Article Text

Abstract
Objectives To evaluate the protein expression of connexin 43 (Cx43) in primary urothelial bladder cancer and test its association with the histopathological characteristics and clinical outcome.
Methods A tissue microarray containing 348 tissue samples from 174 patients with primary urothelial carcinomas of the bladder was immunohistochemically stained for Cx43. The intensity of staining was semiquantitatively evaluated (score 0, 1+, 2+), and the association with clinicopathological features was assessed. Univariable and multivariable analyses were performed to identify predictors for progression-free survival (PFS).
Results Membranous Cx43 immunoreactivity was detected in 118 (67.8%) of 174 analysable urothelial carcinomas, of which 31 (17.8%) showed even a strong (score 2+) and mainly homogeneous staining. Strong expression levels of Cx43 (score 2+) were associated with higher tumour grade, multiplicity and increased proliferation (all p<0.05). In the subgroup of patients with stage pTa and pT1 bladder tumours (n=158), strong Cx43 expression (p<0.001), solid growth pattern (p<0.001) and increased Ki-67 proliferation fraction (p<0.05) were significantly associated with shorter PFS in an univariable Cox regression analysis. In multivariable Cox regression models, Cx43 immunoreactivity and histological growth pattern remained highly significant and adverse risk factors for PFS.
Conclusions The expression levels of Cx43 are frequent in non-muscle invasive bladder cancer (NMIBC), with high expression levels being associated with poor prognosis. Routine assessment of Cx43 expression may improve the identification of high-risk NMIBC.
- TUMOUR MARKERS
- URINARY TRACT TUMOURS
- BLADDER
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Despite improvements in diagnosis and management of urothelial bladder cancer (BC), the risk of tumour progression and recurrence remains a relevant problem. Patients with primary BC initially present mostly with non-muscle invasive bladder cancer (NMIBC) with either papillary non-invasive (pTa) or early invasive (pT1) urothelial carcinoma (70–80%), whereas the remaining 20–25% of primary tumours are already muscle invasive (≥pT2) at first diagnosis.1 ,2 Among NMIBC, almost 70% recur after initial transurethral resection and up to 25% show progression into muscle-invasive disease.3 Currently, the risk of recurrence and progression is assessed by clinicopathological factors.4 However, clinical and pathological parameters cannot accurately predict individual disease courses. Therefore, patients still need to be closely monitored to detect tumour recurrence and progression, leading to high healthcare costs of this disease.5 Markers that can diagnose NMIBC with a high risk of progression are needed for better and more specific surveillance strategies.6 Despite decades of research for biomarkers that allow a valid prediction of NMIBC progression,7–10 none are routinely used in clinical practice.
Cell migration is a fundamental process and is essential for many physiological functions of the organism. In addition, cell migration has an active role in pathophysiological processes such as tumour growth and the ability to metastasise.11 ,12 Several proteins are involved in cell migration or its modulation; these include connexins (Cxs), which are considered to compose gap junctions to form intercellular channels.13 ,14 The channels composed by Cxs serve as selective gates for the transport of small molecules such as growth factors, second messenger molecules or ions between cells.15 Cxs are therefore essential for cell homoeostasis and play an important role in the regulation of proliferation, cell growth and apoptosis.16 ,17 Cxs comprises a family of more than 20 proteins. One of the most studied Cx proteins is Cx 43 (Cx43).18 ,19 Cx43 is expressed in most epithelial tissues. Previous studies showed reduced Cx43 expression in cancerogenesis and therefore Cx43 was initially thought to have only a tumour suppressor role.20–22 However, there is growing evidence that Cx43 is involved in cancer development and metastatic processes and overexpressed in invasive lesions of some solid tumours such as breast or colon cancer.23–25
A broad expression analysis of Cx43 in urothelial carcinomas has not been conducted so far and there are no studies available on the prognostic relevance of Cx43 in BC. We aimed to analyse the expression patterns of Cx43 in a fairly large cohort of primary BCs and correlated these to clinicopathological parameters including tumour stage, grade, multifocality, adjacent carcinoma in situ, growth pattern and finally, disease course.
Methods
BC tissue microarray
Tissue microarrays (TMAs) contained 348 formalin-fixed, paraffin-embedded urothelial BC tissues from 174 patients and were constructed as previously described.26 All tumour samples were represented in duplicate tissue cores (diameter 1 mm). Specimens were collected between 1990 and 2006 by the Institute of Surgical Pathology, University Hospital Zurich, Switzerland. TMA includes a series of 174 consecutive (non-selected) primary urothelial bladder tumours. Finally, TMA contained 90 pTa, 68 pT1 and 16≥pT2 tumours. H&E-stained slides of all specimens were re-evaluated by a board-certified pathologist (PJW). Tumour stage and grade were assigned according to Union for International Cancer Control (UICC) and WHO criteria.
Retrospective clinical follow-up data were available for all the 174 patients (100%). The median follow-up period for the entire cohort was 110.6 months (range 32.4–266.8 months). Adjuvant bladder installation therapy (BCG or chemotherapy) could not be evaluated properly due to missing data in about 50% of the patients. Clinicopathological data are summarised in table 1. TMA and associated clinicopathological data have been previously published.27
Patient and tumour characteristics and results of molecular and immunohistochemical analyses
Immunohistochemistry
TMA was freshly cut and was used on 3 µm paraffin sections, as described previously.28 Additionally, to analyse the immunoreactivity of Cx43 in non-dysplastic urothelium, eight slides were cut from formalin-fixed, paraffin-embedded urothelium of the bladder neck of patients without any history of urothelial dysplasia or BC. For immunohistochemical detection of Cx43 on tissue samples, antihuman Cx43 antibody from Sigma (C6219, dilution 1:200) was used. Ki-67 was detected with clone Molecular Immunology Borstel-1 (MIB-1) (dilution 1:50; Dako, Glostrup, Denmark).
Immunohistochemical studies used an avidin-biotin peroxidase method with a diaminobenzidine chromatogen. After antigen retrieval (microwave oven for 30 min at 250 W), immunohistochemistry was conducted using an autostainer (Ventana, Tucson, Arizona, USA) following the manufacturer's instructions.
Evaluation of immunohistochemistry
Slides were evaluated by two experienced pathologists (LB, PJW). Immunoreactions for Cx43 were evaluated using a semiquantitative three-scale scoring system by considering scores 0–2+, in which score 0: no staining; score 1+: weak staining; score 2+: strong staining. For statistical analysis, cases exhibiting a score of 0 or 1+ were pooled in a Cx43 low-expression group, whereas cases with a score of 2+ were categorised in a Cx43 high-expression group. The percentage of Ki-67 positive cells of each specimen was determined as described previously.29 High Ki-67 labelling index was defined as more than 10% of positive tumour cells.30 If different staining intensity was observed between the duplicate tissue cores, the core with more representative tumour tissue was chosen. If both duplicate cores showed equal amounts of representative tumour tissue, the intensity of the core with more homogenous staining intensity was selected.
Statistical analysis
Statistical analyses were performed with the survival package in R V.3.0.3 (http://www.r-project.org) and SPSS V.22.0 (SPSS, Chicago, Illinois, USA). Differences were considered statistically significant if p<0.05. To study statistical associations between clinicopathological and immunohistochemical data, contingency table analysis and two-sided Fisher’s exact tests were used. Univariable and multivariable Cox regression analyses were used to evaluate statistical association between clinicopathological/immunohistochemical data and progression-free survival (PFS) and recurrence-free survival (RFS). The assumptions of proportional hazards were satisfied in the Cox regression model and were graphically assessed by looking at the log-minus-log plot. All variables in the multivariable model were added in one single step (enter method). Harrel's concordance index (c-index) was calculated to assess predictive accuracy.
PFS and RFS curves were calculated using the Kaplan-Meier method with significance evaluated by two-sided log-rank statistics and were plotted with pointwise bands at a confidence level of 0.95. For the analysis of PFS in NMIBC, patients were censored at the date when there was a stage-shift (from pTa to pT1–T4 or from pT1 to pT2–T4), or if a distant metastasis was detected. Grade progression (low grade (or G1–2) to high grade (G3)) without stage-shift was not considered as progression. For the analysis of RFS, patients were censored at the date when there was a recurrent and histologically proven tumour in the bladder. Any positive resection or another transurethral resection of the bladder (TUR-B) within 3 months after primary TUR-B was not considered as recurrence but residual tumour.
Results
Staining patterns of Cx43
Cx43 protein expression in BC tissue samples was investigated by immunohistochemical analysis of TMA containing 174 specimens from patients with primary urothelial carcinoma of the bladder. All 174 (100%) patients could be evaluated for Cx43 immunostaining.
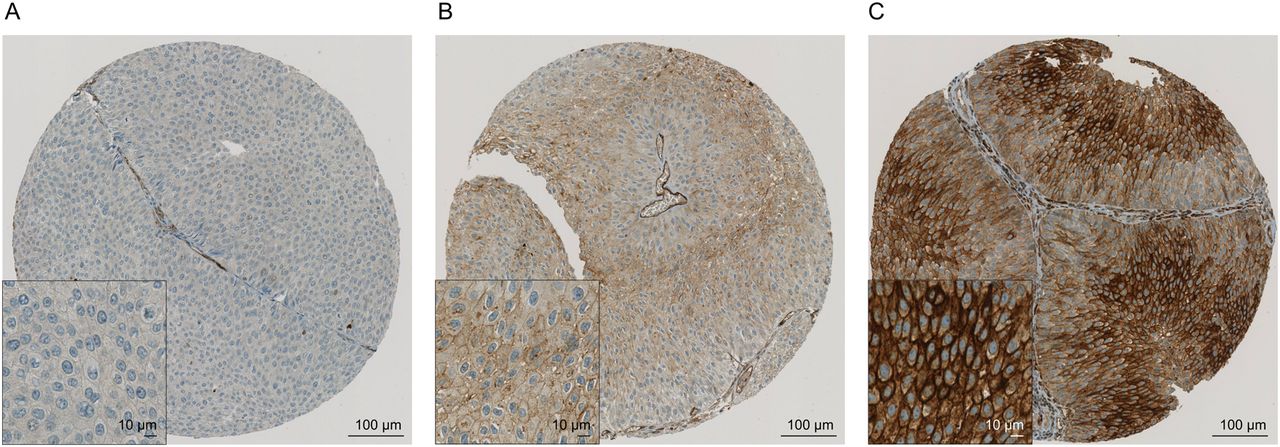
Cx43 immunoreactivity mainly showed a homogeneous membranous staining in 170 of 348 TMA spots (48.9%). A relatively small proportion of the investigated tumours showed Cx43 immunoreactivity only in the intermediate and upper layers (n=52, 14.9%), whereas a few cases were found to have Cx43 expression only in the basal layer (n=9, 2.6%). Figure 1A represents a tumour tissue example of Cx43 negative staining (score 0). Figure 1B shows an example of weak Cx43 staining (score 1+), whereas figure 1C depicts a typical example of strong Cx43 staining (score 2+) in the plasma membrane of the tumour cells.

Immunohistochemical staining with Cx43: An example of negative staining Score 0 (A) and weak (score 1+) staining pattern (B) of the Cx43 protein; Strong staining (score 2+) pattern (C) of Cx43.
Strong expression levels of Cx43 (score 2+) were found in 31 of 174 patients (17.8%). Eighty-seven (50%) of the other tumours showed weak expression levels (score 1+) of Cx43, and 56 (32.2%) were found to have no staining (score 0) for Cx43. All other clinicopathological data are summarised in table 1.
In non-dysplastic urothelium of the bladder neck of individuals without any previous history of bladder dysplasia or cancer, seven out of eight samples showed a weak but consistent Cx43 protein expression in the basal and intermediate layers (see online supplementary figure S1A–F) as well as in Brunn's nests (see online supplementary figure S1G). Another single sample showed a strong Cx43 staining intensity (see online supplementary figure S1H). Urothelial umbrella cells at the surface were negative for Cx43 in all normal cases.
Correlation of Cx43 expression with clinicopathological parameters
Cx43 was correlated with clinicopathological characteristics (stage, grade, adjacent carcinoma in situ, multiplicity, growth pattern and Ki-67) of the tumours (table 2). Strong staining of Cx43 was associated with higher grade49 (p=0.026) and multiplicity (p=0.004). Moreover, strong staining of Cx43 was significantly associated with high Ki-67 labelling index (p=0.014). High Ki-67 labelling index showed a significant correlation with all clinicopathological characteristics (p<0.05), except for tumour multiplicity (data not shown). Results of clinicopathological and Ki-67 label index of this TMA have been previously published.27
Comparison of the molecular and immunohistochemical markers with pathological characteristics (n=174)
Prognostic potential of Cx43 in primary pTa and pT1 urothelial tumours
A total of 158 patients underwent TUR for a primary pTa or pT1 urothelial carcinoma of the bladder and were followed for a median of 110.7 months (range: 32.4–245.9 months). From the 158 NMIBC cases, 22 (13.9%) cases showed progression (median time to progression was 45.2 months (range 10.2–226.7 months)), and 26 (16.5%) patients died during follow-up. In this group, high expression levels (score 2+) of Cx43 were significantly associated with increased risk of progression (p<0.001). Aside from the growth pattern (p<0.001) and Ki-67 (p=0.003), none of the other clinicopathological parameters were significantly associated with PFS. Table 3 shows p values for the pathological data and the molecular markers.
Analysis of factors for tumour progression
We performed univariable and multivariable Cox regression analyses. In univariate analysis, strong Cx43 expression (p<0.001), solid growth pattern (p<0.001) and Ki-67 (p=0.006) were significantly associated with reduced PFS. Additionally, grading49 showed a trend for reduced PFS (p=0.09). All four variables were included in a multivariable Cox regression analysis. Strong staining of Cx43 (p<0.001; HR 7.754 (95% CI 2.763 to 21.76)) and solid growth pattern (p<0.001; HR 13.377 (95% CI 3.314 to 53.99)) remained independent predictors for shorter PFS (table 4). Kaplan-Meier analyses for PFS and RFS depicted in figures 2A, B, respectively, show that patients with strong Cx43 immunoreactivity have a significantly shorter PFS and RFS than patients with weak or negative staining for Cx43. The clinical benefit was moreover confirmed by analysing the C-index in the multivariable Cox regression model. The C-index was higher using the multivariable model with Cx43 than without (C-index with Cx43: 0.813; C-index without Cx43: 0.723).
Univariable and multivariable Cox regression analyses for tumour progression

{kind=link}
{kind=link}
Kaplan-Meier analyses for progression-free survival (A) and for recurrence-free survival (B) for Cx43 staining (n=158). For statistical analysis for survival curves log-rank test was used. Pointwise bands at a confidence level of 0.95 were computed. N-values represent the number of patients in each group.
In a descriptive subgroup analysis for patients with pT1 high grade tumours (n=40) strong Cx43 expression (p=0.024) was significantly associated with reduced PFS (see online supplementary figure S2A). Strong Cx43 immunoreactivity (p=0.257) was not associated with shorter RFS in this subgroup analysis (see online supplementary figure S2B).
Discussion
This is the first study analysing immunohistochemical Cx43 expression in primary BC and its association with prognosis. In our study, we found that Cx43 was highly expressed in 31 out of 174 investigated urothelial tumours. Strong Cx43 staining was associated with higher grade, multifocal tumours and increased Ki-67 labelling index. Furthermore, high expression levels of Cx43 were found to be an independent predictor of PFS in NMIBC. Our findings suggest that Cx43 may play a role in the prognosis of patients with non-muscle invasive urothelial tumours.
So far, only two studies have investigated the role of Cx26 in BC and both have found an overexpression of Cx26 in human BC and an association with adverse pathological features.31 ,32 Another study, by Corteggio et al,33 examined the expression levels of Cx43 in bovine urothelium and bovine urothelial cancer. The authors found that Cx43 was expressed in normal urothelium, papillary neoplasms and carcinoma in situ, but not in invasive urothelial cancer. In addition, Cx43 has been found to be altered in the detrusor muscle of the bladder in patients with overactive bladder syndrome or interstitial cystitis.34 ,35
Cx43 expression is upregulated in various other tumour entities, including glioma, colon cancer and invasive breast cancer.24 ,36 ,37 In contrast, several studies have reported the downregulation of Cx43 in solid tumours; for example, in ovarian cancer, non-melanotic skin tumours and lung cancer.38–40
The role of Cxs in tumours and in cancer progression seems to be controversial. This may be due to cellular heterogeneity of the analysed tumours and the complex multilevel process of tumorigenesis and progression. However, more reports suggest that Cx43 is overexpressed in some solid tumours and is involved in late metastatic steps. This could be demonstrated for breast cancer, melanoma and oral squamous cell carcinoma.25 ,41 ,42
As previously published, increased proliferation as assessed by Ki-67 was highly associated with tumour grade, stage and shorter PFS in this cohort.27 The prognostic role of Ki-67 in urothelial cancer and its association with pathological parameters and prognosis has already been shown in several studies.43 ,44 Here, we observed a significant correlation between the proliferation index (Ki-67) and Cx43 (p=0.014).
As the proportion of muscle-invasive BC samples was limited, we cannot draw any conclusions for this group of tumours. The prognostic role in locally advanced invasive BC has to be evaluated in further studies with higher sample sizes.
Our results demonstrate the potential diagnostic value of Cx43 for the assessment of progressive primary NMIBC. Our findings suggest that the overexpression of Cx43 in BC facilitates tumour cell survival and progression by enhanced gap junction activity, which has previously been shown to induce tumour growth and tumour cell survival.45–47 In addition to its prognostic significance, specific pharmaceutical or genetic approaches to inhibit Cx43 activity may provide ways to reduce progression in NMIBC.
Conclusion
Positive immunoreactivity of Cx43 is frequently observed in BC and showed a significant correlation with different clinicopathological variables in BC.
High expression levels of Cx43 were associated with poor prognosis in NMIBC. Routine assessment of Cx43 expression may improve the identification of high-risk NMIBC. Further prospective studies and larger cohorts are needed to confirm the prognostic impact of Cx43 in BC.
Take home messages
Besides clinicopathological parameters no biomarkers are established to assess prognosis in primary bladder cancer (BC).
Connexin 43 (Cx43) has been proposed to be involved in cancer development in solid tumours such as breast cancer or colon cancer.
This is the first study demonstrating the prognostic value of immunohistochemical Cx43 expression in primary non-muscle invasive BC.
Strong Cx43 protein expression was associated with worse clinicopathological features and was furthermore an independent risk factor for shorter progression-free survival.
Routine assessment of Cx43 expression may improve the identification of high-risk non-muscle invasive BC.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figures
Abstract in Deutsch
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Abstract in Deutsch - Online abstract
Footnotes
CP and LB contributed equally.
Handling editor Cheok Soon Lee
Contributors Conception and design: CP, LB, PJW. Provision of study materials or patients: CP, TH, AH, JR, LB, HM. Collection and assembly of data: AH, DM, CP. Data analysis/interpretation: CP, LB, FR, MD, PJW, TS, QZ. Manuscript writing: CP, LB, PJW. Final approval of manuscript: CP, LB, FR, MD, TH, DM, AH, JR, QZ, TS, HM, PJW.
Competing interests None declared.
Ethics approval Cantonal Scientific Ethics Committee Zurich (http://www.kek.zh.ch/, approval no.: StV-Nr. 25/2007).
Provenance and peer review Not commissioned; externally peer reviewed.