Article Text

Abstract
Background Testing for BRAF mutations in colorectal carcinoma (CRC) is important in the screening pathway for Lynch syndrome and is of prognostic value to guide management. This is a diagnostic accuracy study of the Idylla system, a novel and automated alternative PCR system.
Methods 100 consecutive formalin-fixed, paraffin-embedded CRC resection cases were tested for BRAF mutations using the Idylla automated platform and compared with standard (Cobas) PCR.
Results The sensitivity of the Idylla BRAF test was 100% and the specificity was 96%. Only one discordant Idylla positive/standard PCR negative result occurred and on Droplet Digital PCR demonstrated a mutation not identified by traditional PCR in this case.
Conclusion This study has validated the Idylla system for BRAF testing in CRC and demonstrated a possibly greater sensitivity, in addition to cost effectiveness and shorter turnaround time, when compared with standard PCR.
- COLORECTAL CANCER
- diagnostic screening
- SURGICAL PATHOLOGY
Statistics from Altmetric.com
Introduction
BRAF is a serine/threonine kinase member of the RAS/RAF/MAPK pathway encoded by the proto-oncogene BRAF. Mutations in BRAF have been identified in numerous cancers, such as melanoma, papillary thyroid carcinoma, and some lymphomas.1 BRAF mutations are also detected in around 15% of colorectal carcinoma (CRC) resection specimens and while V600E (c.1799T>A) is the most common lesion, mutations in the E2, D, K, M and R codons have all been shown to be clinically relevant.2 ,3
While most cases of CRC are sporadic, around 5% of cases occur in patients with Lynch syndrome (LS)4 and screening of tumour resection tissue for LS is now endorsed by the Royal College of Pathologists5 and others.4 ,6 ,7 For those patients meeting the revised Bethesda criteria for screening for LS (box 1), this approach uses immunohistochemistry (IHC) for mismatch repair (MMR) proteins and also incorporates BRAF mutation testing (figure 1).2 ,4–7 IHC for the MLH1 MMR protein has low specificity but this is improved by incorporating BRAF analysis.4 BRAF mutations are rare in non-sporadic tumours and thus identifying a mutation virtually excludes LS.2 Furthermore, some authors have suggested testing for BRAF mutations alone in LS screening in those patients meeting the revised Bethesda criteria.8 BRAF testing is also recommended in stage II or greater CRC as a prognostic marker to guide management.9 Therefore, BRAF testing is increasingly becoming routine for many patients with CRC in the UK.
The latest revised Bethesda guidelines for immunohistochemical microsatellite instability screening
Revised Bethesda criteria:
CRC diagnosed at younger than 50 years
Presence of synchronous or metachronous CRC or other LS-associated tumours
CRC with MSI-high pathologic-associated features (Crohn-like lymphocytic reaction, mucinous/signet cell differentiation, or medullary growth pattern) diagnosed in an individual younger than 60 years old
Patient with CRC and CRC or LS-associated tumour diagnosed in at least one first-degree relative younger than 50 years old
Patient with CRC and CRC or LS-associated tumour at any age in two first-degree or second-degree relatives
Patients meeting one or more criterion should be screened. LS-associated tumours include colon, rectum, stomach, ovary, endometrium, pancreas, uterus, kidney, biliary tract, brain, small bowel and some skin tumours.3 ,4
CRC, colorectal carcinoma; LS, Lynch syndrome; MSI, microsatellite instability.

Flow chart demonstrating the current recommended screening pathway for Lynch syndrome (LS) using mismatch repair immunohistochemistry (IHC) (MLH1, PMS2, MSH2, MSH6 antibodies) and BRAF testing, adapted from the consensus statement by the US Multi-Society Task Force on Colorectal Cancer.4
Current modalities for BRAF testing include PCR and gene-sequencing panels. These require specialist facilities and staff, are costly and have a long turnaround time.6 ,7 ,10 The Idylla system (Biocartis) is a relatively inexpensive, compact, automated real-time PCR unit, with an on-demand turnaround time of around 60–120 min for multiplex mutation assays which is suitable for use by staff who are not trained in molecular biological techniques. The system is a compact standalone unit which can be placed in any histopathology laboratory (see figure 2) and comprises a computer console and up to four processing units. The cost per test is variable and based on the caseload, but is competitive with other standard assays currently available. Tissue preparation (section cutting) adds no additional burden beyond that of standard PCR.11

The Idylla system in situ with computer console 50×35×25 cm (above) and one tissue processing unit 30×45×20 cm (below).
The Idylla technology is cartridge based (see figure 3) and uses microfluidics processing with all reagents on board. The cartridges require a user to put in macro-dissected tissue and the remaining process, including nucleic acid extraction, is fully automated. Tissue is homogenised and cells lysed using a combination of heat, high-frequency ultrasound and enzymatic/chemical digestion. Extraction and purification is carried out using a silica-based compound. The PCR is real time and uses a fluorophore-based detection system. The post-PCR curve analysis is automated on board the console and the results are presented on screen as either ‘No mutation detected’ or ‘BRAF mutation detected’.11

The Idylla BRAF Mutation Test cartridge (95×70×40 mm).
Unlike standard PCR systems, which usually only assay the V600E codon,12 the Idylla BRAF Idylla BRAF Mutation Test cartridge covers the full range (E, E2, D, K, M and R)13 of clinically relevant and actionable V600 mutations in CRC.2 ,13 While the Idylla system was originally launched with the Idylla BRAF Mutation Test for use in melanoma,11 ,13–15 KRAS has just been launched for CRC and the authors understand that a number of other clinically relevant single and multigene assay cartridges (including NRAS) are in development.11
The published literature on the Idylla platform is currently limited to small technical validation studies on highly selected cases.14–16 The aim of this study was to clinically validate the Idylla system for the detection of BRAF mutations in patients with colorectal adenocarcinoma for whom BRAF testing by PCR is carried out as standard care. This includes LS screening for patients meeting the revised Bethesda criteria and for prognostication in patients with stage II (pT3N0 and pT4N0) or above CRC. The reference standard which the Idylla (index test) was compared against is a commonly used standard-care test, the Cobas 4800 BRAF V600 Mutation Test performed on the Cobas 4800 System (Roche Molecular Diagnostics),12 which has been previously validated on CRC tissue and is now in widespread use.17 This assay largely detects the V600E mutation, with limited D or K mutation coverage.12
Methods
Consecutive clinical cases that had undergone BRAF testing at the John Radcliffe Hospital, Oxford over a 6-month period between 2013 and 2014 were identified. Inclusion criteria were adult colorectal adenocarcinoma cases with known BRAF mutation status that had been tested for prognostication or for LS screening. Referral cases and cases with no remaining tissue were excluded. Anonymised tissue from the same paraffin block that was BRAF mutation tested was obtained with full ethical approval from the National Research and Ethics Service (Oxfordshire Research and Ethics Committee A; reference 04/Q1604/21) from all cases meeting the inclusion criteria.
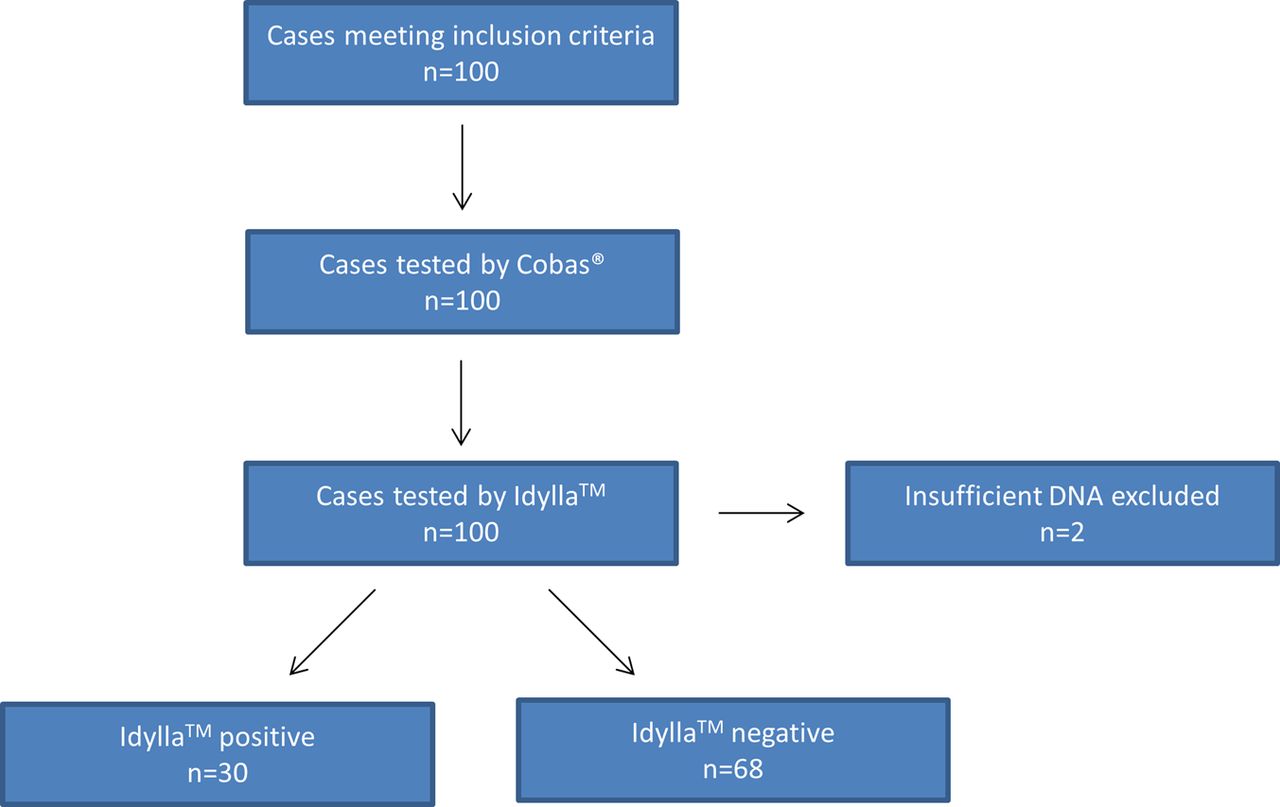
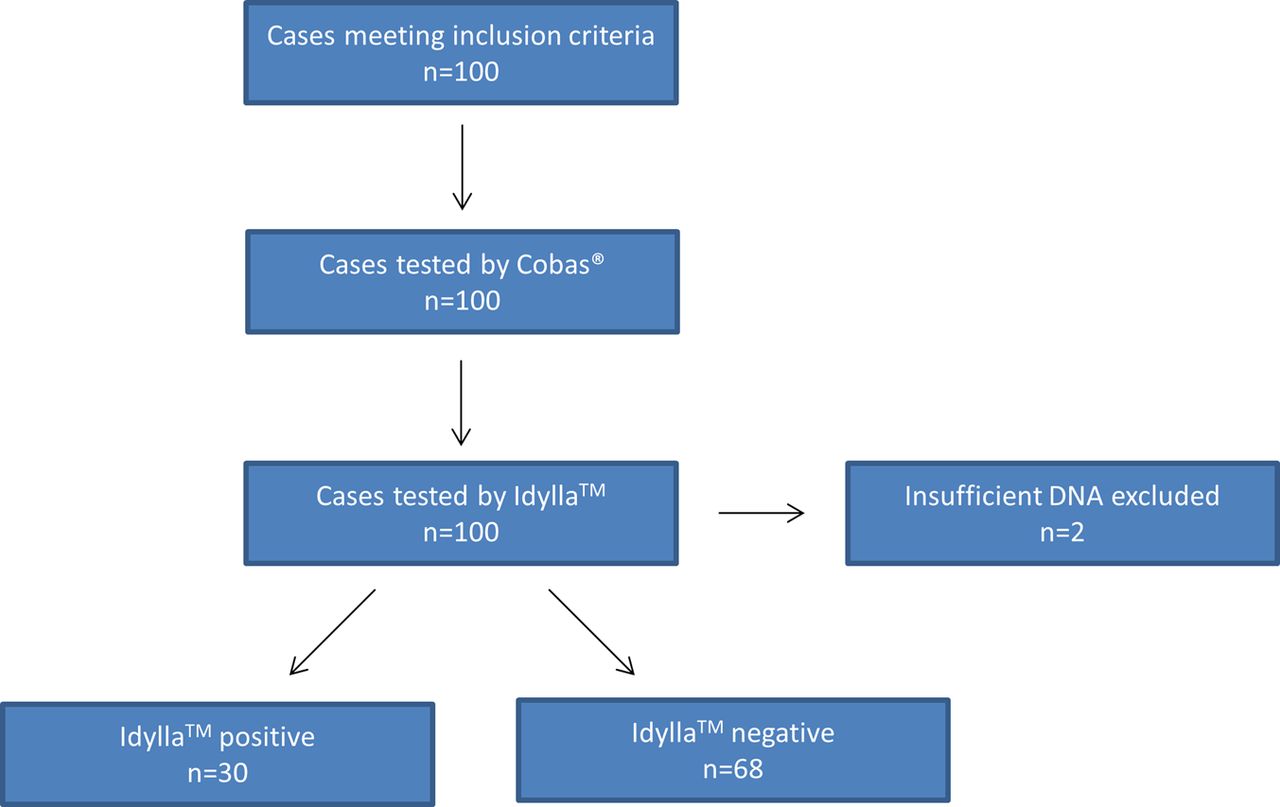
BRAF mutational status had been determined retrospectively by PCR using the Cobas 4800 system12 at the time of the original report by our molecular diagnostics unit. There was one individual (RC) carrying out the index test and tissue was cut by an independent, blinded laboratory. All study participants were blinded to the original Cobas result until after Idylla gave a definitive result. For each case one unstained 5 µm formalin-fixed, paraffin-embedded (FFPE) tissue section was cut and placed on a glass slide. Water baths and blades were cleaned between cases. The original H&E sections were examined and an appropriate tissue area (50–600 mm2, ≥10% tumour cells) for testing was macro-dissected from the unstained sections. Tissue was processed using the Idylla BRAF Mutation Test13 cartridge and run on the Idylla system. The dissected tissue was placed between two 5 mm discs of blotting paper, wetted with nuclease-free water, and placed inside an Idylla BRAF Mutation Test cartridge.13 The cartridge was loaded onto the Idylla system for processing. The Idylla console auto-analysed the PCR curve to determine the presence or absence of a BRAF mutation. Cases were processed between April and July 2015. One (discordant) case was further assayed using the PrimePCR ddPCR Mutation Assay on the QX200 Droplet Digital PCR System (Bio-Rad Laboratories).18 A positive test was defined as a case with any mutation detected. See figure 4 for depiction of the study protocol.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow diagram depicting the study protocol design and results.
The sample size was estimated using a nomogram method19 for 95% CIs at a sensitivity and specificity near 100%, based on previous data.14 ,15 Statistical analysis for sensitivity, specificity and predictive values was carried out using standard formulae using the XLSTAT plugin for Microsoft Excel.20
Results
One hundred consecutive CRC cases from 97 patients were retrieved, representing around 70% of CRC resection workload. Ninety-six cases were resection specimens and four cases were biopsies. The average age was 72 years (range 34–94). Forty-five were men and 55 were women. All cases were invasive adenocarcinoma ranging from moderately to poorly differentiated tumours and ranging from pT1 to pT4 tumours. All cases met the minimum tissue requirements for testing and the majority of the cases contained 50–80% tumour cells in around 25 mm2 of tissue. All cases had the Idylla test and the standard PCR (see figure 4). The four biopsy cases and two of the resection cases required multiple sections to meet the tissue area requirements; the maximum number of sections used in any case was six. Two cases (both were resections) contained insufficient DNA in the tissue available to the study to produce a result, thus these were excluded. Of the 98 cases which produced a result, 30 (31%) were MLH1 negative on IHC and therefore tested for BRAF mutations within the context of LS screening. The remaining 68 cases had been tested for BRAF mutations for prognostication.
In total, 30 cases (31%) had tested positive for BRAF mutations on the Idylla system. All but one case showed agreement between the Idylla system and Cobas, making the concordance 98.97%. All 29 Cobas-positive cases tested positive with Idylla and 60 of the 61 Cobas-negative cases tested negative with Idylla. Therefore the one discordant case was Idylla positive and Cobas negative. A summary of the results is given in table 1.
Summary of the diagnostic accuracy study comparing Idylla (index test) with Cobas (reference test) PCR
The sensitivity of the Idylla system therefore was 100.0% (95% CI 85.8% to 100.0%) and the specificity was 98.6% (95% CI 91.3% to 100.0%). The positive predictive value was 96.7% (95% CI 90.2% to 100.0%) and the negative predictive value was 100% (95% CI 100.0% to 100%). The positive likelihood ratio was 69.
The discordant tissue submitted had a tumour surface area >50mm2 and was >50% tumour cells. The case was adjudicator tested by Droplet Digital PCR for BRAF which found the case to be positive for the V600E mutation, making the Idylla result a true positive and the original Cobas result a false negative. Given this, the specificity of the Idylla system could therefore be given as 100%.
Discussion
BRAF mutational status now plays a significant role both in screening for LS and prognostication in patients with CRC.4–7 ,9 Current diagnostic modalities include traditional PCR (commonly Cobas) and cancer gene panels.4–7 ,10 ,12 These approaches require expensive equipment, specialist laboratory facilities and staff, cause significant delays in tur-around times (often up to 7 days) for NHS histopathologists and many centres are forced to outsource the work (where possible), adding further costs and delays.7 ,21 Furthermore, some of these approaches do not cover the full range of actionable mutations in their assays.12
In this study we validated the Idylla system for BRAF mutations retrospectively using 100 consecutive clinical cases mimicking true clinical practice. The Idylla platform uses established real-time PCR technology but is a single test, on-demand, fully automated system with minimal sample preparation and no post-test analysis. This was compared with a traditional platform (Cobas), which requires multiple specimen preparation stages and batched processing.12 ,13 We found the Idylla system fast and easy to use. The diagnostic accuracy was high and concordance with Cobas PCR was near 100%. The one discordant (Idylla positive/Cobas negative) case was found to be a true BRAF V600E mutant via an adjudicator test, making the actual sensitivity and specificity of the Idylla system 100% and demonstrating the increased sensitivity of the Idylla system over that of the Cobas platform. Besides the obvious advantage of Idylla detecting more clinically relevant mutations (E2, M, R etc) than most standard PCR assays,13 with this finding we have highlighted the potential for Cobas to miss even the common V600E lesions.
We experienced only seven failed tests. This included three failures due to a machine error because the unit was faulty (it was quickly replaced and no further errors were encountered) and two failures due to user error. Only one cartridge failed under normal working conditions (true failure rate 1%). Two tests were reported as insufficient material and these were paucicellular (<10% tumour cells) mucinous tumours which, had further tissue sections been available (which would have been the case in clinical practice, however this was limited in the study by funding), could have been tested with multiple tissue sections.
The cost of sending our cases for BRAF PCR by the Cobas system is around £180 (including section cutting) at our institution,21 which is significantly higher than the cost of a test on the Idylla platform. Furthermore, the potentially increased sensitivity and larger range of mutation loci covered by the Idylla system is likely to reduce LS-screened referrals and reduce institutional expenditure further. Indeed, the one discordant case was MLH1 negative on IHC, but with a BRAF mutation this represents a likely sporadic tumour2 ,4 and would have therefore reduced the number of cases that would have required Clinical Genetics referral (costing £1340 with germline testing) from three to two.
The advantages of an on-demand, automated PCR approach over traditional methods are clear; the platform offers a competitive alternative to traditional PCR at a reduced cost and much reduced turnaround time. Where this technology can fit into the market deserves some further consideration however. Currently, while most large centres are still using traditional PCR approaches for BRAF and other single gene mutations, gene panels will become increasingly popular as the cost of Next Generation Sequencing (NGS) falls.7 ,10 Such NGS gene panels, however, are often ‘home-brew’, test a wide range of clinically irrelevant genes, are challenging to interpret, expensive, poorly validated and not CE marked for routine clinical use.22 The cartridges offered by this automated system are focused on clinically relevant and actionable mutation targets, as mentioned.2 ,11 ,13–16 The system also opens the possibility of smaller district centres, which may not have access to molecular pathology laboratories or find sending tissue away costly and laborious, the opportunity to set up their own in-house diagnostic molecular service. With current trends towards molecular diagnostics, the need for this service to provide best patient care is likely to grow.23 Specifically for CRC, the screening for LS is now increasingly recognised by many professional bodies.4 ,5 The cost effectiveness of providing such screening is also now clear.21 It has been suggested by the Royal College of Pathologists5 that IHC testing for MMR protein to be performed on all CRC specimens for LS screening and prognostication and there is an observed trend towards this direction in our institution due to the demand from the oncologists and clinical genetics department. Furthermore, emerging treatment options are providing more indications for establishing MMR status.24 Thus requests for BRAF testing are only likely to increase.
In conclusion, in this study we have clinically validated a novel automated standalone PCR technology for use in detecting BRAF mutations in FFPE CRC tissue. We found this to be a simple and potentially cost-effective technology which, in the right laboratory setting and context, would be a useful addition for diagnostic molecular pathology testing.
Take home messages
BRAF mutation detection imparts important prognostic information in patients with colorectal carcinoma (CRC) and is useful in screening for Lynch syndrome (LS).
Traditional PCR-based mutation assays have significant financial, staffing, mutation coverage and turnaround time limitations.
The Idylla platform is a robust, fast and cost-effective automated, on-demand PCR platform which has potential to play a significant future role in molecular pathology departments in the UK.
This study validates the Idylla BRAF Mutation Test for use in CRC adenocarcinoma formalin-fixed, paraffin-embedded resection tissue.
Acknowledgments
The authors would like to thank Adrian Wood, Paola Valente, Jochen Schuck, Suzanne Page and the Oxford Molecular Diagnostics Centre, and the Oxford Centre for Histopathology Research.
References
Footnotes
Handling editor Cheok Soon Lee
Contributors RC conceived the project, collected the data, analysed the results and drafted the manuscript. LMW and ES oversaw the project. All authors contributed to the final draft of the manuscript.
Funding Provided by the Oxfordshire Health Services Research Committee. The Idylla system was provided on loan from Biocartis with a sample set of cartridges.
Competing interests None declared.
Ethics approval Oxfordshire Research and Ethics Committee A.
Provenance and peer review Not commissioned; externally peer reviewed.