Article Text

Abstract
Aims Traditionally, a core biopsy diagnosis of radial scar will prompt diagnostic surgery because of the risk of associated malignancy. However, in the absence of atypia, the risk of malignancy is low. The recent introduction of the mammotome device facilitates vacuum-assisted large-volume sampling of a lesion, such that a benign diagnosis may be accepted more confidently, and if the lesion has been entirely removed, it effectively becomes a therapeutic procedure. The aim of this study was to review the role of mammotome excision in the management of non-atypical radial scars in the screening population.
Methods Screen-detected radial scars diagnosed on core biopsy between July 2004 and September 2008 were identified from pathology records. From January 2006, the mammotome device was used to excise non-atypical radial scars on core biopsy, as an alternative to surgery.
Results 22 core biopsy samples containing radial scars without atypia were included in the study; 14 were planned for mammotome excision and eight for diagnostic surgical excision. In the mammotome group, 78% (11/14) of patients had confirmation of non-atypical radial scars and thus avoided an operation. Three of the 14 cases planned for mammotome excision required surgery; in one case, the mammotome cores contained lobular in situ neoplasia, and, in two cases, attempts to sample the lesion with the mammotome were unsuccessful. Only one of the 22 cases ultimately proved malignant. This was a case of ductal carcinoma in situ arising within a radial scar, where the patient proceeded straight to surgery in view of discordance between radiological and pathological features.
Conclusion Utilisation of mammotome excision in the management of non-atypical radial scars successfully avoided surgery in 78% of eligible patients. Pathologists have an important role in selecting patients for mammotome excision by excluding the presence of atypia.
- Radial scar
- mammotome
- needle core biopsy
- breast screening
- breast
- breast pathology
Statistics from Altmetric.com
Introduction
Radial scars are benign foci of proliferative breast disease giving rise to stellate distortions of the tissue architecture. With the advent of population-based screening programmes, radial scars may be seen with increased frequency; the current incidence is 0.6–0.9 per 1000 women screened.1–3 Mammographically, radial scars are seen as an area of architectural distortion with long, thin radiating spicules against a background of radiolucent fat creating a ‘black star’ appearance. Histologically, they have a characteristic appearance with a central fibroelastotic core containing entrapped glandular elements and ducts that radiate outward.4 Diagnosis may be challenging, as both radiologically and histologically the appearances may mimic carcinoma.
Radial scars are in themselves benign, but they may be associated with atypical epithelial proliferations or malignancy in a significant number of cases.2 5–7 In a review of 125 surgically excised radial scars within the Irish screening population, Doyle et al reported malignancy in 24.8% (with a third of cases proving invasive) and atypia, including lobular carcinoma in situ, in 22.4%.8 Traditionally, all radial scars diagnosed on needle core biopsy have been surgically excised because of this potential risk. However, there is increasing evidence that, if the radiological findings suggest a radial scar and the needle core biopsy confirms a radial scar with no atypia, then surgical excision may be unnecessary.9–11
The recent introduction of vacuum-assisted large-volume mammotome biopsy provides an opportunity to sample lesions more extensively such that malignancy may be more confidently excluded. Used in this way, mammotome excision offers an alternative to surgery and, if the lesion has been entirely removed, effectively becomes a therapeutic procedure. Since January 2006, we have used the mammotome device in this way for patients presenting via the NHS Breast Screening Programme. Here we present our initial experience, which confirms the usefulness of this approach.
Methods
Screen-detected radial scars diagnosed on breast needle core biopsy between July 2004 and September 2008 were identified from pathology records. From July 2004 to December 2005, all patients with radial scars diagnosed on needle core biopsy underwent diagnostic surgery. From January 2006, we incorporated the use of the mammotome device in the management of non-atypical radial scars. After multidisciplinary team (MDT) discussion to ensure radiological–pathological concordance, all patients with non-atypical radial scars on needle core biopsy were offered mammotome excision as an alternative to surgery. Exceptions due to technical limitations of the mammotome device include lesions abutting the skin or areola and radial scars exceeding 25 mm.
All core biopsies were performed under stereotactic or ultrasound guidance, using 14-G needles. Vacuum-assisted excision was performed under stereotactic or ultrasound guidance, using the mammotome biopsy system (Ethicon Endo-Surgery, Cincinnati, Ohio, USA) with either 8-G or 11-G needles. All procedures were performed under local anaesthesia in an outpatient setting. For each case, the following data were recorded: (i) patient's age; (ii) screen round; (iii) mammographic size of lesion; (iv) detection of the lesion on ultrasound imaging; (v) number of needle core biopsy samples obtained and image guidance used; (vi) number of mammotome cores obtained and image guidance used; (vii) histology from needle core biopsy, mammotome biopsy and surgical excision; (viii) duration of follow-up.
Results
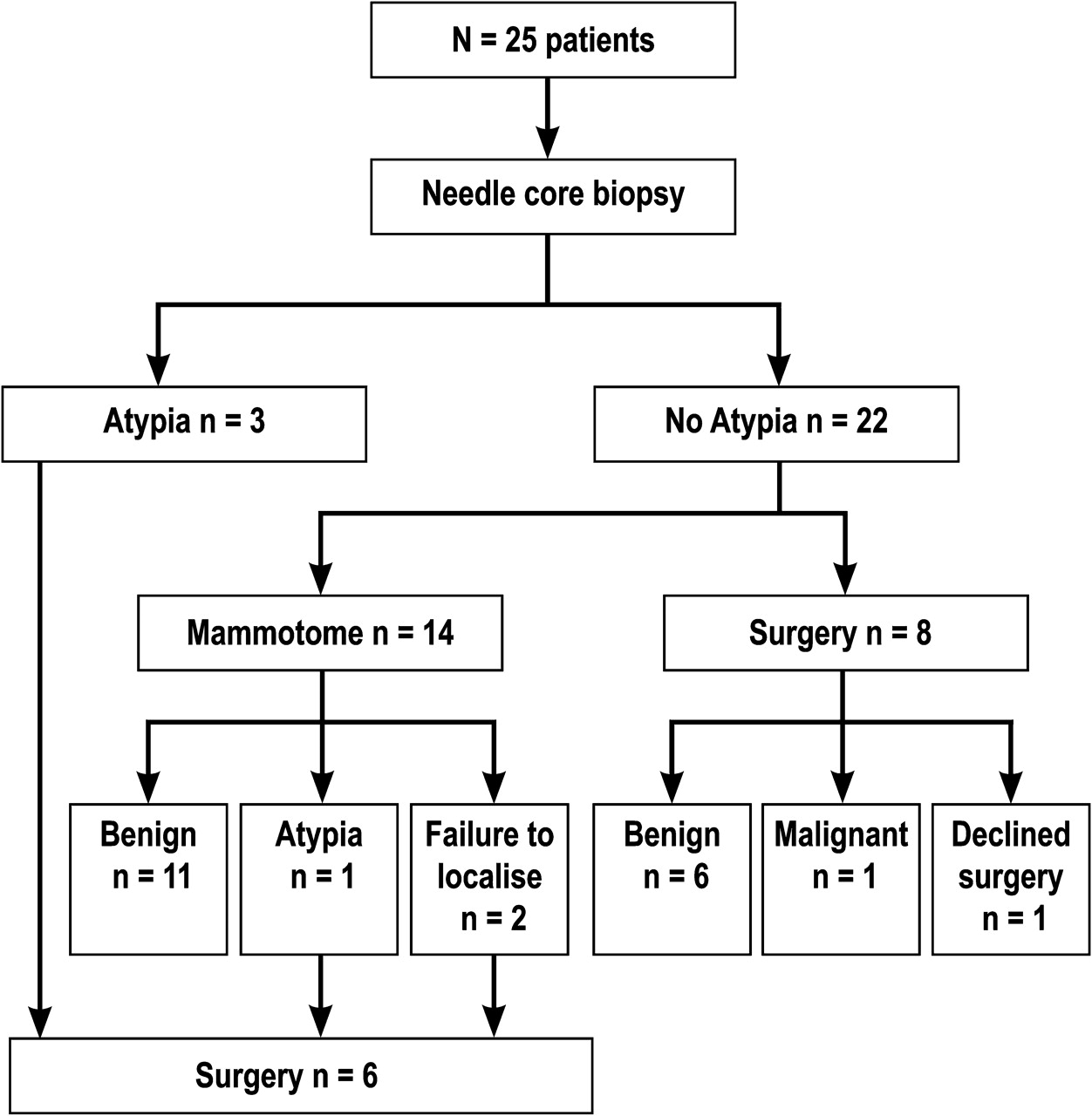
Twenty-five radial scars were diagnosed on needle core biopsy during the study period (figure 1). The mean age at presentation was 58 years (range 49–70), with six cases detected in the prevalent screening round. Maximum mammographic diameter of the radial scars ranged from to 4 to 25 mm (mean 11.8 mm), with nine radial scars visible on ultrasound imaging. Follow-up data were available for all patients (mean=35 months, range 1–5 years).
{kind=link}
Management algorithm for radial scars in the study population.
All 25 core biopsies were performed with a 14-G needle, with a mean of six cores taken per lesion (range 3–10 cores). Nineteen core biopsies were performed under stereotactic guidance, and six under ultrasound guidance. In three cases, the core biopsy samples contained an atypical epithelial proliferation in addition to the radial scar, and these patients proceeded directly to surgery. Of the remaining 22 patients with non-atypical radial scars, six presented before the availability of the mammotome device, and therefore underwent diagnostic surgical excision. From January 2006, there were 16 patients with non-atypical radial scars on needle core biopsy, who were potentially eligible for mammotome excision. However, after MDT discussion, one patient was sent straight to surgery because of radiological–pathological discordance, and one patient with learning difficulties was considered unsuitable for mammotome excision. As a result, of the 22 patients with non-atypical radial scars on core biopsy, 14 were planned for mammotome excision and eight for diagnostic surgical excision (table 1).
Data from patients with non-atypical radial scars on needle core biopsy
Mammotome excision
Fourteen patients with non-atypical radial scars on needle core biopsy were planned for mammotome excision. In one patient (case 14), it was not possible to localise the lesion under stereotactic guidance, and mammotome excision was not performed. Thirteen mammotome procedures were successfully performed, with nine under stereotactic guidance and four under ultrasound guidance. Nine lesions were excised using an 8-G needle, with a mean of 18 cores taken per lesion (range 10–24 cores). Four lesions were excised using an 11-G needle, with a mean of 28 cores taken per lesion (range 18–48 cores).
Histology from mammotome cores confirmed radial scar with no features of atypia or malignancy in 11 cases (cases 1–11), and these patients avoided an operation. Three of the 14 cases planned for mammotome excision required surgery (cases 12–14). One patient (case 12) had atypia in the form of lobular in situ neoplasia (LN) within the radial scar on mammotome cores, prompting surgical excision at this point. The final excision histology showed a radial scar and associated LN amounting to atypical lobular hyperplasia (ALH). One patient (case 13) proceeded to surgery because of inadequate sampling with the mammotome device. Histology on mammotome cores revealed only post-core biopsy changes, indicating that the radial scar had not been sampled. On subsequent surgical excision, the radial scar exhibited foci of ALH.
Surgical excision
Eight patients (cases 15–22) with non-atypical radial scars on needle core biopsy were planned for diagnostic surgical excision. One patient (case 22) declined surgery and has demonstrated stable mammographic appearances in keeping with benign disease after 4 years follow-up. Of the seven cases that went to surgery, only one (case 21) subsequently proved malignant. This case was unique in showing malignant imaging features. The mammogram revealed a spiculate mass, and the ultrasound scan a 6 mm malignant-looking lesion. The MDT recommendation was to proceed directly to diagnostic surgical excision because of the radiological–pathological discordance. Excision histology showed 8 mm of intermediate nuclear-grade solid and cribiform ductal carcinoma in situ (DCIS) arising within a radial scar. Final histology from the other six surgical specimens confirmed a radial scar with no features of atypia or malignancy.
Discussion
Breast screening aims to reduce deaths from breast cancer through early detection and management while avoiding unnecessary interventions for benign disease in asymptomatic women.12 Large-volume mammotome biopsy is a relatively new technique that permits additional non-operative sampling of benign but potentially heterogeneous lesions, which have a known but low risk of associated malignancy. We have previously demonstrated the usefulness of this approach in the management of benign screen-detected papillary lesions.13 Here we demonstrate how mammotome excision can facilitate a more conservative approach in the management of non-atypical radial scars.
A number of recent studies have suggested that excision may not always be necessary after a core biopsy diagnosis of radial scar. Brenner et al reviewed 157 patients with core biopsy-diagnosed radial scars undergoing either surgical excision or mammographic surveillance and reported malignancy at excision in 8% of cases.14 In biopsy samples with associated atypia on the core, the risk of malignancy was 28%, but in samples without atypia the risk was only 4%. However, no malignant lesions were missed if 12 or more cores were taken or if the lesions were biopsied using a directional vacuum-assisted device. Two other groups reported that 44%15 and 37%16 of radial scars with atypia on core biopsy harboured malignancy, while the rate in both series after biopsies without atypia was only 6%. In our series, 11 of 14 (78%) patients with non-atypical radial scars had concordant benign histology after mammotome excision and thus avoided surgery. No patients managed in this way have subsequently developed malignancy, with a mean mammographic follow-up of 23 months.
An inherent limitation of core biopsy sampling is the potential for missing a malignant or atypical component to a radial scar. Farshid and Rush found that foci of malignant change within radial scars were often small and could comprise as little as 5% of the lesion.17 In addition, atypical hyperplasia and malignancy, while usually confined to the lesion, are thought to occur most often at the periphery.5 In our series, carcinoma (DCIS) was found at excision in only one of 22 (4.5%) radial scars with no atypia on initial sampling. The DCIS in this case was found peripherally and was not sampled on the initial needle core biopsy. This case was exceptional in that there was significant radiological–pathological discordance with malignant imaging features, and the MDT recommendation was therefore to proceed directly to surgical excision. Our selective approach to surgery is supported by Tennant et al, who recently reported their experience of vacuum-assisted excision in the management of lesions of uncertain malignant potential. Reassuringly, none of their 18 patients with non-atypical radial scars managed in this way subsequently developed malignancy.18
In our series, two of the 22 (9%) patients who had non-atypical histology on needle core biopsy exhibited foci of ALH within the radial scar on final excision histology. Both these patients had mammographic lesions in excess of 10 mm, which is interesting given previous reports that malignancy and atypical hyperplasia are more common in lesions >6–7 mm in maximum dimension.5 In this context, however, it is also relevant that there is still debate over the optimum management of LN detected on needle core biopsy. Recent reports suggest that the risk of concurrent invasive malignancy may be as low as 4% if cases where there is radiological–pathological discordance are excluded.19 Excision of LN may not always be necessary,20 although the implications of LN within radial scars are even less clear.
Selection of patients for mammotome excision over surgery depends critically on the absence of atypia on needle core biopsy. Histological assessment may prove problematic given the known interobserver variability in diagnosis of atypical epithelial proliferations. Immunohistochemistry for CK5/6 and oestrogen receptor may be of value in distinguishing between epithelial hyperplasia of usual type and atypia, especially when assessing the limited tissue samples obtained in needle core and vacuum-assisted biopsies.21 Immunohistochemistry for E-cadherin may highlight small foci of LN22 and may also help distinguish LN from areas of artefactual dyscohesion. Previous studies have shown the usefulness of the myoepithelial markers CK14 and p63 in papillary lesions,23 and these markers can also be helpful in highlighting the background architecture of a radial scar. Pathologists should be aware of the usefulness of these immunohistochemical markers and how they may assist in minimising potentially unnecessary surgical intervention in patients with screen-detected abnormalities.
In conclusion, selection of patients suitable for mammotome excision requires careful histological evaluation and thorough MDT discussion to ensure radiological–pathological correlation. Utilisation of mammotome excision in the management of non-atypical radial scars has significantly reduced the need for diagnostic surgery in the asymptomatic screening population.
Take-home messages
In the absence of atypia on needle core biopsy, the risk of malignancy associated with radial scars is low.
Selection of cases suitable for mammotome excision requires careful histological evaluation and thorough multidisciplinary team discussion to ensure radiological–pathological concordance.
Mammotome excision enables a more conservative approach in the management of non-atypical radial scars in the asymptomatic screening population.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.