Article Text

Abstract
The concept of serrated colorectal neoplasia has become recognised as a key process in the development of colorectal cancer (CRC) and an important alternative pathway to malignancy compared with the long-established ‘adenoma-carcinoma’ sequence. Increasing recognition of the morphological spectrum of serrated lesions has occurred in parallel with elucidation of the distinct molecular genetic characteristics of progression from normal mucosa, via the ‘serrated pathway’, to CRC. Some of these lesions can be difficult to identify at colonoscopy. Challenges for pathologists include the requirement for accurate recognition of the forms of serrated lesions that are associated with a significant risk of malignant progression and therefore the need for widely disseminated reproducible criteria for their diagnosis. Alongside this process, pathologists and endoscopists need to formulate clear guidelines for the management of patients with these lesions, particularly with respect to the optimal follow-up intervals. This review provides practical guidance for the recognition of these lesions by pathologists, a discussion of ‘serrated adenocarcinoma’ and an insight into the distinct molecular genetic alterations that are seen in this spectrum of lesions in comparison to those that characterise the classic ‘adenoma-carcinoma’ sequence.
- COLON
- RECTUM
- COLORECTAL CANCER
Statistics from Altmetric.com
Introduction
Until relatively recently the only serrated (‘saw tooth’) colorectal lesion that many diagnostic histopathologists were aware of was the hyperplastic polyp. The term ‘serrated polyp’ was first used in 1990 by Longacre and Fernoglio-Preiser to describe a newly recognised form of colorectal polyp that showed features of a conventional adenoma and a hyperplastic polyp. This lesion subsequently became known as the ‘traditional’ serrated adenoma (TSA).1 Torlakovic and Snover later identified subtle differences between sporadically occurring hyperplastic polyps and the polyps found in the condition initially known as ‘hyperplastic polyposis’. These polyps showed a constellation of features that were distinct from both sporadic hyperplastic polyps and TSAs, and this led to the recognition of the ‘sessile serrated lesion’ (SSL).2 SSLs can of course occur sporadically as well as in the setting of polyposis. Jass later demonstrated that SSLs were associated with a distinct molecular pathway to colorectal cancer (CRC).3 Jass highlighted the biological importance of these ‘hyperplastic polyp-like’ lesions that were more commonly found within the right colon, were usually sessile and relatively large (often 10 mm or more in diameter) but that did not show features of dysplasia as seen in ‘classical’ adenomas.4
As a result of these and other studies, a spectrum of colorectal polyps exhibiting a partially or wholly serrated architecture is now recognised (table 1). Some of these lesions show no dysplasia of any recognisable form while others show ‘dysmaturation’ that is now recognised by at least some pathologists as a subtle form of dysplasia. Finally, some serrated lesions show ‘conventional’ dysplasia, as is already widely recognised by histopathologists as an integral feature of ‘classical’ colorectal adenomas. These areas of ‘conventional’ dysplasia may be low grade or high grade in nature and in the setting of serrated colorectal polyps, and are usually present within one or more areas of the polyp, combined with other areas that do not show ‘conventional’ dysplasia. This heterogeneous appearance has led to use of the term ‘mixed polyp’ by some groups.
Prevalence of the different types of serrated lesion within the colorectum (adapted from Bettington et al unless otherwise stated)5
During the process of recognition of the serrated colorectal polyp ‘spectrum’, several names have been used to describe some of these lesions and this has led to terminological confusion. The key skill for the diagnostic histopathologist is the ability to recognise that some colorectal lesions that would probably previously have been called ‘hyperplastic polyps’, with the implication that they are not associated with a significant increase in CRC risk, may in fact represent one of the forms of colorectal polyp that can progress to malignancy.
The ability of histopathologists to differentiate accurately between types of serrated lesion is most pertinent during the differentiation between SSLs and hyperplastic polyps, as SSLs are the lesions that may not show conventional dysplasia, yet are associated with an increased risk of progression to CRC.
CRC arising in association with serrated polyps most often shows histological features that are not distinguishable from those of CRC arising in association with ‘classical’ adenomas. Alternatively, it may show a range of morphological appearances that are characteristic of ‘serrated adenocarcinoma’.7 The molecular alterations occurring during progression to CRC along the ‘serrated pathway’ are distinct to those occurring within the classical ‘adenoma-carcinoma sequence’, and there is evidence that this progression occurs more quickly within the ‘serrated pathway’.5
The spectrum of serrated lesions
Hyperplastic polyp
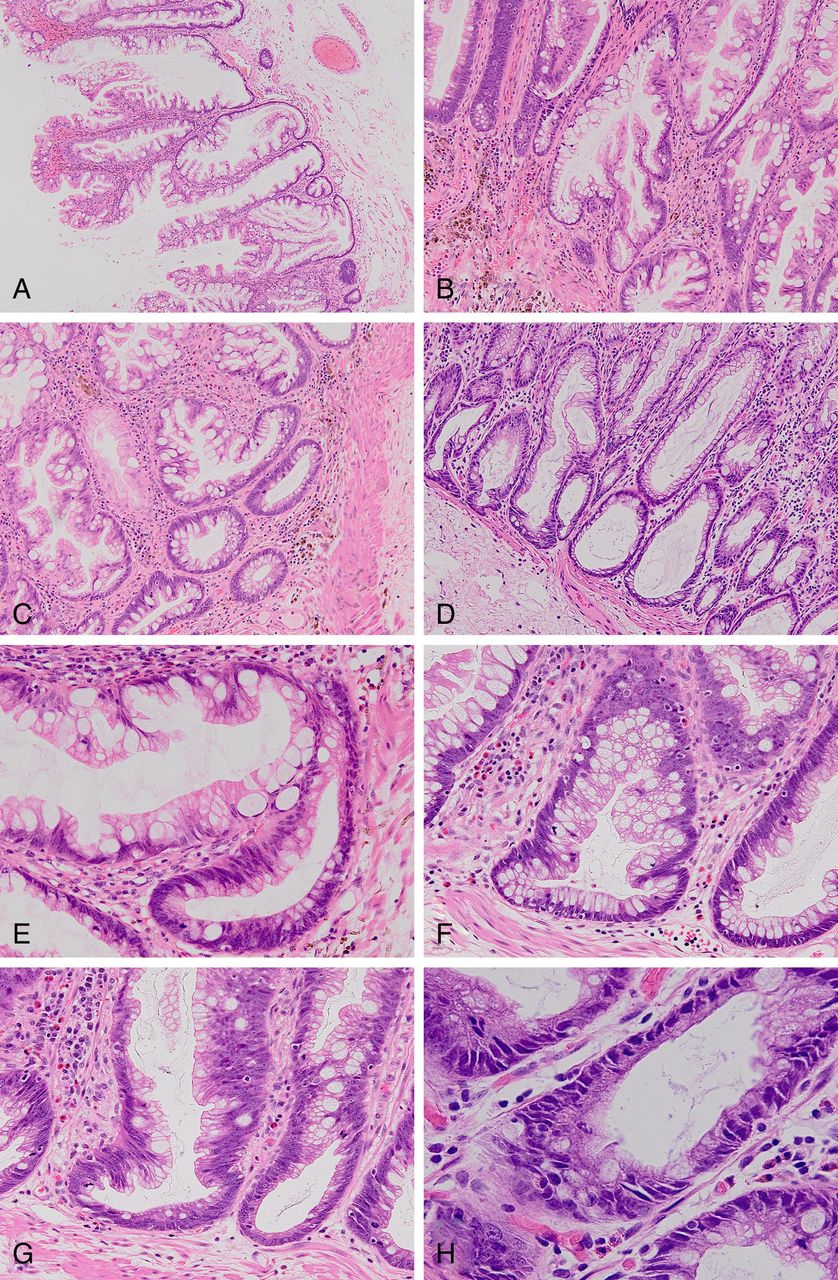
Hyperplastic polyps are very commonly encountered by all pathologists who report colorectal lesions. They occur at all sites within the large intestine—although they are most common within the distal colon and rectum—and are classically less than 10 mm in size. They share some histological features with SSLs, for example, a serrated architecture. Three morphological variants exist—microvesicular, goblet cell and mucin-poor (figure 1). Very few pathologists will use this subclassification system for hyperplastic polyps in a routine setting. Despite this, knowledge of the spectrum of appearances of hyperplastic polyps may facilitate their positive identification and therefore facilitate their differentiation from other serrated lesions, especially SSLs (table 2).
Key features of the three variants of hyperplastic polyp

The histological features of hyperplastic polyps. (a) Microvesicular variant. Magnification ×100. (b) Microvesicular variant. Magnification ×200. (c) Base of crypts to show proliferative zone. Magnification ×200. (d) Mucin-poor variant. Magnification ×400. (e) Microvesicular variant. Magnification ×400. (f) Goblet cell variant. Magnification ×100. All—H&E stain.
Hyperplastic polyps have historically not been considered as precursor lesions to CRC. However, both BRAF and KRAS mutations (see later) are common in these lesions and are likely to be important steps in their development.8
Sessile serrated lesions
SSLs (also known as ‘sessile serrated polyps’ or ‘sessile serrated adenomas’) resemble hyperplastic polyps on initial examination. Indeed, differentiation between hyperplastic polyps and SSLs can be problematic, especially with small biopsies or those showing crush, diathermy or tangential cutting artefact. SSLs are most commonly encountered in the right colon,2 although they can occur throughout the large intestine. As their name suggests, they are usually sessile in nature (itself a difficult quality to define with absolute clarity). They may be over 10 mm in diameter, although interestingly, around one-third of SSLs are 5 mm or less across.2 The characteristic histological features of SSLs are listed in box 1 (figure 2). There is some difference of opinion regarding how many of these characteristic features are required and how widespread they need to be in order to make a diagnosis of SSL. For example, the American Gastroenterology Association Guidelines suggest that when assessing a serrated lesion, the presence of a single crypt showing one of the characteristic features is sufficient in order to diagnose a SSL.9 In contrast, the World Health Organisation criteria include a statement that at least three crypts—or two adjacent crypts—must show the characteristic features for the diagnosis to be reached.10 SSLs share some histological features with the microvesicular variant of hyperplastic polyp, while BRAF mutations are common within both lesions. These features have led some to suggest that SSLs may evolve from hyperplastic polyps.8 If this is true and hyperplastic polyps are indeed part of a spectrum of serrated polyps that includes SSLs, it clearly leads to the requirement for reassessment of the relationship (if any) of hyperplastic polyps to CRC.
Key histological features of SSLs2,5
Irregular distribution of crypts
Dilatation of crypt bases
Serration present at crypt bases
Branched crypts
Horizontal extension of crypt bases*
Dysmaturation of crypts†
Herniation of crypts through muscularis mucosa
World Health Organisation criteria—at least three crypts or at least two adjacent crypts must show one or more of these features to enable a diagnosis of SSL10
American Gastroenterology Association criteria—one crypt showing the characteristic features is sufficient for the diagnosis of SSL9
*Involved crypts often have an ‘L’ or inverted ‘T’ shape.
†Dysmaturation is disordered cellular maturation within crypts and is evidenced by subtle nuclear enlargement, crowding, pseudostratification and mitotic activity together with the presence of a disorganised mixture of non-mucus-containing epithelial cells and mature goblet cells within the deep aspects of crypts.2 In this context, assessment of proliferation index, for example, using MIB-1 may provide supporting evidence for a diagnosis of SSL by highlighting epithelial cell proliferation within the superficial half of crypts. However, such immunohistochemistry, while sometimes helpful, does not reveal features that are alone diagnostic of SSL.
SSL, sessile serrated lesion.
The histological features of sessile serrated lesions (SSLs) and the key histological features of these lesions. (a) Low-power view to show pronounced serration. Magnification ×40. (b) Irregular, branched crypts. Magnification ×100. (c) Serration close to crypt bases. Magnification ×100. (d) Dilated crypts. Magnification ×100. (e) Markedly distorted crypt. Magnification ×200. (f) T-shaped crypt. Magnification ×200. (g) Boot-shaped crypt. Magnification ×200. (h) Subtle ‘dysmaturation’ within base of crypt. Magnification ×400. All—H&E stain.
There is evidence that the reproducibility of diagnosis of SSLs is poor, that is, that significant inter-observer variability exists in the differentiation of these lesions from other polyps.11 A recent single-centre study has demonstrated a large increase in the diagnosis of SSLs over a 4-year period from 2009, but also that retrospective review of right-sided lesions originally diagnosed as hyperplastic polyps resulted in re-categorisation to SSLs in 30–64%.12 It has been suggested that the presence of features of mucosal prolapse may be one of the most frequent reasons for misdiagnosis of SSLs.13 Since SSLs appear to possess greater clinical significance than hyperplastic polyps and may progress more rapidly to adenocarcinoma than ‘classical’ adenomas, accurate diagnosis is essential. In the UK, the introduction of the National Bowel Cancer Screening Programme (BCSP) has raised the awareness of all forms of colorectal polyp, including SSLs. Educational events linked to the BCSP should gradually improve the future consistency of diagnosis of these lesions among pathologists involved in the programme. There is some evidence that achieving a consensus on the diagnostic criteria for serrated lesions (including hyperplastic polyps and TSAs) between reporting pathologists can improve the consistency of diagnosis of these lesions.14
‘Pure’ SSLs do not show ‘conventional’ dysplasia, that is, dysplasia as is characteristic of ‘classical’ adenomas, although they do characteristically show ‘dysmaturation’ (box 1). However, dysplasia can develop within them—both low and high grade. The natural history of SSLs with and without ‘conventional’ dysplasia is not fully defined. However, it is believed that the development of ‘conventional’ dysplasia is indicative of a high risk of progression to CRC and that malignancy may supervene more rapidly than with ‘classical’ adenomas.5 ,15 The term ‘mixed polyps’ has been used to describe SSLs that include an area of ‘conventional’ dysplasia. However, this term may not be ideal as it could be interpreted as implying that these lesions develop de novo as a combination of SSL and ‘conventional’ dysplasia rather than following the occurrence of ‘conventional’ dysplasia within a pre-existing SSL that originally developed without ‘conventional’ dysplasia. The alternative term ‘sessile serrated adenoma’ has been suggested to describe SSLs with (or sometimes, indeed, without) ‘conventional’ dysplasia. The use of this term is understandable as the areas of ‘conventional’ dysplasia in these lesions frequently possess a serrated morphology, even when it is high grade in nature.15 However, at present, the phrase ‘sessile serrated adenoma’ is used more commonly in North America than in the UK.
‘Conventional’ dysplasia is recognisable when it occurs in SSLs using the same criteria for its recognition in ‘classical’ adenomas. However, loss of the DNA mismatch repair enzymes hMLH-1 and hMSH-2 is commonly seen in ‘conventional’ dysplasia arising in SSLs, and therefore demonstration of loss of expression of these proteins using immunohistochemistry may be useful to confirm the presence of dysplasia occurring in this setting.16 However, since loss of DNA mismatch repair enzyme expression occurs in these lesions due to inactivation of the gene promoter sequence, demonstration of loss of expression of these proteins in this context does not imply that the patient has Lynch syndrome, that is, a germline mutation in the corresponding gene (figure 3) (see later).
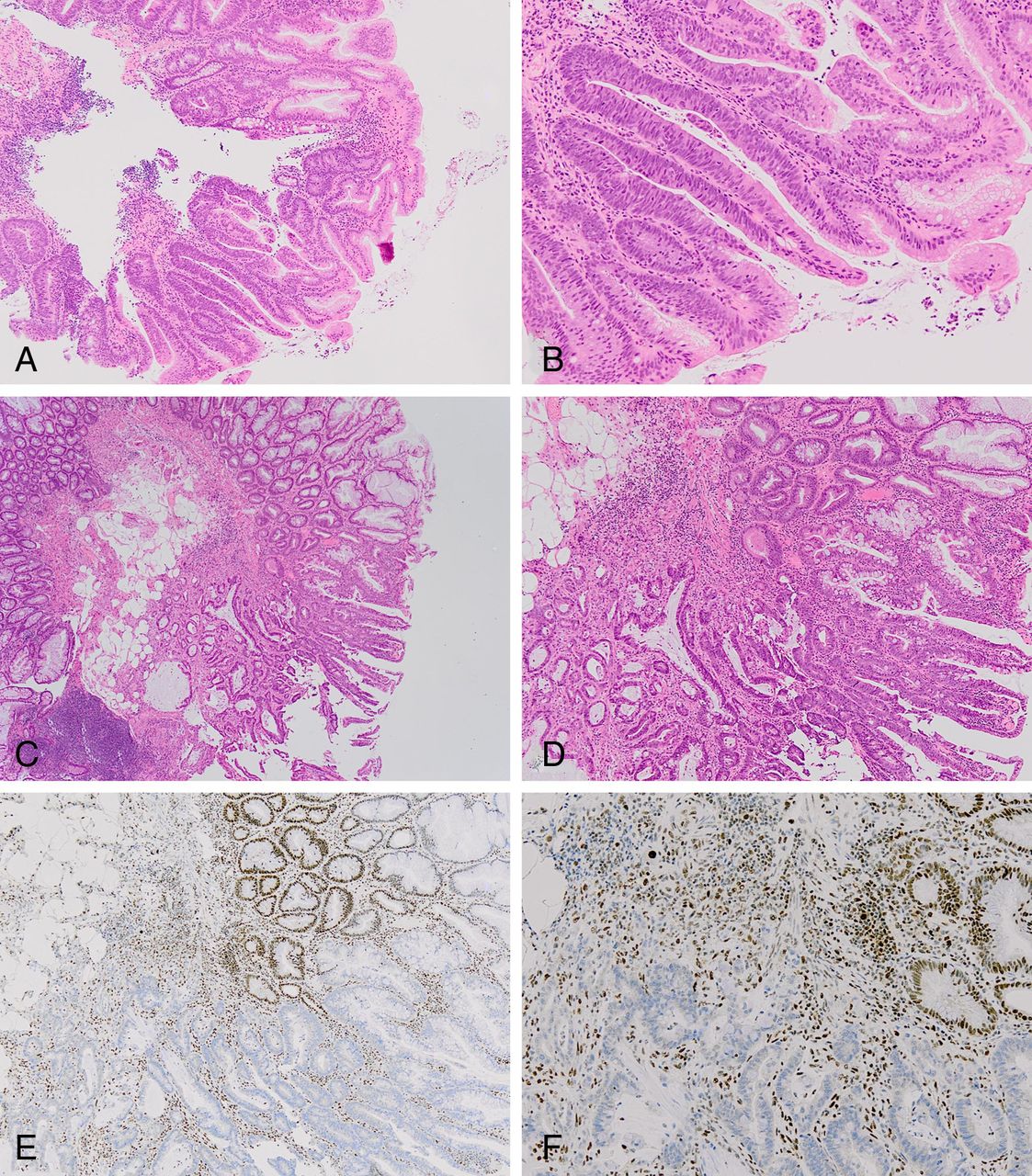
Sessile serrated lesion (SSLs) with ‘conventional’ dysplasia and adenocarcinoma. (a) Low-grade ‘conventional’ dysplasia arising within an SSL (lower half of field). Magnification ×40. (b) As (a). Magnification ×100. (c) ‘Conventional’ dysplasia and adenocarcinoma arising within an SSL (lower half of field). Magnification ×20. (d) As (c). Magnification ×40. (a) to (d)—all—H&E stain. (e) Immunohistochemistry to show loss of nuclear hMLH-1 expression within area of dysplasia and adenocarcinoma. Magnification ×40. (f) As (e). Magnification ×100.
Traditional serrated adenomas
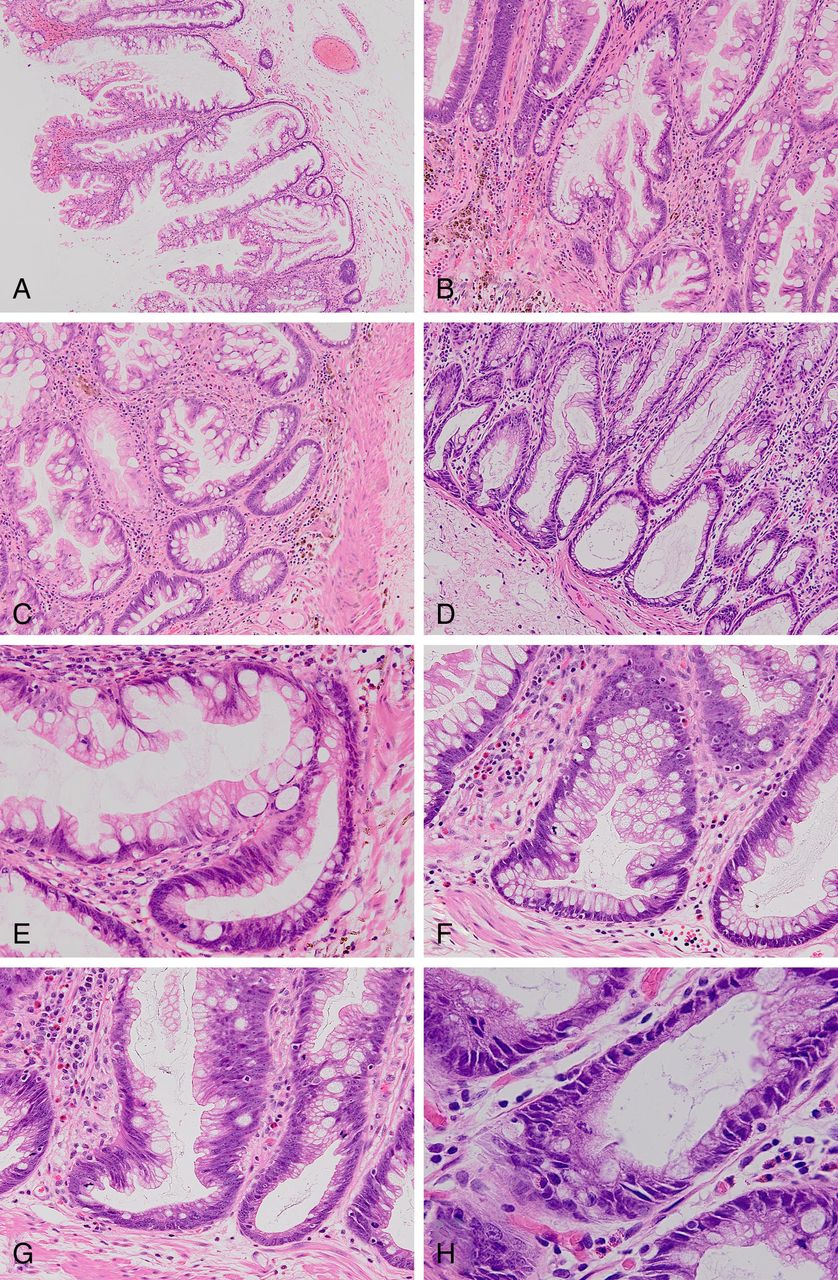
TSAs are relatively uncommon lesions that occur most frequently in the left colon and are characterised by tubulovillous architecture, eosinophilic cytoplasm, elongated (‘pencillate’) nuclei and ectopic crypts, that is, the presence of multiple tiny crypts extending from the primary crypts (figure 4). The latter impart a serrated appearance to the lesion. These areas are usually mixed with areas showing a more typical adenoma growth pattern, and the transition between these areas is classically abrupt. High-grade dysplasia can occur within TSAs and progression to adenocarcinoma may take place, with the latter showing a serrated appearance (see below).7 Occasionally, TSAs may show a strikingly filiform growth pattern.17

The histological features of traditional’ serrated adenomas (TSAs). (a) Low-power view to show filiform architecture. Magnification ×40. (b) Eosinophilic cytoplasm and pencillate nuclei with crypt budding. Magnification ×100. (c) and (d) Crypt budding. Magnification ×200. (e) Crypt budding. Magnification ×400. (f) Eosinophilic cytoplasm and pencillate nuclei. Magnification ×400. (g) A tiny focus of eosinophilic cytoplasm and pencillate nuclei within an otherwise typical ‘classical’ tubulovillous adenoma. Magnification ×200. (h) A focus of crypt budding within an otherwise typical ‘classical’ tubulovillous adenoma. Magnification ×100. All— H&E stain.
The proportion of a lesion that is required to show the characteristic features of a TSA—in contrast to areas showing the appearances of a ‘classical’ adenoma—in order to make a diagnosis of TSA is not clearly defined. Neoplastic epithelium with a focally eosinophilic appearance may be seen in lesions that otherwise show the features of a ‘classical’ tubulovillous adenoma and without the constellation of features that are characteristic of TSAs (figure 4). These lesions are best regarded as ‘classical’ adenomas. However, some lesions comprise almost equal proportions of TSA-like and ‘classical adenoma’-like areas, and it is likely that these will be termed TSAs by some and ‘mixed’ TSA and ‘classical’ adenomas by others. Regardless of the precise terminology used in this situation, the key step is to recognise the lesion as a variant of an adenoma and to be able to grade the dysplasia accurately, as these assessments will allow the correct risk stratification.
Endoscopic recognition of serrated lesions
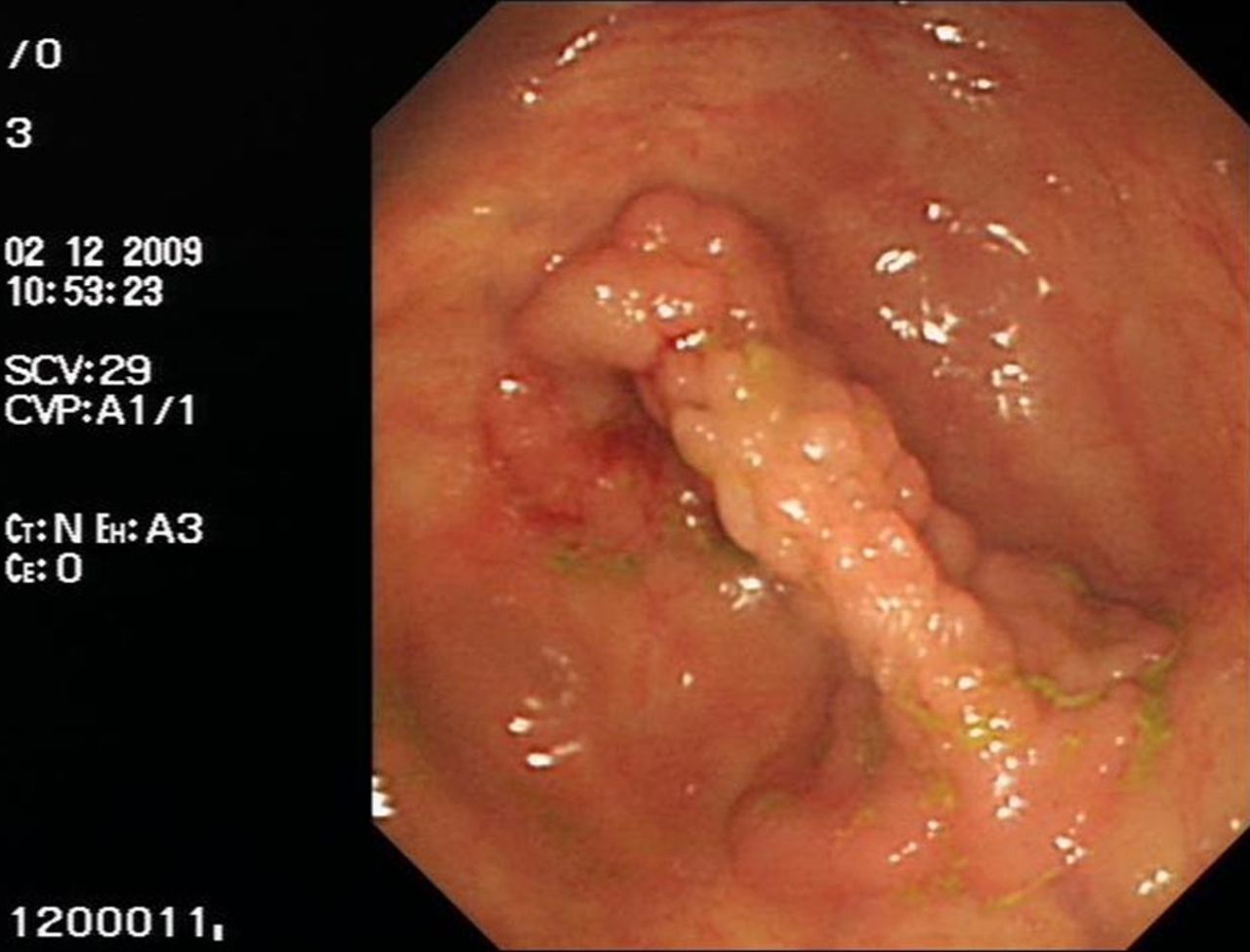
SSLs are often difficult to recognise using conventional endoscopy (figure 5). Presumably this is due to their flat growth pattern and their not uncommon association with mucosal folds. They are also prone to being covered within mucus.18 Endoscopic identification rates for SSLs vary significantly between studies—from 1% to 18% in one study.19 Advanced techniques such as magnifying endoscopy and narrow band imaging may enhance their visualisation.20 ,21 The location and size of serrated lesions can help the endoscopist to determine whether they are likely to be dealing with an HP, an SSL or a TSA. TSAs are more commonly pedunculated, while some have suggested that they possess a red colouration on endoscopic examination—although this does not seem to be a universally held belief.18

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The endoscopic appearance of a sessile serrated lesion.
Serrated polyposis
Serrated polyposis (aka hyperplastic polyposis) is a condition characterised by the presence of multiple serrated polyps within the colorectum. Criteria for the diagnosis of this condition have now been created (box 2).10 The distinct morphological features of these polyps were described by Torlakovic and Snover in 1996, highlighting that the polyps in this syndrome showed important differences from those of sporadic hyperplastic polyps.2 The polyps found in serrated polyposis may be quite variable in histological appearance, even within the same patient. However, the majority show features most in keeping with those of SSLs, with some showing the appearances of ‘classical’ adenomas.2 The fact that the majority of lesions in patients with this condition show the features of SSLs explains why—prior to the identification of SSLs as a distinct entity—the condition was known as ‘hyperplastic polyposis’.
Criteria for the diagnosis of serrated polyposis (‘hyperplastic polyposis’)10
At least five histologically diagnosed serrated polyps proximal to the sigmoid colon, of which two are >10 mm in diameter
Any number of serrated polyps occurring proximal to the sigmoid colon in an individual who has a first degree relative with serrated polyposis
More than 20 hyperplastic polyps of any size but distributed throughout the colon
Serrated adenocarcinoma
It is well established that serrated polyps can progress to CRC (box 3) and the term ‘serrated adenocarcinoma’ has been used to describe these tumours.7 ,22 Just as CRC arising within the classical ‘adenoma-carcinoma’ pathway may be associated with an adjacent residual adenomatous component, serrated polyps are sometimes visible at the edge of CRC arising within the ‘serrated’ pathway. Second, the invasive carcinoma may itself show morphological features that are characteristic of CRC arising in the context of the ‘serrated’ pathway. Before the link between serrated polyps and ‘serrated adenocarcinoma’ was established, the features of ‘serrated adenocarcinoma’ were described within cancers that were MSI-H but sporadic in nature, that is, not arising on the basis of Lynch syndrome. It is very likely that many, if not all, of these cancers in fact arise via the ‘serrated’ pathway. It is currently thought that around a third of cancers that arise from the ‘serrated pathway’ show a serrated morphology—therefore, the majority show features that are not distinguishable from cancers arising from the ‘classical’ adenoma-carcinoma sequence.5
Evidence supporting the link between sessile serrated lesions and colorectal carcinoma7
Progression to carcinoma of lesions originally thought to be hyperplastic polyps
Carcinoma developing in serrated (hyperplastic) polyposis
Presence of dysplasia (conventional and serrated type) in sessile serrated lesions
Metachronous carcinoma in patients with sessile serrated lesions
Presence of sessile serrated lesions adjacent to carcinomas
Morphological and immunohistochemical similarities of some carcinomas to sessile serrated lesions
Mutations and epigenetic phenomena common to various stages of the serrated neoplasia pathway
Similarities of carcinomas and sessile serrated lesions on DNA array analysis
The key histological features of ‘serrated adenocarcinomas’ that distinguish them from ‘conventional’ adenocarcinomas are listed in table 3. Of these appearances, the serrated growth pattern is the most common and the trabecular pattern is the rarest.
The key distinguishing features of serrated adenocarcinomas23
The majority of ‘serrated adenocarcinomas’ arise in the distal colon or rectum. These tumours are MSI-S or exhibit MSI-L and are believed to develop from TSAs. A minority arise within the caecum and ascending colon, show MSI-H and are thought to arise from SSLs.23
There is some evidence that serrated adenocarcinomas possess a worse prognosis than CRC developing along the ‘adenoma-carcinoma’ pathway. In particular, they more commonly show adverse histological factors such as tumour budding.24 Some will also contain KRAS mutations, and these tumours will be resistant to anti-EGFR therapies in the same way to KRAS-mutant CRC arising from the ‘adenoma-carcinoma’ pathway (see below).
Genetic alterations in serrated lesions and progression to cancer
In parallel with the recognition of the morphological features of SSLs came an understanding of the distinct molecular genetic alterations that characterise these lesions. The genes that are most involved in the progression from normal mucosa to CRC are listed in table 4. In addition, it is important to understand the concepts of microsatellite instability, the CpG island methylator phenotype (CIMP) and the Wnt signalling pathway.
The genes most commonly involved (through inactivation, loss or mutation) during the molecular pathways from normal colorectal mucosa to CRC
The KRAS gene encodes the KRAS protein (a proto-oncogene), which is a member of the Ras family of proteins that are very important for signalling in normal cells. Mutations within the KRAS gene are commonly found in carcinomas of the pancreas, lung and colorectum and result in KRAS acting as an oncogene. In CRC, the presence of a KRAS mutation is also a predictor of a poor response to EGFR inhibitors such as cetuximab. This is because certain KRAS mutations result in the KRAS protein becoming self-activating and because KRAS is downstream of EGFR in the signal transduction pathway; pharmacological inhibition of EGFR does not then prevent (aberrant) signal transduction via this pathway when KRAS is mutant.25
The BRAF gene (another proto-oncogene) encodes a protein called B-Raf, which is a member of the Raf kinase family of phosphorylating enzymes that are involved in the control of cell division and differentiation. Acquired BRAF mutations have been identified in many human cancers, including malignant melanoma and carcinomas of the lung and colorectum. These mutations result in BRAF acting as an oncogene. Over 30 mutations have been recognised in the BRAF gene, of which the V600E mutation is the most common (90% of BRAF mutations). The V600E mutation is a single-nucleotide substitution at codon 600 of the gene, leading to an amino acid change from valine (V) to glutamate (E) at this position. CRCs showing both loss of the hMLH-1 protein and the presence of the V600E mutation have lost hMLH-1 expression due to inactivation of the hMLH-1 encoding gene rather than due to an inherited mutation within the gene (ie, Lynch syndrome). Screening for the V600E mutation in this situation therefore reduces the number of cases in which a search for a mutation in the hMLH-1 encoding gene is required.26
The p16 gene is a tumour suppressor gene encoding a protein (cyclin-dependent kinase inhibitor 2A) that is involved in cell cycle control and that may be mutated in several different cancers. The MGMT gene encodes the MGMT protein (methylated DNA protein cysteine methyltransferase) that is involved in DNA repair and that can be inactivated via hypermethylation of its promoter sequence.
Microsatellites are short, non-coding regions of DNA that are scattered throughout the genome. They can act as markers of imperfect DNA replication since when this occurs individual microsatellites are present at differing length within different cells. This phenomenon is termed ‘microsatellite instability’ (MSI). MSI can be present only in some microsatellites (MSI-low or MSI-L) or within many (MSI-high or MSI-H). The presence of MSI-H is commonly associated with defective DNA mismatch repair (ie, the failure of the normal process of correction of imperfections in DNA replication) and is characteristic of Lynch syndrome and in certain CRCs that arise from the serrated pathway. Lesions that show no evidence of MSI are termed ‘microsatellite stable’ (MSS).
The CIMP is a state in which extensive methylation of the promoter sequences of genes—including those encoding certain DNA mismatch repair enzymes—occurs. CpG islands are pairs of cytosine and guanine nucleotides that are present mainly within the promoter regions of genes such as the DNA mismatch repair enzyme-encoding gene hMLH-1. When methylation (a physiological process important in the regulation of gene activity) of these CpG islands occurs, this results in inactivation of the corresponding gene. Methylation may be present at either a low (CIMP-L) or high (CIMP-H) level across the genome.
The Wnt signalling pathways are important cascades of proteins that are involved in signal transduction and control of cellular growth and differentiation. Genes encoding proteins within this pathway can act as oncogenes when their regulation becomes abnormal.
Several different molecular pathways to CRC exist (table 5). The classical Vogelstein ‘adenoma-carcinoma’ model has been established for many years and involves what is believed to be a stepwise accumulation in mutations within, for example, APC (adenomatous polyposis coli; commonly mutated early in CRC), p53 (an important tumour suppressor gene involved in halting cellular proliferation in the presence of DNA damage and promoting apoptosis if this damage cannot be repaired) and SMAD-4 genes (one of a family of genes encoding proteins involved in signal transduction within the TGF-β pathway). Mutations in the KRAS gene may also occur, and the resulting CRCs are MSS and either CIMP-negative or CIMP-L.
Molecular classification of colorectal cancer3
Familial adenomatous polyposis (FAP) is associated with a germline mutation in the APC gene, and the resulting CRC are CIMP-negative and MSS. Lynch syndrome is associated with a germline mutation in one of the DNA mismatch repair enzyme-encoding genes, and the resulting CRC are CIMP-negative and show MSI (the latter is associated with resistance to 5-fluorouracil chemotherapy).
SSLs are associated with early BRAF mutations followed in some cases by loss of hMLH-1 expression due to hypermethylation of the promoter sequence leading to inactivation of the encoding gene, rather than due to a mutation. One study of 148 colorectal polyps found that 90% of SSLs contain the BRAF V600E mutation compared with 29% of (microvesicular) hyperplastic polyps, 36% of TSAs and 5% of ‘classical’ adenomas.27 The resulting CRC contain BRAF mutations, are CIMP-H and exhibit MSI. SSLs in which hMLH-1 expression is not lost may alternatively show p16 and MGMT loss. The resulting CRC again contain BRAF mutations and exhibit CIMP-H but are MSS.
TSAs are particularly associated with early KRAS mutations and Wnt abnormalities. The resulting CRC contain KRAS mutations and exhibit CIMP-L but are MSS.
Management of serrated lesions
Whether or not serrated polyps are identified within the context of the BCSP, the most appropriate management of affected patients requires clarification. Despite the morphological and molecular genetic similarities between microvesicular hyperplastic polyps and SSLs, it is still widely believed that patients in whom hyperplastic polyps are identified do not require follow-up based on this finding alone. On the other hand, TSAs should already be universally recognised as a form of adenoma and patients with these lesions will be managed in the same way as those with ‘classical’ adenomas that exhibit otherwise similar characteristics. For example, within the BCSP this will depend on their number, size and grade of dysplasia.
The optimal management of patients harbouring SSLs is still under discussion. Demonstration of the link between SSLs and CRC has led to an understanding that SSLs—even those without ‘conventional’ dysplasia—are at least as significant as ‘classical’ adenomas in defining cancer risk. This concern has been heightened with realisation that the ‘serrated pathway’ to CRC may be more rapid than the classical ‘adenoma-carcinoma’ sequence (box 4).28 The development of UK guidelines for the management of SSLs is currently under discussion by the British Society of Gastroenterology. It is likely that guidance will advocate complete excision of SSLs, as well as clinical follow-up that is at least as frequent as for ‘classical’ adenomas. Patients in whom serrated polyposis is identified will require even more careful scrutiny.
A suggested colonoscopic surveillance protocol for SSLs28
The numbers of SSLs and ‘classical’ adenomas should be additive. For example, the finding of two classical adenomas <10 mm and one SSL <10 mm should lead to 3-yearly surveillance
Distal small hyperplastic polyps are not associated with an increased risk of colorectal cancer and surveillance should not be increased in frequency because of these lesions unless >20 are present
If the pathologist is unable to distinguish between a hyperplastic polyp and an SSL for technical reasons (eg, tiny biopsy or tangential cutting), then all proximal serrated polyps should be considered to represent SSLs
Patients with serrated polyposis should undergo 2-yearly surveillance after all lesions >5 mm have been resected
Patients undergoing piecemeal resection of an SSL should undergo a site check at 2–6 months
If a large proximal SSL or multiple SSLs are identified, the use of advanced endoscopic techniques should be considered as a means of increasing the detection rate of serrated polyposis
SSL, sessile serrated lesion.
Future advances
Further elucidation of the molecular links between the entire spectrum of serrated lesions and CRC will help to inform the guidelines for patient management and follow-up. In particular, a better understanding of the speed of progression along the ‘serrated pathway’ to CRC may allow enhanced risk stratification for patients in whom these lesions are identified. The similarities between microvesicular hyperplastic polyps and SSLs require further detailed study, and this could lead to a change to the paradigm that sporadically occurring hyperplastic polyps possess no link with the future development of CRC.
Key messages
-
‘Serrated neoplasia’ refers to a range of colorectal lesions with varying degrees of malignant risk, together with distinct forms of adenocarcinoma.
-
Bowel Cancer Screening Programmes have highlighted to histopathologists the importance of recognizing and understanding the biological significance of the spectrum of serrated lesions.
-
The optimal terminology, minimum diagnostic criteria and most appropriate management strategies for some serrated lesions (especially the sessile serrated lesion) are still in evolution.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.