Article Text

Abstract
Objective: To compare test characteristics of the Farr radioimmunoassay and an automated fluorescence immunoassay (ELIA dsDNA test) for the diagnosis of systemic lupus erythematosus (SLE).
Methods: A cross sectional study comprising 440 samples from 440 patients, sent to the laboratory over a three month period for anti-dsDNA testing. Chart review was performed, blinded for test results, to count for each patient the number of American College of Rheumatology criteria for the classification of SLE that were fulfilled. At least four criteria were met by 248 (56%) patients (SLE), one to three criteria by 77 (18%) (lupus-like disease, LLD), and no criterion by 115 (26%) (non-SLE/non-LLD). Results from serum samples from the non-SLE/non-LLD and SLE groups were used to calculate receiver operating characteristic curves.
Results: For the Farr assay, specificities of 95% and 99% corresponded to sensitivities of 72% and 56% respectively. For the ELIA dsDNA test these levels of specificity corresponded to sensitivities of 44% and 17% respectively.
Conclusions: The Farr radioimmunoassay is superior to the ELIA dsDNA test for identifying patients with SLE.
- fluorescence immunoassay
- double stranded DNA
- lupus-like disease
- ACR, American College of Rheumatology
- ANA, antinuclear antibodies
- CDLE, chronic discoid lupus
- CLIF, Crithidia luciliae immunofluorescence
- dsDNA, double stranded DNA
- ELIA, fluorescence immunoassay
- ELISA, enzyme linked immunosorbent assay
- LLD, lupus-like disease
- ROC, receiver operating curve
- SLE, systemic lupus erythematosus
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- ANA, antinuclear antibodies
- CDLE, chronic discoid lupus
- CLIF, Crithidia luciliae immunofluorescence
- dsDNA, double stranded DNA
- ELIA, fluorescence immunoassay
- ELISA, enzyme linked immunosorbent assay
- LLD, lupus-like disease
- ROC, receiver operating curve
- SLE, systemic lupus erythematosus
Between 60% and 80% of patients with systemic lupus erythematosus (SLE) have circulating antibodies to double stranded DNA (dsDNA) at some time during their illness.1 Their presence provides the clinician with one out of the four American College of Rheumatology (ACR) criteria necessary to classify a patient as having SLE.2 The techniques most commonly used for detection of anti-dsDNA antibodies are enzyme linked immunosorbent assay (ELISA), indirect immunofluorescence using the haemoflagellate Crithidia luciliae (CLIF), and the Farr radioimmunoassay.3 The techniques of ELISA and CLIF detect anti-dsDNA antibodies with both high or low avidity. As the Farr assay includes ammonium sulphate precipitation at high salt concentrations, a condition that dissociates dsDNA-anti-dsDNA complexes of low avidity,4 this assay detects only antibodies with high avidity.5 High avidity anti-dsDNA antibodies are more specific for SLE than those with low avidity5 and have high predictive value for the development of SLE if present in patients with manifestations compatible with SLE who fulfil fewer than four ACR criteria at the time of evaluation (lupus-like disease, LLD).6
Recent communications suggest that a non-radioactive automated fluorescence immunoassay (ELIA dsDNA test) has similar test characteristics to those of the Farr radioimmunoassay.7–9 This study compares both tests in a setting that mimics daily clinical practice.
PATIENTS AND METHODS
Patient samples
We included all 440 blood samples from 440 different patients, sent to the immunology laboratory of our hospital for anti-dsDNA testing between February and May 2001. One of us (RHWMD), blinded for test results, reviewed clinical charts and scored the number of ACR criteria2 that each patient fulfilled. Patients with four or more criteria were classified as having SLE; those with one to three criteria as having LLD. Those who met no criterion or had a positive test for antinuclear antibodies (ANA, as measured by Hep-2000 immunofluorescence) as the only criterion were classified as non-SLE/non-LLD.
Anti-dsDNA antibodies
Anti-dsDNA antibodies were determined according to the manufacturer's instructions with the Farr assay (Diagnostic Products Corporation, Los Angeles, USA) using 125I-labelled recombinant dsDNA and the ELIATMdsDNA test (Pharmacia BV Diagnostics GmbH and Co, KG, Freiburg, Germany) that uses single polystyrene wells coated with double stranded cyclic plasmid DNA of Escherichia coli, which are automatically dispensed and processed (including instrument dilution of patient samples) in the UniCAP® 100ε instrument at 37°C (Pharmacia and Upjohn Diagnostics GmbH and Co, KG, Freiburg, Germany). Results were expressed in IU/ml, using Wo/80 as the ultimate standard. Cut off levels advised by the manufacturer are 10 IU/ml (Farr assay) and 15 IU/ml (ELIA dsDNA test). For both tests intra-assay and interassay variations were<10%.
RESULTS
Patient characteristics
One hundred and fifteen (26%) patients (69% women; median age 40 years) were classified as non-SLE/non-LLD, 77 (18%) patients as LLD (86% women; median age 35 years), and 248 (56%) patients as SLE (90% women; median age 35 years; median disease duration 10 years). In the non-SLE/non-LLD group, respectively 20% and 0% of patients had a history of a positive antinuclear antibody (ANA) and anti-dsDNA test result. For the LLD and SLE groups these percentages were 70% and 98% for ANA, and 26% and 87% for anti-dsDNA. Figure 1 depicts frequencies of ACR criteria in patients with LLD or SLE. Patients with SLE met a median of five ACR criteria (range 4 to 10). Had the presence of anti-dsDNA antibodies not been tested for, 18% of patients with SLE would have only met three criteria.

Prevalence of ACR criteria for the classification of systemic lupus erythematosus (SLE) in 77 patients with lupus-like disease (LLD) and 249 patients with SLE. Numbers on the x axis represent individual criteria. 1, Butterfly rash; 2, chronic discoid lupus (CDLE); 3, photosensitivity; 4, oropharyngeal ulcers; 5, arthritis of at least two joints; 6, anti-dsDNA antibodies (any assay, any time); 7, nephritis; 8, serositis; 9, psychosis and/or epilepsy; 10, haemolytic anaemia, leucocytopenia, and/or thrombocytopenia; 11, ANA.
Results with the Farr and ELIA dsDNA test
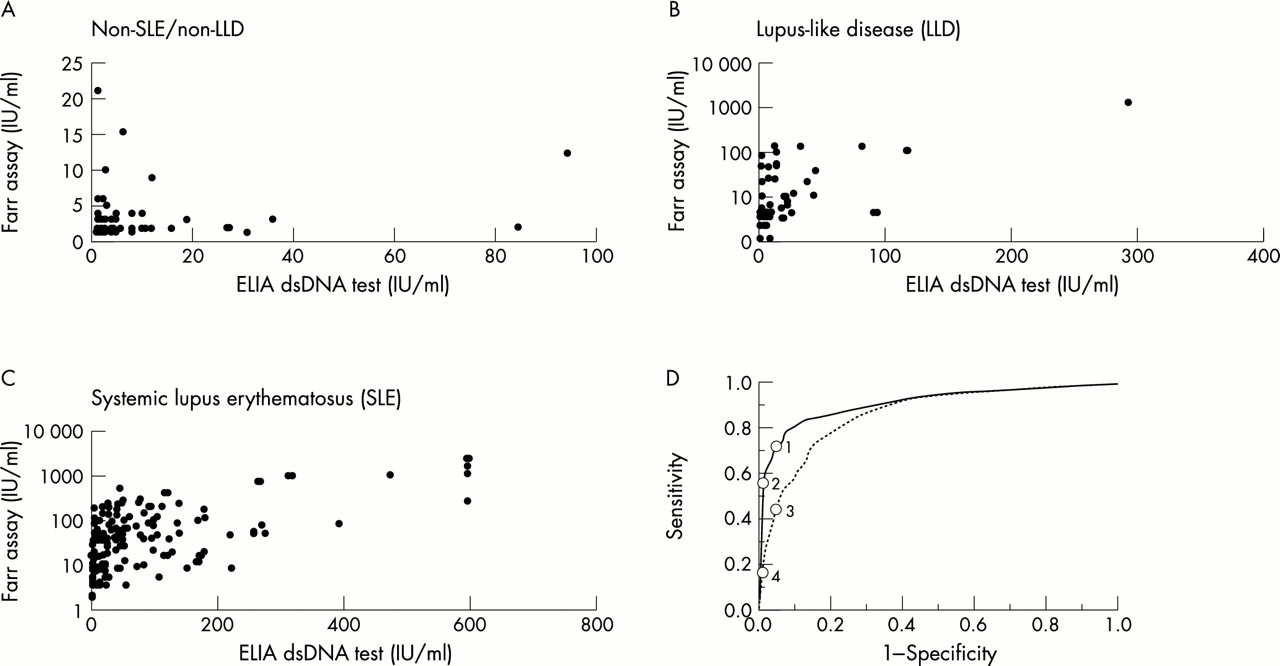
Figure 2 (panels A-C) shows results with both anti-dsDNA tests for all three groups of patients. We used results with samples from SLE and non-SLE/non-LLD groups to calculate receiver operating curves (ROCs) (fig 2, panel D). A specificity of 95% corresponded to a cut off point between “negative” and “positive” results of 6 and 19 IU/ml for the Farr assay and the ELIA dsDNA test, respectively. Corresponding sensitivities were 72% (Farr assay) and 44% (ELIA dsDNA test). Specificities and sensitivities with cut off levels advised by the manufacturers (10 IU/ml for Farr assay; 15 IU/ml for ELIA dsDNA test) were 98% and 59% for the Farr assay, and 94% and 47% for the ELIA dsDNA test, respectively. With a cut off point at 12 IU/ml, the Farr assay reached a specificity of 99% (corresponding sensitivity 56%). For the ELIA dsDNA test 99% specificity was reached with a cut off point at 84 IU/ml, with a corresponding (clinically irrelevant) sensitivity of 17% (fig 2, panel D).

{kind=link}
{kind=link}
Results with the Farr assay and ELIA dsDNA test in IU/ml for the patients who were non-SLE/non-LLD (n=115, panel A), patients with LLD (n=77, panel B), and those with SLE (n=248, panel C). The results for the Farr assay are shown in panels A, B and C on the y axis; the y axis in panels B and C has a log scale. Panel D depicts the ROC curve for the Farr assay (continuous line) and ELIA dsDNA test (dotted line). Circles 1 and 2 correspond to cut off points for the Farr assay of 6 IU/ml and 12 IU/ml, respectively. These cut off points result in 95% and 99% specificity, respectively. Circles 3 and 4 correspond to cut off points with the ELIA dsDNA test of 19 IU/ml and 84 IU/ml, respectively. These cut off points have a specificity of 95% and 99%, respectively.
For a test result considered positive with values exceeding the cut off point corresponding to 95% specificity (≥6 IU/ml for the Farr assay and ≥19 IU/ml for the ELIA dsDNA test), 12 (10%) samples from the non-SLE/non-LLD group, 29 (38%) from the LLD group, and 188 (76%) from the SLE group, were positive with at least one anti-dsDNA test. Table 1 gives details on corresponding patients from the first two groups. A positive ANA test was present in four out of seven (57%) Farr positive and one out of six ELIA dsDNA test positive samples from patients in the non-SLE/non-LLD group. In samples from patients with LLD all Farr positive samples and all but two ELIA dsDNA test positive samples were ANA positive. In samples from patients who were non-SLE/non-LLD, the titre in the Farr assay was ≤10 IU/ml in five out of six who were Farr positive and ELIA dsDNA test negative, whereas the titre in the ELIA-dsDNA test was >15 IU/ml in five Farr negative, ELIA dsDNA test positive samples. As a result, the use of cut off points advised by the manufacturer reduced the number of Farr positive samples in the non-SLE/non-LLD group to two, whereas the number of ELIA dsDNA test positive samples was unchanged. Application of cut off points advised by the manufacturers to samples from patients with LLD reduced the number of positive samples in the Farr assay from 25 to seven and did not affect the number of positive samples with the ELIA dsDNA test.
Characteristics of patients in the non-SLE/non-LLD group (n=12) and with lupus-like disease (n=29) and a positive Farr assay (≥6 IU/ml) and/or a positive ELIA dsDNA test (≥19 IU/ml). Bold numbers with titres (IU/ml) correspond with positive test results
Taking ≥6 IU/ml for the Farr assay and ≥19 IU/ml for the ELIA dsDNA test as cut off points for a positive test, 77 samples (31%) from patients with SLE were Farr positive and ELIA dsDNA test negative and seven samples (3%) were Farr negative and ELIA dsDNA test positive. Application of the manufacturers' cut off points reduced the number of Farr positive and ELIA dsDNA test negative samples to 49 and increased the number of Farr negative and ELIA dsDNA test positive samples to 17. Overall, application of the manufacturers' cut off points decreased the number of Farr positive SLE samples from 181 (73%) to 150 (60%) and increased the number positive in the ELIA dsDNA test from 111 (45%) to 118 (48%).
DISCUSSION
Compared with the Farr radioimmunoassay the recently introduced ELIA dsDNA test has several advantages. The test does not use radioactive materials (no specific location in the laboratory or specialised personnel needed; no fear of radioactive irradiation for technicians and milieu), takes less time (a run takes 2.5 hours compared with seven hours with the Farr assay; “hands on” time: one hour v five hours with the Farr assay) and has a similar cost per analysed sample (considering materials, technicians, and apparatus). For diagnostic purposes clinicians need a disease specific and sensitive assay. The ROC curves (fig 2 D) clearly showed that the Farr assay performs better than the ELIA dsDNA test. Other communications published in abstract form7–9 concluded that specificity and sensitivity are almost the same for both assays. A likely explanation for these different conclusions is a difference in study design. The other studies7–9 compared test results with samples from patients with SLE with those from healthy blood donors, “control sera”, patients with Sjögren's syndrome, rheumatoid arthritis, “various disorders”, and patients with IgA nephritis. Our study design differs in two important aspects. Firstly, our setting mirrors daily clinical practice as we used all requests for anti-dsDNA testing that came from the clinic to the laboratory. Secondly, we divided the patients into SLE, LLD and non-SLE/non-LLD groups, blinded for the test results, and did not use the results in the LLD group for calculation of specificity and sensitivity. Identification of patients with LLD is of importance when an anti-dsDNA test is evaluated. As a patient is allowed to “collect” the required number of ACR criteria over any period,2 the result of an anti-dsDNA test cannot be classified as “incorrect” in a patient with clinical manifestations that are compatible with SLE. We consider differences in the percentage of included SLE patients with active disease a less likely explanation for the different conclusions of our study and those of others,7–9 as this difference holds for the ELIA dsDNA test and not for the Farr assay. The test characteristics with the Farr assay in our study (depending on the cut off point specificity of 95% to 72%), were comparable with those in the other studies (specificity 96%, sensitivity 32%7; specificity >90%, sensitivity 71%8; specificity 99%, sensitivity 63%9).
Almost all Farr positive samples in our study also had a positive ANA test, as expected for samples with anti-dsDNA antibodies. However, several samples that were ELIA dsDNA test positive and Farr negative were ANA negative (table 1). These findings suggest that both assays may detect different antibodies.
It should be stressed that our study was only designed to evaluate the diagnostic capacity of the Farr assay and ELIA dsDNA test. It has been shown that changes in antibody levels as measured by the Farr assay10,11 and ELISA or CLIF techniques12 are related to exacerbations of disease. Further studies are needed to evaluate whether this also holds for the ELIA dsDNA test.
Acknowledgments
We thank Mr T de Poorter, Pharmacia BV Diagnostics, Woerden, the Netherlands for providing the apparatus and materials for the ELIA dsDNA test.