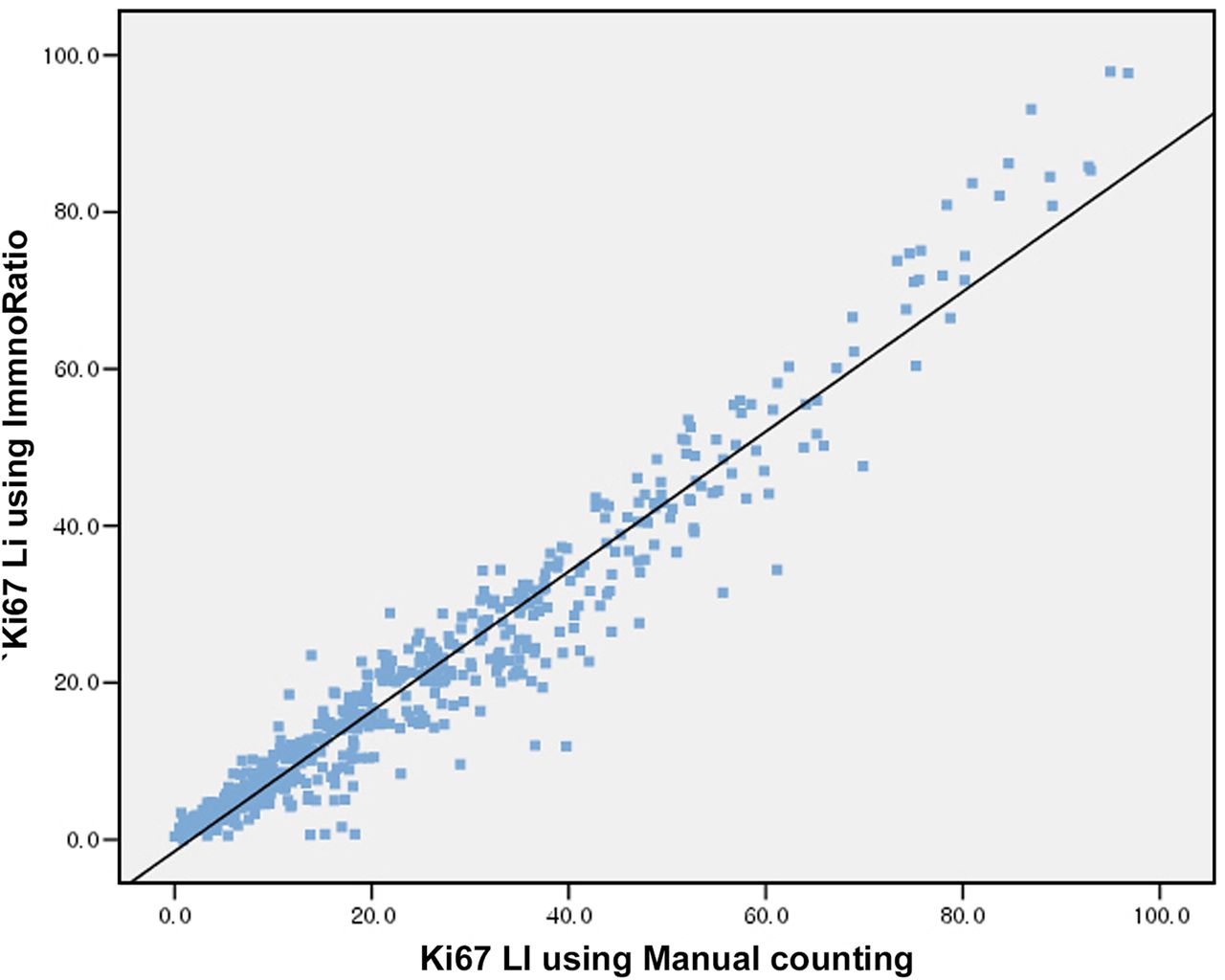
The mean Ki-67 LI was 20.3±18.2 by ImmunoRatio and 24.4±19.8 by manual counting. The correlation between ImmunoRatio and manual counting for Ki-67 LI was excellent (Spearman's ρ=0.96, p=0.000) (figure 3). The prognostic significance of Ki-67 LI in breast cancer was evaluated using a 20% cut-off value.12 ,13 Excellent agreement between Ki-67 LI using ImmunoRatio and manual counting was obtained at a 20% cut-off with a κ coefficient of 0.881.

Excellent correlation between the Ki-67 labelling index (LI) using ImmunoRatio and manual counting.
The prognostic significance of Ki-67 LI on breast cancer
Kaplan-Meier survival curves showed a significant association between poor overall survival and high Ki-67 LI using ImmunoRatio and manual counting in a total of 577 breast cancer cases (p=0.038 and p=0.019, respectively) (figure 4).

Kaplan-Meier overall survival curves based on the Ki-67 labelling index (LI) using ImmunoRatio (A) and manual counting (B) using a 20% cut-off value in a total of 577 breast cancer cases.
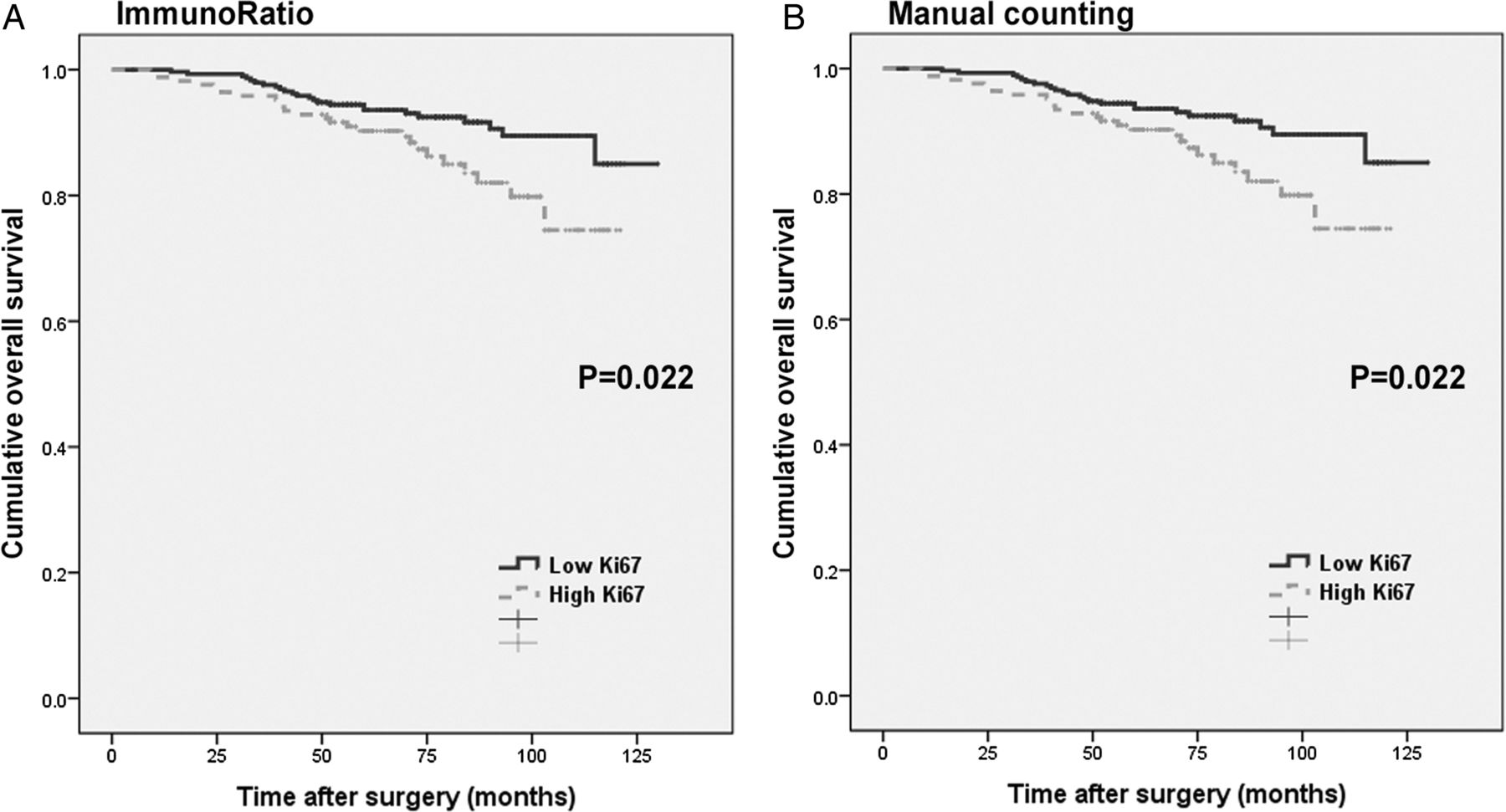
High Ki-67 LI by ImmunoRatio and manual counting was significantly associated with worse survival in 461 cases in the hormone receptor positive group (including luminal type A and B) (p=0.022 and p=0.022, respectively) (figure 5). Ki-67 LI was not associated with overall survival in the hormone receptor negative group (p=0.544 for ImmunoRatio and p=0.955 for manual counting).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In the hormone receptor positive group, Kaplan-Meier curves show a relationship between poor overall survival and high Ki-67 labelling index (LI) (20% cut-off) using ImmunoRatio (A) and manual counting (B).
Multivariate analyses was performed using the Cox proportional hazards model including age, sex, tumour size, lymph node metastasis, nuclear grade, ER status and Ki-67 LI using the 20% cut-off in a total of 577 breast cancer cases (see online supplementary table S1). The multivariate analyses did not show a significant association between overall survival and Ki-67 LI by ImmunoRatio and manual counting (p=0.226 and p=0.389, respectively). Lymph node metastasis was the only significant prognostic factor for prediction of poor overall survival in multivariate analyses (p=0.000).
supplementary tables
High Ki-67 LI by ImmunoRatio and manual counting was not significantly associated with worse survival in 461 cases in the hormone receptor positive group (including luminal type A and B) using the Cox proportional hazards model including age, tumour size, lymph node metastasis, nuclear grade and ER status (p=0.210 and p=0.274, respectively) (see online supplementary table S2).
Discussion
Ki-67 is the most common tumour proliferation marker in breast cancer. Ki-67 proliferative activity has prognostic value for patient survival and is a predictor of response to therapy in breast cancer.14 To increase the clinical utility of Ki-67, an accurate and reliable Ki-67 scoring method is needed to support the clinical demand. The International Ki-67 in Breast Cancer Working Group recommends manual scoring of Ki-67 LI; however, accurate manual counting of a large number of tumour cells is time consuming and cumbersome in daily pathology practice.1 To improve the utility and reproducibility of the Ki-67 LI, various image analysis programs have been commercially developed.
The ImmunoRatio is a free, automated web-based image analysis application for scoring immunostained slides. The present study attempted to validate the ImmunoRatio method by scoring the Ki-67 LI in 577 breast cancer samples and comparing the results obtained by ImmunoRatio with those obtained by manual counting. The Ki-67 LI correlation between the ImmunoRatio and manual counting was good (Spearman's ρ=0.96, p=0.000). The International Ki-67 in Breast Cancer Working Group recommends that the Ki-67 cut-off point for prognosis should be applied only after careful validation, and the analysis should be performed in a highly experienced laboratory with its own reference data.1 The present study used a 20% cut-off value for the Ki-67 LI as previously suggested.9 High Ki-67 LI was associated with poor breast cancer-specific survival with cut-off values of 14% and 20%, but a 20% cut-off showed a higher HR than 14% did in previous and present studies. Furthermore, in the hormone receptor positive subgroup, high Ki-67 LI was associated with poor survival only with a 20% cut-off.9 The Ki-67 LI showed prognostic significance at a cut-off point of 20%, as determined using the ImmunoRatio application. Univariate survival analysis revealed a significant association between poor overall survival and high Ki-67 LI by ImmunoRatio in 577 breast cancer cases and in 461 hormone receptor positive cases (p=0.038 and p=0.022, respectively) (figures 4 and 5).
Compared with the concordance rate between Ki-67 LI using the eyeballing method (quick scan rapid estimate of whole Ki-67 immunostained slides) and manual counting, ImmunoRatio showed better agreement with manual counting than that of the eyeballing method.9 Considering that the eyeballing method for Ki-67 scoring has poor reproducibility, Ki-67 LI scoring by ImmunoRatio could be a better alternative.8
One of the limitations of the present study is TMA tissue sections, which were used to count Ki-67 LI instead of using whole tissue sections. Focke et al15 reported a concordance of 75% between core needle biopsy and surgical specimen for the Ki-67 LI at the cut-off 20%.
The ImmunoRatio was developed in 2010 and calibrated with the nuclear ER, PR and Ki-67 immunohistochemistry markers in breast cancer specimens. The program uses a colour deconvolution algorithm that recognises DAB and haematoxylin-stained nuclei separately by picture thresholding. Original and pseudocoloured (montage) images are shown together to determine whether the result is optimally compatible with the original slide and the positive staining percentage is calculated. Unlike other commercial image analysis software programs that recognise malignant cells by size, the ImmunoRatio cannot discriminate tumour cells from normal cells. A previous study using ImmunoRatio to score ER positivity showed moderate agreement with manual counting because of the lack of distinction of cancer from non-cancer nuclei.16 To overcome this limitation, the stromal tissue was removed from the tumour nest in all uploaded images to count only breast cancer cells. As a result, the correlation between Ki-67 LI using ImmunoRatio and manual counting was excellent.
Staining quality is important for automated image analysis. Variation in the appearance of stained nuclei can be difficult to interpret using image analysis programs. Poorly fixed clear tumour nuclei can be missed during counting, and strong counterstaining disturbs recognition of positive staining.1 ,16 In the present study, Ki-67 LI could not be determined in 12 cases, montage images could not be acquired in 7 cases and discordant images were created in 5 cases (see online supplementary figure S1). All failed cases showed a poorly fixed nuclear appearance. The average Ki-67 LI using ImmunoRatio was lower than that obtained by manual counting. It was assumed that weakly stained Ki-67 nuclei were considered positive by manual counting; however, some of the nuclei were not recognised as positive because of the picture thresholding of the ImmunoRatio program. Therefore, careful modulation of the picture threshold setting based on original Ki-67 stained slide before using advanced mode of ImmunoRatio was important for the result reliability.
In conclusion, the Ki-67 LI determined using the web-based image analysis application ImmunoRatio was highly correlated with that obtained by manual counting. The Ki-67 LI by ImmunoRatio had prognostic value to predict breast cancer survival. The assessment of Ki-67 LI using ImmunoRatio is an attractive alternative to manual counting in breast cancer.
Take home messages
The Ki-labelling index (LI) determined by ImmunoRatio, a free web-based image analysis program, correlated well with that obtained by manual counting.
High Ki-67 LI (cut-off value of 20%) by ImmunoRatio was associated with worse survival in a total breast cancer cases and hormone receptor positive cases.
ImmunoRatio is an attractive alternative to manual counting to determine the Ki-67 LI in breast cancer.
References
Footnotes
Handling editor Cheok Soon Lee
Contributors M-KY: analysed and interpreted data and wrote the paper. HEK: performed experiments. SHK: provided data. BJC: provided data. BJS: provided data. AL: designed the study, performed experiments and approved the final version of the paper.
Funding This study was supported by Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Science, ICT and Future Planning (2014R1A1A3049554).
Competing interests None declared.
Ethics approval Institutional Review Board of Seoul St. Mary's Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.