Role of glycaemic control in development of microalbuminuria in patients with insulin dependent diabetes
BMJ 1994; 309 doi: https://doi.org/10.1136/bmj.309.6969.1608 (Published 17 December 1994) Cite this as: BMJ 1994;309:1608
- J K Powrie,
- G F Watts,
- J N Ingham,
- N A Taub,
- P J Talmud,
- K M Shaw
- Division of Medicine, United Medical and Dental Schools of Guy's and St Thomas's Hospitals, St Thomas's Hospital, London SE1 7EH, lecturer in medicine. University of Western Australia, Royal Perth Hospital, PO Box X2213, Perth, Western Australia 6001, senior lecturer in medicine. Department of Diabetes and Endocrinology, Queen Alexandra Hospital, Portsmouth PO6 3LY, registrar in medicine, consultant physician Department of Public Health Medicine, United Medical and Dental Schools of Guy's and St Thomas's, St Thomas's Hospital, London SE1 7EH, lecturer in medical statistics. Division of Cardiovascular Genetics, University College London Medical School, London WC1E 6JJ, senior lecturer in cardiovascular genetics.
- Correspondence to: Dr Powrie.
- Accepted 5 October 1994
Abstract
Objective: To ascertain which factors determine the progression from very low rates of albumin excretion to persistent microalbuminuria in patients with insulin dependent diabetes mellitus.
Design: A 10 year prospective study of a cohort of diabetic patients.
Setting: Outpatient department of the Portsmouth District Hospitals. Subjects—97 patients with insulin dependent diabetes mellitus who were initially free of microalbuminuria and hypertension. Main outcome measure—Urinary albumin: creatinine ratio.
Results: Eight of the 97 patients had developed microalbuminuria (urinary albumin:creatinine ratio > 3 mg/mmol in three consecutive early morning samples) by the 10 year follow up. The group who developed microalbuminuria had higher baseline log 10 plasma glucose concentrations (mean (SD), 1.210 (0.122) (upsilon) 0.984 (0.196) mmol/l, P < 0.001) and glycated haemoglobin concentrations (1.112% (0.069%) (upsilon) 0.997% (0.076%), P < 0.001) and a younger age at onset of diabetes (10.0 (5.5) (upsilon) 15.6 (7.8) years, P < 0.05). There was no difference in baseline duration of diabetes, smoking, sex, insulin dose, body mass index, serum creatinine concentration, or systolic, diastolic, or mean arterial blood pressure between the two groups. Multiple linear regression analysis showed that urinary albumin:creatinine ratio at 10 years was influenced by initial albumin: creatinine ratio (P = 0.006), initial glycated haemoglobin concentration (P = 0.002), and duration of diabetes (P = 0.045). Genotype for angiotensin converting enzyme was not related to the development of microalbuminuria nor, in a larger group of patients, the presence of any degree of diabetic nephropathy.
Conclusion: In patients with insulin dependent diabetes mellitus the progression of minimal albuminuria and the development of microalbuminuria is determined primarily by poor long term glycaemic control. There is a weaker relation with longer duration of disease and younger age at onset of diabetes, but blood pressure does not seem to be implicated. Gene polymorphism for angiotensin converting enzyme is not linked to the development of microalbuminuria or established diabetic nephropathy.
Key messages
Key messages
Renal disease still affects about 30-40% of patients with insulin dependent diabetes
Urinary albumin excretion rates of above 30 μg/min (microalbuminuria) predict the later development of overt diabetic nephropathy
This study shows that the development of microalbuminuria over 10 years is related mainly to poor glycaemic control and urinary albumin:creatinine ratio at baseline
Blood pressure and genotype for angiotensin converting enzyme do not seem to predict microalbuminuria
These data provide further evidence implicating poor glycaemic control as the main initiating factor for the development of nephropathy in insulin dependent diabetes mellitus
Introduction
About 30-40% of patients with insulin dependent diabetes mellitus will develop overt diabetic nephropathy, a major cause of morbidity and mortality in this condition. The remainder of patients seem to be protected against this complication, even in the presence of long duration of disease, and the reasons for this incongruity have not been identified. Clinical nephropathy is heralded by the development of persistent proteinuria in excess of 0.5 g/24 hours.1 The development of clinical nephropathy is preceded by a period of increased urinary albumin excretion,2 3 4 5 so called microalbuminuria, the measurement of which allows identification of those at risk of clinical nephropathy and the possibility of early therapeutic intervention. Once microalbuminuria has developed then it is associated with hypertension and poor glycaemic control.3 5 6 It is not clear, however, whether these associated abnormalities are a cause or consequence of the early renal changes signified by the microalbuminuria.
There is debate concerning the factors that initiate change from normal albumin excretion to microalbuminuria and thence overt renal damage. Thus poor glycaemic control, hypertension, and possibly dyslipoproteinaemia and smoking have all been implicated as initiating factors,7 8 9 10 11 whereas parental history of hypertension12 or vascular disease13 and more recently angiotensin converting enzyme gene polymorphism14 have been suggested as the genetic factors predisposing to diabetic renal disease. Verification of these factors would help in the understanding of diabetic nephropathy and allow planning of strategies to screen for it and perhaps enable early intervention to try to prevent this distressing complication.
We have investigated the development of microalbuminuria over a period of 10 years by means of a longitudinal study in a cohort of well documented patients with insulin dependent diabetes in the Portsmouth area.15
Patients and methods
Details of the cohort of patients have been published elsewhere.15 Briefly 172 patients with insulin dependent diabetes were recruited from the outpatient clinics of the Portsmouth District Hospitals in 1984 with a view to setting up an observational cohort study investigating various aspects of early diabetic nephropathy. There was a deliberate selection policy for patients with a duration of diabetes between five and 20 years. Exclusion criteria comprised a supine blood pressure > 160/95 mm Hg, current use of antihypertensive drugs, and any chronic disease other than diabetes which could potentially interfere with the study. Details were taken of current or recent illness, smoking habits, insulin dose, and prescribed drugs. Body weight, height, and pulse rate were recorded, and blood pressure was measured after 5 minutes' rest in the supine position (diastolic blood pressure measured at Korotkoff phase V); a standard mercury sphygmomanometer was used with the cuff being kept level with the heart, the mean of three readings being recorded. Mean arterial blood pressure was calculated as diastolic pressure plus one third of the pulse pressure. Blood samples were taken for estimation of blood glucose, creatinine, and glycated haemoglobin concentrations. Two early morning samples of urine were taken for estimation of albumin and creatinine concentrations at entry into the study. These were taken on separate days not more than two months apart.
One hundred and twenty seven patients were all followed up at a median of 9.6 years (range 8.4-10 years) at which time clinical details were again recorded and three further early morning urinary samples were taken for estimation of albumin and creatine concentrations. Whole blood samples were stored in EDTA for genotyping for angiotensin converting enzyme.
For the purposes of this study we further excluded patients in whom either of the two baseline early morning urinary albumin:creatinine ratios were >/=3 mg/mmol as this is the value above which albumin excretion has been conclusively shown to predict overt renal disease.2 4 Thus all patients included in the study were initially free of significant microalbuminuria. Table I gives details of the remaining 97 patients at entry into the study and 10 years later. We defined persistent microalbuminuria as an albumin:creatinine ratio of >3 mg/mmol in all three of the early morning urine samples taken at the 10 year follow up.16
—Characteristics at baseline and at 10 year follow up of 97 patients with insulin dependent diabetes included in study. Values shown for insulin dose, body mass index, blood pressure, and concentrations of plasma glucose, glycated haemoglobin, and serum creatinine are based on mean of two baseline measurements but one 10 year follow up measurement for each patient. Plasma glucose was not measured at 10 year follow up visit
Control subjects for genotyping for angiotensin converting enzyme were 364 men aged 51-60 years selected from the register of a general practice in Camberley, Surrey. Patients were excluded if they were suffering from any intercurrent illness or if they were known to have diabetes or coronary artery disease.
LABORATORY MEASUREMENTS
Urine albumin concentration was measured by radioimmunoassay17; the interassay coefficient of variation was < 9%. Urinary creatinine concentration was measured by an end point Jaffe reaction with an interassay coefficient of variation of < 6%. Both initial and follow up samples were analysed by the same methodology. Plasma glucose concentration was measured on the Yellow Springs Analyser (Clandon Scientific, United Kingdom). Glycated haemoglobin concentration was measured by an electroendosmotic method by using agar gel electrophoresis (Corning Medical, United Kingdom) with an interassay coefficient of variation of < 4%. Serum creatinine concentration was measured on a SMAC-II analyser (Technicon), the creatinine clearance being derived from the Cockcroft and Gault equation.18
Genotyping of angiotensin converting enzyme I/D polymorphism was carried out on DNA isolated from whole blood by using the “salting out” procedure.19 The I/D polymorphism in intron 16 of the angiotensin converting enzyme gene was detected by amplification of the polymerase chain reaction and analysis of the resulting fragments by agarose gel electrophoresis as described elsewhere.20
STATISTICAL ANALYSES
Variables that were not normally distributed were logarithmically transformed and are summarised by the geometric mean together with the standard deviation as a multiplicative factor. Categorical data were defined as binary variables. The baseline variables and angiotensin converting enzyme genotype in the group of patients who developed microalbuminuria were compared with those in the group who did not develop microalbuminuria by using the MannWhitney or Fisher's two sided exact test. The baseline variables of insulin dose; body mass index; blood pressure; concentrations of plasma glucose, glycated haemoglobin, and serum creatinine; and albumin: creatinine ratio used in the statistical analyses were all the mean of those recorded or measured at two separate visits not more than two months apart. Multiple linear regression models were used to examine which baseline variables (explanatory variables) predicted the urinary albumin:creatinine ratio at 10 years (outcome variable). The models used included those baseline variables which were found to show significant association with albumin:creatinine ratio at follow up on univariate regression analysis or which were a priori considered to be potentially important predictors of microalbuminuria. Baseline variables showing high correlation were not both included in the model; thus glycated haemoglobin concentration was used rather than plasma glucose concentration and duration of diabetes rather than age at onset. A P value of < 0.05 was taken to indicate significance.
Results
One hundred and twenty seven of the original 172 patients were followed up at a median period of 9.6 years (range 8.4-10.0 years). Twelve patients had died during this period (eight of myocardial infarction, two of malignant disease, one of an insulin overdose, and one in a road traffic accident) 11 had left the Portsmouth area, we could not contact 18, and four refused to attend for a further visit. Of the 127 who returned 97 fulfilled the criteria of having an albumin: creatinine ratio of < 3 mg/mmol in both baseline samples. Eight (four men and four women) of these 97 patients (8.2%) developed persistent microalbuminuria (albumin: creatinine ratio >3 in all three urine samples at follow up over the 10 year period of the study. Only one of these patients with microalbuminuria was taking antihypertensive drugs (enalapril 5 mg/ day). There was progression of albumin excretion in the group as a whole; the mean albumin:creatinine ratio increased from 0.67 to 1.29 mg/mmol, and this was highly significant (P<0.0001, paired t test).
Table II shows a comparison of the various baseline variables in those who had (microalbuminuric) and had not (normoalbuminuric) developed microalbuminuria by the follow up at 10 years. Younger age at onset of diabetes was associated with development of persistent microalbuminuria, but this only just achieved significance at the 5% level. More importantly there was a highly significant difference in baseline concentrations of plasma glucose and glycated haemoglobin between the two groups, but no difference in any other baseline variables tested. Glycated haemoglobin concentration did not change significantly in either the microalbuminuric or normoalbuminuric groups over the 10 year period (mean log 10 (SD) 1.112 (0.069) to 1.104 (0.103)% and 0.997 (0.076) to 1.012 (0.072)%, respectively).
—Comparison of baseline variables in 97 patients with insulin dependent diabetes mellitus grouped into those who developed persistent microalbuminuria (microalbuminuria) and those who did not (normalbuminuria) after 10 years of follow up. Values shown are means (SD) except for smoking where value is number of smokers and sex which is expressed as a ratio. Values shown for insulin dose, body mass index, blood pressure, and concentrations of plasma glucose, glycated haemoglobin and serum creatinine are based on mean of two separate baseline measurements for each patient
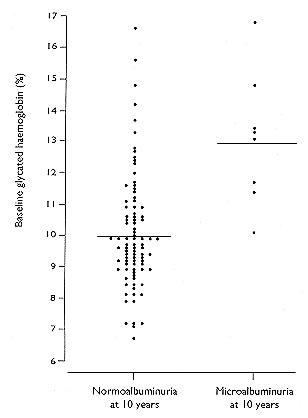
The figure shows the baseline values of glycated haemoglobin for each of the 97 patients according to whether they had or had not developed microalbuminuria by 10 years. Those who developed persistent microalbuminuria all had baseline glycated haemoglobin concentrations >10%—that is, higher than the mean value in those who did not develop microalbuminuria. The odds ratio of a patient developing microalbuminuria over 10 years if baseline glycated haemoglobin is >12% was 9.7 (95% confidence interval 2.1 to 45.8, P = 0.004).

Baseline glycated haemoglobin values in 97 patients with insulin dependent diabetes mellitus grouped according to development (microalbuminuria) or not (normoalbuminuria) of persistent microalbuminuria after 10 years of follow up. Normal glycated haemoglobin <7.5%. Horizontal lines in each group indicate mean value of glycated haemoglobin in that group (13.0% and 10.0%, respectively). Individual values show mean of two separate baseline measurements for each patient
{kind=link}
Determinants of the progression of albumin excretion over the 10 year period were investigated by multiple linear regression analysis by using the various baseline factors as explanatory variables and the mean of the three follow up albumin:creatinine ratio values in each patient as the outcome variable. The model shown (table III) indicates again that poor glycaemic control is significantly related to the progression of albumin excretion. There was also a weaker association of longer duration of diabetes with follow up albumin: creatinine ratio, but age at onset of diabetes did not show any significant association in this analysis. Baseline albumin:creatinine ratio showed a strong positive association with follow up albumin:creatinine ratio and was therefore also included in the model.
There was no significant association of any particular genotype for angiotensin converting enzyme with the development of microalbuminuria (with χ2 test) or with final albumin:creatinine ratio by using one way analysis of variance. To investigate this further we extended our analysis to include all 127 patients who were followed up after 10 years. Data on genotype for angiotensin converting enzyme were available for 104 of these patients. Nineteen of these had evidence of measurable nephropathy, ranging from persistent microalbuminuria as defined above to overt renal failure. Table IV shows the prevalence of the various genotypes for angiotensin converting enzyme in those with and without nephropathy compared with a control group of 364 men without diabetes. Again there was no significant association of genotype with the development of nephropathy nor was there any difference in the prevalence of the various genotypes between the subjects without diabetes and the patients with and without nephropathy either by χ2 test or one way analysis of variance.
—Genotypes for angiotensin converting enzyme in 104 patients with insulin dependent diabetes with (nephropathy) and without (normoalbuminuria) evidence of renal disease at 10 year follow up visit compared with group of 364 men without diabetes
Discussion
This prospective study has clearly shown that poor glycaemic control is a major determinant of progression from very low rates of urinary albumin excretion to microalbuminuria in patients with insulin dependent diabetes mellitus. The strength of this study lies in the long period of follow up, the strict definition of microalbuminuria, the well defined clinical characteristics, and the wide spectrum of variables studied. The shortcomings are that the patients were highly selected, and the conclusions drawn may not be applicable to other groups particularly those with non-insulin dependent diabetes. In addition, patients who are not attending an outpatient clinic for whatever reason are more likely to develop microalbuminuria21 and therefore our study may have underestimated the incidence of this. Our cumulative incidence of 8.2%, however, is broadly similar to that seen in other longitudinal investigations.7 8 9 10
There are few prospective studies investigating determinants of microalbuminuria, and these have shown conflicting results. The microalbuminuria collaborative study group found blood pressure, glycated haemoglobin concentration, and smoking to be determinants of microalbuminuria in a cohort of 137 patients followed up over four years.7 The baseline cut off for albumin excretion in this study was 30 μg/min. Although this is the rate above which microalbuminuria has been shown conclusively to predict overt renal disease, rates of >15 μg/min, which is still above the albumin excretion rate in normal subjects,22 may also predict overt nephropathy.5 Thus the collaborative group may have included some subjects who already had some degree of microalbuminuria and therefore an early rise in blood pressure as a consequence of the renal damage associated with this.10
We did not find any association of either systolic, diastolic, or mean arterial blood pressure with the development or progression of microalbuminuria. In fact, as can be seen from table II, the mean arterial blood pressure at baseline was slightly lower in the group who developed microalbuminuria. Patients with overt hypertension were excluded from both our study and that of the microalbuminuria collaborative group. Our study, however, was carried out over a longer period and more importantly had a much lower albumin:creatinine ratio (arithmetic mean 0.79 versus 2.57 mg/mmol) at entry, and so we are less likely to have included patients who already had early but perhaps appreciable nephropathy initiating an increase in blood pressure. In support of our findings Mathiesen et al also found that baseline concentration of glycated haemoglobin was higher in those who subsequently developed microalbuminuria over the ensuing five years but that an increase in blood pressure occurred only after the development of a considerable increase in urinary albumin excretion.10 In this latter study subjects had a higher blood pressure of 100 mm Hg at entry, and it was therefore more likely to pick up an effect of blood pressure as an initiating factor. This group also chose a fairly low albumin excretion rate at entry (<30 mg/24 hours) so again were less likely than the collaborative group to have included patients who already had microalbuminuria. A further study by Rudberg et al in children with insulin dependent diabetes showed poor glycaemic control but not blood pressure to be a determinant of microalbuminuria.9
It is interesting that we and others7 have found that initial albumin excretion is significantly related to follow up albumin excretion. This may be an indication that even at the very low levels of albuminuria used as entry criteria in these studies the pathological process leading to eventual overt diabetic nephropathy may have already begun. Long duration of diabetes and young age at onset also seem to have some predictive value for the development of microalbuminuria both in our study and those of others.7 9 10
Although we found glycaemic control to be an important predictor of the development of microalbuminuria, it is known that about 60-70% of patients with insulin dependent diabetes mellitus will not develop nephropathy. Even in the presence of long duration of diabetes and poor long term glycaemic control there are those who seem to be protected against progressive nephropathy. The reason for this is not known but it may well involve an inherited factor, which either protects or predisposes certain patients to nephropathy when glycaemic control is poor. A family history of hypertension or vascular disease has been shown to be related to the risk of developing microalbuminuria and nephropathy.12 13 New lines of investigation have more recently shown that deletion polymorphism in the gene for angiotensin converting enzyme, which is associated with the highest circulating plasma concentrations of angiotensin converting enzyme, is a risk factor for ischaemic heart disease23 and furthermore that those homozygous for the insertion polymorphism may be protected against renal disease in diabetes.14 This is an attractive hypothesis given the suggestion that angiotensin converting enzyme inhibitors may have a specific role in protecting the kidney against damage in diabetes.24 We were, however, unable to show any relation of genotype for angiotensin converting enzyme with the development of microalbuminuria. This may have been because of the small numbers (eight) who developed microalbuminuria and so we extended our study for this purpose to look cross sectionally at any degree of nephropathy in 104 patients who were followed up at 10 years, but we still failed to find any significant relation of genotype to the development or otherwise of renal damage.
In conclusion, this 10 year prospective study of a cohort of patients with insulin dependent diabetes has shown that the progression of very low level albuminuria and the development of microalbuminuria is not determined by blood pressure of genotype for angiotensin converting enzyme but primarily by poor long term glycaemic control. These results add to the growing body of evidence implicating higher blood glucose concentrations as the main aetiological factor in the development of diabetic nephropathy and emphasise the need to strive for good glycaemic control.
This study was funded by Wessex Regional Health Authority and the Portsmouth microalbuminuria study research fund. PT is funded by the British Heart Foundation (RG16). We are grateful to Professor G Viberti for measuring urinary albumin concentrations and Dr D Rowe for measuring concentrations of urinary creatinine and glycated haemoglobin. We thank Dr G Miller and patients and staff of the Camberley General Practice for their cooperation.