Article Text

Abstract
Immunohistochemistry is a valuable adjunct in routine gynaecological pathology. The molecular revolution has redesigned knowledge of gynaecological cancers and refined histological classification. The direct consequence has been the progressive introduction of new immunostainings for diagnostic and classification purposes. Hence, we review the routine diagnostic use of immunohistochemistry in the field of gynaecological neoplasia. We reviewed the immunomarkers useful in gynaecological pathology according to literature revision, our personal experience and research findings. We discuss the application of immunohistochemistry to reach the most accurate diagnosis in morphologically equivocal cases of gynaecological pathology and present the appropriate panel of immunomarkers in the most common scenarios of gynaecological pathology. This short review provides an updated overview of the essential immunohistochemical markers currently used in the diagnostics of gynaecological malignancies along with their molecular rationale.
- immunohistochemistry
- ovarian tumour
- gynaecological pathology
- diagnostics
- diagnosis
Statistics from Altmetric.com
Introduction
Immunohistochemistry (IHC) combines microscopic morphology with accurate molecular identification and allows in situ visualisation of any specific protein antigen. The introduction of IHC in diagnostic pathology has revolutionised routine practice, and IHC studies have significantly contributed to a better understanding and subtyping of many malignancies, initially lymphoid neoplasms. Furthermore, IHC has become an integral part of the definition of the majority of solid tumours and is progressively gaining a foothold in guiding anticancer therapy. Among other examples, HER2/neu and oestrogen receptor (ER) expression is routinely used to identify patients with breast cancer eligible to trastuzumab and tamoxifen, respectively.
With the boost and consequential widespread use of advanced technologies, molecular studies that claim to have discovered novel candidate makers with diagnostic, predictive, prognostic or therapeutic value are published daily. In this context, the responsibility of the pathologist is increasing. Besides making tissue diagnosis, they are also in charge of (1) guaranteeing the adequacy of samples used for diagnostic tests, which will be translated into therapeutic decisions, (2) performing IHC biomarker analysis and (3) assisting the development of novel tissue biomarkers. Over the last decade, molecular studies have unveiled the molecular genetic pathway of gynaecological malignancies and enriched the portfolio of IHC markers useful in the differential diagnosis of gynaecological diseases. Accordingly, IHC represents a solid adjunct for the classification of gynaecological malignancies that improves interobserver reproducibility1 and has the potential of revealing unexpected features. However, interpretation in the light of knowledge-based specificity of each single marker along with histopathology expertise and stringency is still the sine qua non. A satisfactory IHC must localise cells and tissue targets, clearly and specifically, keeping the non-specific background to a minimum level.
Here, we will describe the panels of IHC markers used in the most common scenarios of differential diagnosis seen in routine gynaecological pathology, along with their rationale. Though beyond the scope of this paper, clinical information and macroscopical and microscopical features will be outlined at times since they still represent a keystone for the correct diagnosis and characterisation of many pathological entities.
Looking at the ovary
Primary ovarian tumours are summarised in three main subgroups with well-defined clinicopathological characteristics: epithelial, germ-cell and sex-cord stromal tumours (table 1).2 However, metastatic tumours and primary tumours derived from non-ovarian-specific lymphoid or stromal cells (ie, lymphomas, leukaemias and soft-tissue tumours) should not be ignored since they represent a large proportion of ovarian malignancies.
Clinicopathological characteristics of ovarian tumours
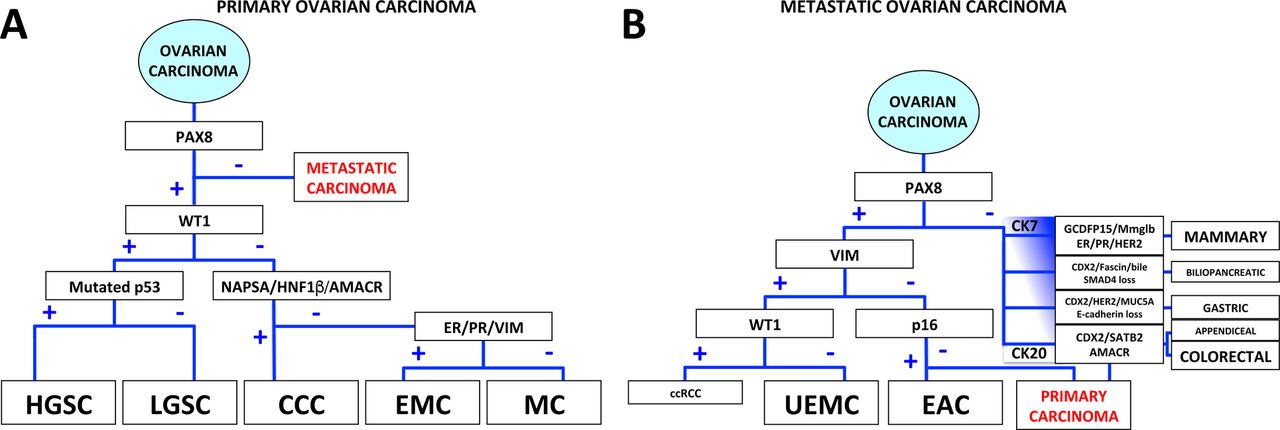
Currently, PAX8 is emerging as the most specific marker to distinguish a primary ovarian carcinoma from a metastasis, but it lacks sensibility as it is also expressed in metastasis from the endocervix, kidney and thyroid (see figure 1 and table 2).1 The most common malignancy of the ovary is high-grade serous carcinoma (HGSC) that together with other serous tumours of the adnexa (low-grade serous carcinoma and borderline serous tumour) are now thought to derive from the fallopian tube epithelium.3 4 Coherently, these tumours demonstrate consistent nuclear expression of Müllerian marker WT1, which is highly expressed in the normal tubal epithelium.3 WT1 is the most sensitive and specific marker for serous histotype and can be used to discriminate serous tumours from all other histotypes.

Immunohistochemical algorithm proposed to diagnose ovarian carcinomas, both primary and metastatic. (A) This algorithm addresses the distinction of morphologically equivocal primary ovarian carcinomas using five to nine immunomarkers. (B) The stepwise immunohistochemical approach for metastatic ovarian carcinomas uses six main immunostainings plus other tissue-specific markers. Because CK7 and CK20 are often coexpressed, they are schematically represented as a continuous vertical from prevalent CK7 positivity (upper end) to prevalent CK20 positivity (lower end). The frequency of the metastatic disease is correlated with font size. CCC, clear cell carcinoma; ccRCC, clear cell renal cell carcinoma; CK, cytokeratin; EAC, endocervical adenocarcinoma; EMC, endometrioid carcinoma; ER, oestrogen receptor; GCDFP15, gross cystic disease fluid protein-15; HGSC, high-grade serous carcinoma; LGSC, low-grade serous carcinoma; MC, mucinous carcinoma; Mmglb, mammaglobin; NAPSA, Napsin A; PR, progesterone receptor; UEMC, uterine endometrioid carcinoma; VIM, vimentin.
Immunohistochemical (IHC) markers in the differential diagnosis of ovarian tumours
Recently, a practical approach to the use of IHC in the classification of primary ovarian carcinomas has been proposed and presented as an IHC algorithm.1 This algorithm results in a hierarchical decision tree, and takes advantage of four IHC markers, including WT1, p53, Napsin A and progesterone receptors (PR), to subclassify primary ovarian carcinomas. We propose a modified IHC algorithm (figure 1A) that includes other interchangeable markers, namely HNF1β and AMACR (also known as racemase or p504S) for clear cell carcinoma (CCC), and ER and vimentin for endometrioid carcinoma, to gain flexibility in routine practice. Moreover, we propose an algorithm (figure 1B) for approaching either ovarian carcinomas with an unusual morphology, with regard to ovarian primary, or suspected metastasis of unknown origin, that keeps into account both the frequency of metastasis and the morphological similarity.
Endometrioid carcinoma versus high-grade serous carcinoma
HGSC with glandular and cribriform growth may closely resemble endometrioid carcinoma. In addition to WT1 expression, virtually all HGSCs show an aberrant p53 protein expression due to TP53 somatic mutation.4 Specifically, in HGSC p53 is overexpressed, in that it is diffusely and intensely nuclear positive, in 60%–70% of HGSCs because of missense mutation, whereas it is entirely negative in the remaining cases due to truncating mutation. Notably, p53 may also be aberrant in almost 30% of endometrioid carcinomas, particularly in those with high nuclear grade. Besides this, p16 expression tends to be intense and diffuse or completely blank in HGSC, while in endometrioid carcinoma, it shows a ‘mosaic’ pattern. Usually, endometrial carcinoma expresses cytoplasmic vimentin, as opposed to HGSC. Half of endometrioid carcinomas harbour CTNNB1 mutations, which cause nuclear translocation of β-catenin, differently from HGSC.5 6 More recently, ARID1A somatic mutation and concurrent protein expression loss have been identified in up to 50% of endometrioid carcinomas.7 Also, the tumour suppressor PTEN is mutated and the protein lost in almost 70% of endometrioid carcinomas; IHC downregulation for PTEN is also reported in up to 52% of HGSCs due to either homozygous deletion or hemizygous loss.8 Moreover, cyclin E1 expression and CCNE1 amplification have been reported in many HGSCs, but are absent in endometrioid carcinomas.9–11
Clear cell carcinoma versus high-grade serous carcinoma
Distinguishing HGSC with cytoplasmic clearing from CCC, or vice versa CCC with eosinophilic cytoplasm from HGSC, may be challenging. Useful markers include WT1 and ER chiefly expressed in HGSC, along with aberrant p53, as well as nuclear HNF1β and cytoplasmic Napsin A and AMACR positive in CCC,12 and negative ARID1A in up to 57% of CCCs.
Advanced ovarian versus uterine serous carcinoma
Disseminated serous carcinomas that contemporarily involve ovaries, uterus and peritoneum represent a challenge for delineating the site of origin. WT1 is the most reliable marker in this setting and marks HGSC diffusely and uterine serous carcinoma (USC) only in up to one-third of cases, in a variable way. Specifically, in cases of synchronous involvement of both the endometrium and ovaries, WT1 is mainly worthy if it is negative at both locations, supporting an endometrial primary, or if the staining patterns are different at the two sites, suggesting two independent tumours.13–15
Peritoneal serous carcinoma versus epithelioid mesothelioma
Epithelioid mesothelioma may closely resemble serous carcinoma, both low-grade and high-grade. Among the useful immunomarkers to distinguish these neoplasias, there are calretinin, keratin 5/6 and D2-40 positive in mesothelioma and PAX8, ER, claudin-4, MOC31 and Ber-EP4 expressed by serous carcinoma.16 17 Although PAX8 positivity has been reported in a relevant proportion (6%–18%) of peritoneal malignant mesotheliomas, usually the staining is weak and focal.18–20 The most reliable recently discovered markers for the diagnosis of mesothelioma are loss of BRCA-associated protein 1 (BAP1) by IHC and deletion of p16 by fluorescence in situ hybridisation; therefore, these markers can certainly help in this differential diagnosis.21–24
Mucinous adenocarcinoma: ovarian primary versus metastatic
The most difficult differential diagnosis in the ovarian cancer field concerns mucinous tumours since both morphological and immunophenotypical features are shared between primary and metastatic tumours. Indeed, macroscopic features and clinical correlation remain fundamental for a correct diagnosis (table 1).2 Immunohistochemically, there is a significant overlap in the immunophenotypes between primary mucinous ovarian carcinoma and metastatic gastrointestinal carcinoma. Typically, CK20, CDX2 and SATB2 are expressed by colorectal adenocarcinoma and show an intense and diffuse pattern. Notably, they are negative, or only focal and weak, and in any case less intense and diffuse than CK7, in primary ovarian carcinomas, with the only exception being the rare intestinal-type mucinous ovarian tumours originating from ovarian teratomas.25
In primary ovarian mucinous tumours, besides cytokeratin 7 (CK7) and CA125, PAX8 is expressed in 65% of cases, but not in colorectal adenocarcinomas.26 Notably, CA125 is not ovarian specific; even breast, lung, pancreas, cervix and uterine carcinomas and mesothelioma may be positive. Therefore, though CK20+/CK7− is prototypical for metastatic adenocarcinomas from the lower intestinal tract and this immunoprofile can be definitive for correct diagnosis, often it is necessary to resort to lineage-specific markers PAX8 and SATB2, both highly specific but defectively sensitive.26 27 In this situation, ER and PR are of limited value since they are negative in both intestinal-type primary and metastatic carcinomas, whereas CDX2 is a site-unspecific marker of intestine differentiation (see below).28–30
Finally, and uniquely, SMAD4 (DPC4) is lost in half of all pancreatic cancers.31 32 A summary of the many tissue-specific IHC markers that may help in the differential diagnosis of tumours from various sites is reported in table 2 and representative pictures in figure 2.2 12 33–36

Representative images of the most helpful immunostainings used in the differential diagnosis of ovarian epithelial tumours. β-cat, β-catenin; CCC, clear cell carcinoma; EMC, endometrioid carcinoma; HGSC, high-grade serous carcinoma; MC, mucinous carcinoma; META, metastatic mucinous carcinoma; SMT, seromucinous tumour.
Small cell carcinoma of hypercalcaemic type versus other mimics
Small cell carcinoma of hypercalcaemic type (SCC-HT), a rare but aggressive tumour, can simulate mainly HGSC and adult granulosa cell tumour, but typically arises in children and young women, and is associated with hypercalcaemia. Similarly to HGSC, SCC-HT also demonstrates IHC positivity for p53 and WT1. Characteristically, SCC-HT shows calretinin positivity, similar to granulosa cell tumours, although focal and weak. Morphologically, SCC-HT is reminiscent of small cell lung carcinoma and present hyperchromatic, ungrooved nuclei, with frequent mitoses. Recently, it has been shown that SMARCA4 is specifically mutated in over 90% of SCC-HT, and this genetic aberration produces a loss of SMARCA4 (BRG1) protein expression37 that can be used as a valid adjunct in the differential diagnosis of SCC-HT.
Clear cell carcinoma versus yolk sac tumour
CCC and yolk sac tumour share many morphological features, such as glycogen-rich clear cells with atypical nuclei with occasional nucleoli and infrequent mitoses, papillary growth, loosened oedematous pattern, hyaline globules and HNF1β positivity. Importantly, CCC often arises in a background of endometriosis, or clear cell adenofibroma, and it is usually positive for AMACR, CK7, EMA and Napsin A and negative for AFP and glypican 3, as opposed to yolk sac tumour.33 38 39 Moreover, SALL4, a specific and sensitive marker for germ cell tumours, may reliably distinguish yolk sac tumour since it stains intensely and diffusely almost all cases analysed, but it is negative or very rarely only focal in CCC.39 40
Looking at the fallopian tube
Serous tubal intraepithelial carcinoma versus other mimics
Ever-growing evidence identifies serous tubal intraepithelial carcinoma (STIC) as the most likely precursor lesion of HGSC. To solve doubtful tubal lesions, a diagnostic algorithm, which includes marked cytological atypia, Ki-67 proliferation index and p53 IHC, has been proposed.41 42 Based on this algorithm, STICs are intramucosal tubal lesions that combine cytological atypia with Ki-67 proliferation index >10% and p53 IHC mutant pattern.
Looking at the uterus
Endometrial carcinoma subtyping
Since 1983, endometrial carcinoma has been proposed to follow a dualistic pathogenetic model.43 Endometrioid carcinoma is the prototypical type I endometrial carcinoma, whereas type II tumours include USC, CCC, malignant mixed Müllerian tumour and undifferentiated carcinoma. Their distinction, usually elementary, has important implications for pathobiology and treatment. In some instances, such as glandular–cribriform USC, papillary endometrioid carcinoma and endometrioid carcinoma with clear cells, their discrimination may be difficult and IHC aids may be necessary (table 3). Endometrioid carcinomas are usually ER and PR positive, whereas USC and CCC are negative.44 In addition, USC harbours TP53 mutation and a mutant p53 IHC pattern (see above), whereas endometrioid carcinoma and CCC are usually TP53 wild-type.43 Conversely, endometrioid carcinoma and CCC harbour ARID1A , CTNNB1 and DNA mismatch repair gene ( MMR ) mutations and a mutant IHC pattern (figure 3).45 Interestingly, p16 tends to be strongly and diffusely positive in USC, only focal in endometrioid carcinoma and negative in CCC. Finally, diffuse HNF1β and Napsin A positivity favours CCC.46 Notably, also Arias-Stella reaction and some endometrioid carcinomas may express HNF1β.

(A) Endometrioid carcinoma associated with Lynch syndrome shows prominent peritumoural lymphocytes (H&E staining, upper picture), and retention of MLH1 and PMS2 and loss of MSH2 and MSH6 by immunohistochemistry. (B) Correlation between mutations, immunohistochemical (IHC) expression of mismatch repair (MMR) genes and microsatellite instability (MSI) status in Lynch syndrome-associated cancers. HE, haematoxylin–eosin; +, positive nuclear staining; −, negative nuclear staining; H, high; L, low.
Immunohistochemical (IHC) markers in the differential diagnosis of endometrial carcinomas
Undifferentiated carcinoma deserves its own chapter. Characteristics of this entity include the IHC negativity or only focal positivity for CKs (AE1/AE3, 8, 18, 8/18), vimentin, EMA, ER, PR, chromogranin, synaptophysin, E-cadherin and CTNNB1, TP53 and MMR gene mutation in about 30%, 30% and 50% of cases, respectively.5 47 Recently, McCluggage’s group reported CD34 IHC expression in 29% of undifferentiated carcinomas and found a relative frequency of loss of IHC expression of SMARCA4 and SMARCA2, members of the SWI/SNF chromatin-remodelling complex.48 49
Malignant mixed Müllerian tumour (ie, carcinosarcoma) is an aggressive biphasic tumour composed of both carcinomatous and sarcomatous cells. Usually, morphological features are sufficient to diagnose this entity. In rare cases, high p53/WT1 and low ER/PR expression are helpful for differentiating malignant mixed Müllerian tumours from endometrioid carcinomas with spindle cell differentiation.50 51
Endometrial hyperplasia versus endometrioid intraepithelial neoplasia versus endometrioid carcinoma
The new classification that defines endometrioid intraepithelial neoplasia (EIN, also known as atypical hyperplasia) as a monoclonal mutated precursor of endometrioid carcinoma permits the use of IHC markers of early mutation to tell endometrial hyperplasia apart from EIN. To this end, nuclear β-catenin and MLH1 or PTEN loss have been demonstrated useful.52 53 In addition, several authors have reported the utility of PAX2 loss to decipher tricky EIN cases.54–57
Furthermore, diagnostic problems in distinguishing EIN from well-differentiated endometrioid carcinoma have long been studied, but there still is no reliable marker, other than the careful and strict implementation of histopathological criteria specifically defined for diagnosis of endometrioid intraepithelial neoplasias.58 On the other hand, although both lesions show PTEN loss, additional loss of ARID1A and increased Ki-67 proliferation index may warn for endometrioid carcinoma.59 60
Müllerian adenosarcoma versus endometrial polyp
The peculiar phyllode-like growth pattern, periglandular stromal hypercellularity and mild–moderate atypia characterise Müllerian adenosarcoma. When morphological features are not conclusive, Ki-67 IHC may help since adenosarcoma shows a zonal periglandular increase of Ki-67, in contrast to the endometrial polyp and atypical polypoid adenomyoma.61
Endometrial stromal sarcoma
The classification of endometrial stromal sarcomas has been refined on the basis of the molecular characteristics recently identified. The most recent WHO classification identifies three different sarcomas likely derived from endometrial stromal cells: low-grade endometrial stromal sarcoma, high-grade endometrial stromal sarcoma and undifferentiated uterine sarcoma. Indeed, low-grade and high-grade endometrial stromal sarcomas are characterised by a simple karyotype and distinctive pathognomonic chromosomal translocations, resulting in JAZF1–SUZ12 and YWHAE–NUTM2A/B gene fusions, respectively.62–64 However, molecular testing is not currently standard practice; therefore, immunophenotype is helpful in the differential diagnosis. Typically, low-grade endometrial stromal sarcomas show diffuse immunopositivity for CD10, ER and PR.65 In contrast, high-grade endometrial stromal sarcomas lack CD10, ER and PR expression and display a strong nuclear positivity for cyclin D1 and membranous/cytoplasmic reactivity for c-Kit.65–67 Finally, undifferentiated uterine sarcomas include a heterogeneous group of aggressive neoplasias harbouring complex karyotype and showing marked pleomorphism, necrosis and mitotic activity and variable expression of CD10, ER and PR.68 Undifferentiated uterine sarcomas should be diagnosed only after exclusion of the most common mimics: leiomyosarcoma, carcinosarcoma, undifferentiated carcinoma, rhabdomyosarcoma and diffuse large B-cell lymphoma.69
Endometrial stromal versus uterine smooth muscle tumour
Some leiomyomas show morphological similarity to endometrial stromal tumours, particularly cellular leiomyomas. Smooth muscle tumours, as opposed to low-grade endometrial stromal sarcoma, usually express desmin and h-caldesmon but not CD10 70–73 (table 4).
Immunohistochemical markers in the differential diagnosis of endometrial mesenchymal tumours
Leiomyosarcoma versus leiomyoma
Difficult smooth muscle tumours may necessitate taking advantage of IHC because diffuse p53 and p16 and a high Ki-67 proliferation index favour a leiomyosarcoma; however, some smooth muscle tumours with uncertain malignant potential and some leiomyomas rarely show overlapping patterns.74–76
Cervical squamous neoplasia versus benign mimics
The main problem in cervical pathology is to distinguish intraepithelial lesions from their innocuous mimics, such as reactive and metaplastic squamous changes, atrophy and cytological atypia due to cautery artefact. In this context, p16 IHC positivity is a surrogate marker for high-risk human papilloma virus (HPV) infection. Normally, p16 protein is inhibited by Rb negative feedback, which is interrupted during HPV infection. In particular, E7 viral oncogene constitutively inactivates Rb pathway through sequestration of pRb, hence, HPV integration in cycling cervical cells results in a block-type strong and diffuse p16 positivity.77 Notably, p16 IHC positivity specific for high-risk HPV lesions is strong continuous staining, both nuclear and cytoplasmic, involving at least the basal third of the epithelial full thickness (ie, block staining).77 This p16 block positivity is found in the majority of high-grade squamous intraepithelial lesions (HSILs) and only in one-third of low-grade squamous intraepithelial lesions (LSILs). In particular, although HSIL with severe dysplasia (corresponding to CIN-3) is almost invariably positive for p16, nearly one-third of the HSIL spectrum’s lower extremity (corresponding to CIN-2) has been reported to be negative for p16.78 79 Importantly, the new recommendations for squamous lesions of the lower anogenital tract (LAST) include the use of p16 immunostaining in lesions morphologically doubtful for CIN-2, and this practice could jeopardise diagnosis of these p16-negative HSILs, resulting in underdiagnosis as LSIL.77 Next related issue is whether p16-negative CIN-2 behave like p16-positive ones. So far, a definitive answer to this question is missing, and the studies on this topic are limited and contradictory. However, recent studies on intermediate dysplastic lesions found that p16-positive lesions are more likely to persist or progress behaving like HSILs, whereas p16-negative lesions tend to regress as well as LSILs, providing evidence of the clinical ‘correctness’ of LAST recommendations.78 80
In addition, SILs show an increased proliferation index with Ki-67. Along with p16 positivity, Ki-67 may also reliably assist the differential diagnosis between HSIL and LSIL, whereby full-thickness proliferation favours HSIL. Clearly, appropriate orientation of the epithelium is necessary in order to prevent misinterpretation.
Recently, the squamocolumnar junction (SCJ) cells have gained increasing interest as possible cells of origin of SILs, hence, the IHC expression of the SCJ proteins (ie, CK7, CK17, MMP7 and p63) has been studied in SILs.81 82 Interestingly, it has emerged that SCJ markers are strongly and diffusely expressed in HSILs, but either negative or patchy in LSILs, so that they may be used as adjunct IHC markers in distinguishing between HSIL and LSIL. This is particularly true for CK7 since it is widely used. In addition, CK7 expression has been correlated with an increased risk of LSIL progression and accordingly proposed as a risk stratifier.83–85
Cervical glandular neoplasia versus benign mimics
Likewise, endocervical adenocarcinoma in situ (AIS) must be distinguished from potential innocuous mimics such as reactive and reparative glandular changes, tubal metaplasia, microglandular hyperplasia and endometriosis.86 Immunohistochemically, AIS shows increased Ki-67 and diffuse p16 and mCEA, but negative vimentin and ER. Conversely, p16 in benign lesions tends to be negative or focal, and Ki-67 proliferation index is low (<10%).86 87
Endocervical versus endometrial adenocarcinoma
The therapeutic approach for endometrial carcinoma and endocervical-type adenocarcinoma is different; therefore, indicating the cancer origin is of extreme importance, but may be tricky based only on morphology, particularly in curettage samples. Morphological characteristics though may be of guidance. Typically, endocervical adenocarcinoma of the usual type is morphologically characterised by (1) angulated and branching glands, (2) nuclear crowding and pseudostratification, (3) nuclear hyperchromasia and marked atypia, and (4) numerous basal apoptotic bodies and mitotic figures, usually apical. Moreover, endocervical adenocarcinoma is often associated with concurrent AIS and squamous lesions.88 89 On the other hand, endometrioid endometrial carcinoma is characterised by (1) predominant tubular architecture, (2) cells with scant cytoplasm and large vesicular nuclei, not pseudostratified, (3) presence of stromal foamy histiocytes and (4) squamous metaplasia. Commonly, EIN accompanies endometrioid carcinoma.
The general IHC panel for this situation includes ER, PR and vimentin strongly positive in endometrial carcinoma, and p16, mCEA and HPV in situ hybridisation diffusely positive in endocervical adenocarcinoma of the usual type.
Notably, p53 positivity in a cervical carcinoma strongly suggests against common cervical carcinomas, that is, squamous carcinoma or endocervical adenocarcinoma of usual type, and in all cases, a diagnosis of a secondary serous carcinoma should be considered and ruled out.86 However, p53 positivity is present in a consistent percentage of endocervical adenocarcinoma of gastric type or serous carcinoma of the cervix, though the latter variant is exceedingly rare. In addition, HNF1β positivity is not restricted to CCC, but it has been also reported in gastric-type and mesonephric carcinomas.90–92 The IHC markers useful for the diagnosis of endometrial adenocarcinoma and special-type endocervical adenocarcinomas are reported in table 5.
Immunohistochemical markers in the differential diagnosis of endometrial carcinomas versus endocervical adenocarcinomas
Role of immunohistochemistry in the diagnosis of syndromic gynaecological cancers
Both ovarian and endometrial carcinomas can be an indication of genetically inherited syndromes.
Two main hereditary cancer syndromes are known that predispose to cancers occurring in the gynaecological tract, namely Lynch and hereditary breast and ovary cancer syndromes.
Lynch syndrome is due to germline mutations in the MMR system, including MLH1, MSH2, MSH6 and PMS2 genes, and in EPCAM gene that cause high microsatellite instability (MSI) and increase the risk of endometrioid, clear cell and undifferentiated carcinomas. Impaired DNA mismatch repair results in alterations to hypermutable short repetitive sequences in the genome (microsatellites) and its detection conventionally performed by IHC analysis of the aforementioned MMR proteins.93 Lynch syndrome is an under-recognised entity, responsible for 5% of endometrial cancers and 1% of ovarian cancer cases, but high MSI is found in more than 30% of endometrial and around 3% of ovarian carcinomas due to somatic mutations and MLH1 promoter methylation. The pathologist plays a fundamental role in identifying cancers harbouring high MSI. In fact, there are some histological clues suggesting Lynch syndrome: prominent peritumoural lymphocytes, increased lymphocytes (>42 per 10 high-power fields) located within the boundary of tumour cell nests or glands, and tumour heterogeneity, defined as juxtaposed distinct tumour populations constituting more than 10% of the tumour volume, along with an undifferentiated component.94–96 To confirm Lynch syndrome, the pathologist should first apply IHC for MLH1, MSH2, MSH6 and PMS2 (figure 3), which is extremely reliable, then request MSI analysis by PCR. In identifying the presence of MMR germline mutations in EMCs, the sensitivity ranges from 77% to 100% for MSI assay by PCR and from 86% to 100% for MMR IHC, whereas the specificity ranges from 38% to 81% and from 48% to 81%, respectively.97–99 A study by McConechy et al showed 93% of concordance between the two methods in EMCs and stated that the two methods ‘are equivalent’ in detecting MMR defects.97 Importantly, MMR IHC has low cost, fast turnaround time, identifies which gene is mutated and can be performed on routine tissue material.97 On the other hand, MSI assay may identify MMR defects that do not affect IHC stainings or that are in genes not tested by IHC, such as MSH3 and PMS1.100 Moreover, MSI assay is unambiguous, easy to read, highly reproducible and requires less material (one section vs four sections). However, a recent paper found that MSI assay in EMCs, when compared with colorectal cancers, has a slightly higher false-negative rate than IHC due to the high prevalence of one-nucleotide shifts that can be missed by MSI assay.101
Hereditary breast and ovary cancer syndrome is due to germline mutations in breast cancer 1 (BRCA1) and BRCA2 genes. These germline mutations cause about 5%–10% of all ovarian carcinomas and a small minority of endometrial carcinomas. Specifically, women with mutated BRCA1 and BRCA2 have a 40% and a 20% lifetime risk of developing ovarian carcinoma, respectively, and a 2%–3% lifetime risk of developing endometrial carcinoma.102 On the other hand, it is known that about 12% of ovarian HGSCs have disruption of the BRCA pathway due to somatic events, either BRCA1/BRCA2 mutation or BRCA1 promoter methylation. Histologically, cancers with BRCA mutations are typically of high-grade histology, virtually all HGSC in the ovary and either serous or clear cell carcinomas in the endometrium. BRCA-mutated HGSCs show a SET growth pattern (solid, pseudoendometrioid and transitional-like) and, specifically, cases with a BRCA1 mutation also present increased tumour intraepithelial lymphocytes, brisk mitotic indexes and necrosis.103 In addition, a micropapillary infiltrative pattern of metastatic HGSC with BRCA germline mutations is more frequently seen in BRCA1-mutated cases and has been associated with poor prognosis.104
Currently, much effort is devoted to developing BRCA1 and BRCA2 antibodies able to identify patients with compromised BRCA pathway with promising results, but they are not translated yet into daily practice.105 106 Therefore, BRCA testing is mainly based on molecular techniques, as real-time PCR or sequencing, and dedicated to women with a familial history. BRCA pathway alterations are known to cause an improved response to platinum-based therapy and to render patients eligible to PARP (ie, poly(ADP)-ribose polymerase) inhibitors.107–109
Given that mutations causing these syndromes and related somatic molecular alterations are responsible for specific sensitivity or resistance to therapy, it is plausible that they will shortly drive therapeutic choices; however, our knowledge is still lacking.110
Unexpected immunostainings
Any immunohistochemical marker is specific until proven otherwise; as a consequence, some organ-associated immunohistochemical markers, not properly Müllerian, have also been described in gynaecological tumours (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examples of unexpected immunohistochemical stainings in gynaecological neoplasias are shown: CDX2 is weakly positive in an endometrioid carcinoma, mainly in the morular metaplasia; D2-40 positivity in the presented ovarian clear cell carcinoma is intense and apical; a relevant proportion of squamous cell carcinomas of the cervix is convincingly GATA3 positive, but usually focal and weak; and TTF1 can be remarkably positive in endometrioid carcinoma, as shown in the last panels (left panels, magnification ×200; right panels, magnification ×630).
CDX2 is a homeobox transcription factor that is expressed in intestinal epithelial cells and is used in diagnostic pathology as a marker of intestinal carcinoma, mainly colonic, but also oesophageal, gastric and biliopancreatic adenocarcinoma. Interestingly, the CDX2 expression has been identified in lung and bladder carcinomas and considered as a marker of intestinal differentiation.29 Coherently, in gynaecological neoplasms, the CDX2 expression has been well characterised in ovarian mucinous adenocarcinoma (previously called intestinal type) where it is positive between 36% and 94% of cases, as well as in 39% cervical adenocarcinoma, especially of intestinal type.30 34 35 111–113
Moreover, CDX2 positivity in endometrial carcinomas ranged from 6% to 44%. Interestingly, two studies reported that CDX2 expression in endometrial endometrioid carcinoma is associated with morular differentiation.114 115 Analogously, 0% to 30% of ovarian endometrioid carcinomas have been reportedly positive for CDX2.
D2-40 (also known as podoplanin) is a mesothelial and lymphatic endothelial marker. Besides gynaecological adenomatoid tumours, peritoneal mesotheliomas and vascular tumours, a variable proportion of ovarian carcinomas have shown immunopositivity for podoplanin, depending on the histotype.116 117 Specifically, 10%–65% of serous carcinomas, 0%–33% of endometrioid carcinomas, 0%–16% of mucinous carcinomas and 0%–55% of CCCs have been reported positive for podoplanin, and based on one study, the latter showed stronger positivity.116–119 Eventually, podoplanin may help to discriminate dysgerminoma since it is invariably positive in dysgerminoma cells but negative in the other ovarian germ cell tumours.119
GATA3 has a pivotal role in the embryogenesis and differentiation of the breast, urothelial and T cells, and as such, its IHC expression is commonly used as a surrogate marker for mammary and urothelial derivation in neoplasias of unknown origin. In gynaecological pathology, GATA3 has shown a weak and focal positivity in endocervical, endometrial and ovarian adenocarcinoma in up to 18%, 23% and 10%, respectively.120 121 Among special gynaecological tumours, the majority of Brenner tumours are diffusely GATA3 positive, similarly to urothelial carcinoma, but only 50% of transitional cell carcinomas.122 Alike, between 26% and 60% of squamous cell carcinomas are remarkably positive for GATA3, but only focally.120 123 Of note, all gestational trophoblastic tumours and almost the totality of mesonephric carcinomas (95%) express GATA3 consistently.124 125
Thyroid transcription factor-1 (TTF1) is a lineage-specific marker expressed in lung and thyroid parenchyma and primarily used as specific immunomarker of lung and thyroid carcinomas. Recently, TTF1 has been found expressed in a minority of ovarian (3%–39%), endometrial (2%–23%) and cervical adenocarcinomas (4%).126–130
Conclusions
This short review intends to provide an updated overview of the essential IHC markers currently used in the diagnostics of gynaecological diseases along with their molecular rationale. Over the last decade, there have been unpredictable advances in the understanding of the molecular pathogenesis of gynaecological malignancies. It is advised that this knowledge becomes the foundation for a molecularly oriented therapeutic approach to improve the outcome and reduce the side effects of patients with gynaecological cancer.
References
Footnotes
EK and AA contributed equally.
Handling editor Dhirendra Govender.
Contributors EK and AA contributed equally to this manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it was published Online First. The corresponding details has been updated to include Prof Ayse Ayhan.