Article Text

Abstract
Rat bite fever is a rarely reported acute febrile bacterial illness caused by Streptobacillus moniliformis or Spirillum minus following a rat bite. It is classically characterised by abrupt onset of fever with rigors, myalgias, headache, and the appearance of a generalised maculopapular petechial skin rash. Polyarthritis complicates the course of the disease in up to 50% of infected patients, and numerous hurdles can make the diagnosis particularly difficult in the absence of fever or rash, as in the present case. A high degree of awareness is necessary to make the correct diagnosis in such cases. Diagnosis has important prognostic implications as the disease is potentially lethal, but easily treatable.
- Streptobacillus moniliformis
- infectious arthritis
- rat bite fever
- MCP, metacarpophalangeal
- NSAIDs, non-steroidal anti-inflammatory drugs
Statistics from Altmetric.com
Rat bite fever is a rarely reported streptobacillar acute febrile illness following a rat or other rodent bite.1,2 Classically, following a rat bite and a short incubation of 1–3 days, systemic dissemination of the organism will initiate the pyogenic response with the formation of abscesses in many tissues from the brain and myocardium to soft tissue and joints, with true septic polyarthritis.1,2
If locally there is minimal inflammation and prompt healing of the wound with absent or minimal regional adenopathy, abrupt onset of disease with intermittent fever, rigors, myalgias, headache, malaise followed by the appearance of a generalised maculopapular or petechial skin rash most prominent in the extremities this will almost certainly suggest an infectious cause for the polyarthritis.1,2
However, only a high degree of awareness and knowledge of the diagnosis in any case of undetermined polyarthritis will allow the diagnosis of rat bite fever to be made when classical symptoms such as fever or rash are missing, as illustrated in the following case history.
CASE HISTORY
A 72 year old man was admitted for subacute polyarthritis. Except for a history of prosthetic surgery of both knees five years ago for osteoarthritis, the patient was in good general health until one month before admission. He then began to notice fluctuating pain and swelling of the left knee, which became constant and was followed by an involvement of the other knee and both elbows. Despite a course of non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids (deflazacort) prescribed by his general practitioner, the situation progressively worsened until the patient was bedridden and finally admitted to hospital.
On admission, the patient was in severe pain. He presented a slightly asymmetric polyarthritis, with involvement of both knees, the right elbow, and the 3rd left metacarpophalangeal (MCP) joint, which were warm, swollen, and very tender on palpation. The patient had no history of fever, rash, tick bite, dental work, travel, injections, or any other infectious risk factor. Personal, familial, and systematic histories did not contribute and there was no evidence for previous or current neoplastic disease. Clinical examination showed arthritis of the joints described, a palpable spleen tip, and osteoarthritic changes of the hands (Heberden nodes and MCP joints II and III) (fig 1A). There was no fever, adenopathy, cutaneous lesions, heart murmur, or signs of an infectious or systemic disease. Initial laboratory examinations showed an erythrocyte sedimentation rate of 125 mm/1st h, a C reactive protein of 120 mg/ml (normal <10), and a white cell count of 11.3×109/l with 81% neutrophils, but were otherwise normal. Chest and knee x ray examinations failed to demonstrate abnormalities or any signs of prosthesis loosening. Hand radiographs confirmed moderate osteoarthritic changes of the interphalangeal joints, MCP joints, and wrists with cartilage calcification compatible with chondrocalcinosis. Microcrystalline disease was, however, considered unlikely as the cause of the present clinical picture in a patient gradually worsening despite almost one month’s treatment with NSAIDs and corticosteroids. A right knee arthrocentesis, performed by the orthopaedic surgeons because of the prosthetic material, demonstrated numerous leucocytes (around 50×109/l) with 83% neutrophils, but no germs or crystals were seen on the direct examination.

{kind=link}
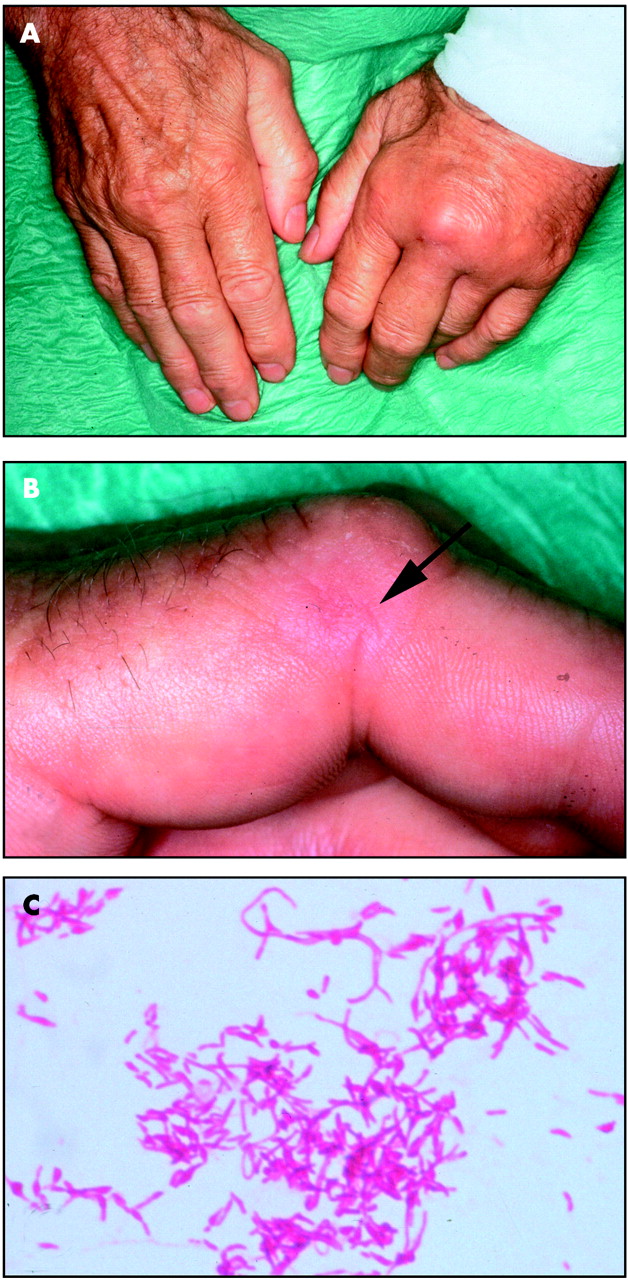
(A) Arthritis of the 3rd metacarpophalangeal (MCP) joint and osteoarthritic changes with Heberden nodes and prominence of the 2nd and 3rd MCP joints. (B) Close up of the middle finger near the interphalangeal joint showing a minimal scar of the rat bite (arrow). (C) Gram stain of Streptobacillus moniliformis demonstrating the typical pleomorphic necklace-like appearance responsible for its name.
After 48 hours, all synovial fluid cultures and three pairs of haemocultures remained sterile, and a thoracoabdominal computed tomographic scan failed to show any abnormality. The patient was finally given an intravenous bolus of corticosteroids for a presumptive diagnosis of atypical rheumatoid arthritis, and his symptoms improved slightly. Nevertheless, this treatment was interrupted two days later and broad spectrum intravenous antibiotic treatment started after rearthrocentesis of both knees, the right elbow, and the 3rd left MCP joint when the microbiology department reported an atypical, slow growing germ, in an initial anaerobe culture of the synovial fluid. A week later, the same germ was finally demonstrated in all synovial samples except that from the MCP joint, and identified as S moniliformis, one of the aetiological agents of rat bite fever (fig 1C) with Spirillum minus. All haemocultures remained sterile and final confirmation was obtained by sequencing of 16S rRNA (Professor M Altwegg, Institute for Medical Microbiology, University of Zurich, Switzerland).3
In the light of the bacteriological findings, a further history was obtained. The patient finally remembered that a rat had bitten him around 15 days before the start of his illness. He lived in an urban setting and while taking out his trash, he saw a small rat near the trashcans. As an animal lover, he picked it up by the tail to prevent him being run over by the garbage truck. This “ungrateful little rat” found nothing better to do than to bite him in the middle finger of the left hand (fig 1B). As the wound healed without local complication after a simple disinfection, the patient did not remember it.
With antibiotic treatment, recovery was rapid and satisfactory, and the patient was discharged. Because of the prosthetic material, he continued to receive antibiotics for three months and is now well, without signs of recurrence or inflammation, for more than two years.
DISCUSSION
No precise data are currently available on the true incidence of rat bite fever as it is not a reportable disease, but it appears to be unusual in Western countries. The major risk factor is exposure to rats, either as an occupational hazard for people such as laboratory workers, or occur in the lower socioeconomic population, especially homeless people.1,4 Ownership of pets such as rats or snakes may represent another growing risk factor, especially for children. It should be realised that from 50% to 100% of healthy wild, but also laboratory rats, harbour S moniliformis in their nasopharynx.1 Furthermore, it has also been found in other rodents such as mice, squirrels, gerbils, or weasels and in pets that prey on these rodents, such as cats and dogs.1 The risk of developing rat bite fever after being bitten or scratched is fairly high, estimated to be around 10%.2 Finally, as stated before, there is usually minimal local inflammation with prompt healing of the wound and immediate disinfection appears not to prevent the infection, as in our case.2
Apart from the already mentioned classical manifestations of rat bite fever with abrupt onset of fever, headache, myalgia, and various cutaneous rashes,1 it is important to emphasise that up to 50% of the infected patients will develop an asymmetric migrating polyarthritis.1,5 It affects the knees, shoulders, elbows, wrists and hands, while characteristically the bitten area seems to heal.1,5 Joint effusion appears more common in adults than in children4 and, as in the present report, it is exceedingly painful.4 Because of the polyarticular nature of the disease, an immunological component has been suggested as a contributing factor.5 Nevertheless, in cases like ours, it is a true infectious polyarthritic disease. Although most cases seem to resolve spontaneously within two weeks, persistence up to two years has been reported,1 and the mortality in untreated cases is around 10–15%,1 rising even to 53% in rare cases with cardiac involvement with peri- or endocarditis.6
Diagnosis can be difficult. Firstly, because of lack of familiarity, but also because no reliable serological test is available and the definitive diagnosis requires isolation of S moniliformis either from the wound, the blood, or the joint fluid, especially in the absence of a history of rodent bite. S moniliformis is a highly pleomorphic Gram negative rod, which may stain positively on Gram stain and is often dismissed as a proteinaceous debris because of its numerous bulbous swellings with occasional clumping (moniliformis means necklace-like).1,4 To make the matter worse, growth requires microaerophilic or anaerobic conditions and media supplementation with blood or serum, and is inhibited by sodium polyanethol sulphonate,1,4 a common adjunct in most commercially available blood culture media. This could explain why our MCP sample, which was inoculated directly in an haemoculture bottle, remained sterile.
We believe this case illustrates well the difficulties of diagnosing rat bite fever in the absence of classical “infectious” signs and symptoms. This diagnosis should be entertained as a possible cause of any undetermined polyarthritis because the patient may minimise or forget the bite, especially in the absence of a local reaction. Pet lovers or laboratory workers who handle rodents daily may also regard bites as commonplace. Furthermore, the microbiology laboratory should be specifically notified of any clinical suspicion because of the hurdles in the identification of S moniliformis. Finally, confirming the diagnosis has important prognostic implication as the disease is potentially lethal but easily treatable by a simple course of penicillin, or tetracycline for allergic patients, even in the presence of prosthetic material as in our case.