Article Text

Abstract
BACKGROUND Biopsy specimens obtained from the gastro-oesophageal junction can reveal intestinal metaplasia in patients presenting for routine upper endoscopy. The site of biopsy may play a critical role in determining the dysplasia risk of a patient.
AIMS To evaluate prospectively the dysplasia risk in patients with intestinal metaplasia of the distal oesophagus or within the gastric cardia.
METHODS Patients with short segment Barrett's oesophagus (SSBO) and cardia intestinal metaplasia (CIM) were followed prospectively.
RESULTS 177 patients with SSBO were identified (mean age 62 years, range 38–82; 91% whites). Twenty prevalence cases of dysplasia in SSBO were detected: 17 low grade dysplasia (LGD), three high grade dysplasia (HGD). Seventy six patients with CIM were identified (mean age 67 years, range 37–81; 81% whites). A single prevalence case of LGD in CIM was detected. During follow up of 78 SSBO and 34 CIM patients, dysplasia developed in nine (seven LGD, two HGD) with SSBO and in one (LGD) with CIM. There were significant differences between the two groups with respect to age, ethnicity, dysplasia prevalence, and incidence. Time to dysplasia progression was significantly longer in CIM compared with SSBO patients. Of the five patients with SSBO and HGD, one developed adenocarcinoma of the oesophagus on follow up. No HGD or cancers have been detected over this time period in CIM patients.
CONCLUSIONS The dysplasia risk is significantly greater in SSBO than in CIM patients, indicating two potentially different clinical processes. Future studies should separate SSBO from CIM in order to enhance the understanding of the pathophysiology and malignant potential of each entity.
- high grade dysplasia
- low grade dysplasia
- metaplasia
- Barrett's oesophagus
- gastro-oesophageal reflux disease
Statistics from Altmetric.com
- high grade dysplasia
- low grade dysplasia
- metaplasia
- Barrett's oesophagus
- gastro-oesophageal reflux disease
Biopsy specimens obtained from the gastro-oesophageal junction (GOJ), in patients undergoing routine upper endoscopy, often reveal intestinal metaplasia. These specimens may have been obtained either from the distal oesophagus or immediately distal to the GOJ—that is, the gastric cardia. The gastric cardia is the most proximal part of the stomach that lies immediately distal to the GOJ. Intestinal metaplasia in the distal oesophagus and gastric cardia has been of great interest recently due to the rapidly rising cancer incidence in these locations.1-3 Carcinomas arising from the gastric cardia differ from those in the remainder of the stomach. They share common epidemiological characteristics with oesophageal adenocarcinoma and may originate from segments of intestinal metaplasia in the oesophagus—that is, Barrett's oesophagus.4
The traditional definition of Barrett's oesophagus included at least 3 cm of circumferential columnar lining in the distal oesophagus.5 However, the entity of short segment Barrett's oesophagus, defined as segments of intestinal metaplasia less than 3 cm in length, has been recently defined and well accepted in the literature.6 Intestinal metaplasia at the GOJ has been reported to vary from 5% to 25% in patients presenting for upper endoscopy.7-9 These series included patients with either a normal squamocolumnar junction or short segments of columnar appearing mucosa in the distal oesophagus. However, few studies separate the prevalence of intestinal metaplasia in the distal oesophagus from that in the gastric cardia.10-14
Short segment Barrett's oesophagus has been associated with gastro-oesophageal reflux disease (GORD), is typically detected in white men, and has the risk of dysplasia and carcinoma.15 16 However, the dysplasia risk of patients with cardia intestinal metaplasia is unclear. The goals of the current study were to define cardia intestinal metaplasia, separate it from short segment Barrett's oesophagus, and prospectively follow these patients for the development of dysplasia and adenocarcinoma.
Methods
PATIENT POPULATION
Patients were enrolled from the Kansas City VA Medical Center and Tucson VA Medical Center. The study was approved by the Human Subjects Committee of each medical centre. Written informed consent was obtained from each patient. The demographics of the patients, including the age, sex, and ethnicity, together with the dose and duration of acid suppressive medications were recorded.
DEFINITIONS
Short segment Barrett's oesophagus (SSBO) was defined as the presence of columnar appearing mucosa in the distal oesophagus less than 3 cm in length with intestinal metaplasia on biopsy. Cardia intestinal metaplasia (CIM) was defined as presence of intestinal metaplasia immediately distal to the GOJ. The GOJ was defined as the pinch at the end of the tubular oesophagus coinciding with the proximal margins of the gastric folds.17
ENDOSCOPY AND BIOPSY PROTOCOL
Upper endoscopy (oesophagogastroduodenoscopy, OGD) was performed in a standard manner using either an Olympus GIF-100 or GIF-1T100 endoscope (Olympus, Lake Success, New York, USA). The appearance of the squamocolumnar junction was carefully evaluated, noted, and recorded. The presence of irregular appearing Z lines, tongues, or segments of columnar lining mucosa in the distal oesophagus was also recognised, noted, and biopsied.
The biopsy protocol included obtaining four quadrant biopsy samples every 2 cm from the circumferential appearing Barrett's epithelium in the distal oesophagus. In patients with small or irregular tongues of columnar mucosa, at least two biopsy specimens from every centimetre length in the distal oesophagus were obtained. At least four biopsy specimens were obtained from the gastric cardia. All biopsy specimens were obtained using standard biopsy forceps.
HISTOLOGICAL ANALYSIS
All biopsy specimens were fixed in formalin, embedded in paraffin wax, and stained with haematoxylin and eosin in combination with alcian blue or using periodic acid Schiff (PAS) with alcian blue at pH 2.5. The diagnoses of SSBO and CIM were confirmed by the presence of goblet cells (staining deep blue) in the biopsy specimens obtained from the columnar appearing distal oesophagus and the gastric cardia, respectively. Dysplasia in the biopsy specimens was recognised by the presence of cytological and architectural abnormalities and was classified as no dysplasia, indeterminate/low grade dysplasia (LGD), and high grade dysplasia (HGD) based on the criteria established for inflammatory bowel disease.18 A single pathologist at each institution reviewed all biopsy specimens with no prior knowledge of the detailed clinical history of the patients.
FOLLOW UP ENDOSCOPY
Once the diagnosis of either SSBO or CIM was established, the patients were followed prospectively and underwent upper endoscopy with biopsies every year, using the biopsy protocol described earlier. Endoscopy was performed earlier if necessary, guided by patient's symptoms or the histological presence of dysplasia. For the purpose of this study, only patients with intestinal metaplasia on two consecutive OGD examinations at least six months apart were included in the follow up analysis.
STATISTICAL ANALYSIS
Fisher's exact test and the two samplet test were used to assess differences between SSBO and CIM patients for categorical and continuous variables, respectively. The log rank test was used to assess the difference in time to progression to dysplasia between SSBO and CIM patients. Three year actuarial probabilities of dysplasia development were calculated for the SSBO and CIM patients. All statistical comparisons were made at the 5% significance level.
Results
PATIENTS WITH SSBO
A total of 177 patients with SSBO was identified from both centres. The mean age of this patient group was 62 years (range 38–82). The majority (91%) of the patients were whites (162 whites, seven African Americans, seven Hispanics, and two native Americans). The mean length of Barrett's mucosa in this group was 1.4 cm (range 1–2.5 cm). Twenty cases of dysplasia in SSBO were detected at the initial endoscopy; including 17 patients with low grade dysplasia (LGD) and three patients with high grade dysplasia (HGD). The dysplasia prevalence in the SSBO group was 11.3% (table 1).
Clinical characteristics of patients with short segment Barrett's oesophagus (SSBO) and cardia intestinal metaplasia (CIM)
PATIENTS WITH CIM
Seventy six patients with CIM were identified from both centres. The mean age of this group was 67 years (range 37–81). This included 81% whites and 16% African Americans (62 whites, 12 African Americans, and two Hispanics). The CIM patients were older (p=0.0045) and had a higher percentage of African Americans (p=0.0028) than the SSBO patients (table 1). Only one patient was detected with dysplasia at initial endoscopy (LGD)—a prevalence of 1.3%. Dysplasia prevalence was statistically higher (p=0.0058) in the SSBO patients (11.3%) than in the CIM patients (1.3%).
FOLLOW UP OF PATIENTS WITH SSBO AND CIM
A total of 78 patients with SSBO (documented intestinal metaplasia on two separate occasions) have undergone repeat endoscopy with biopsy. The mean follow up of this group was 31 months (range 8–100 months). Thirty four patients with CIM (intestinal metaplasia on two separate occasions) were followed prospectively for a mean of 24 months (range 6–80 months).
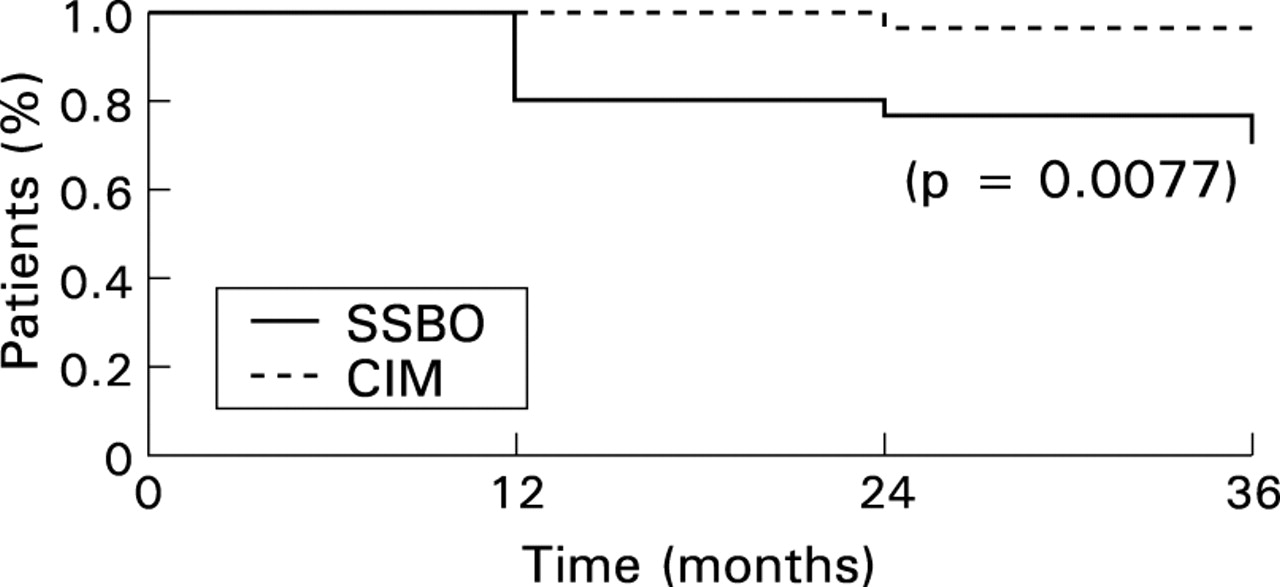
During follow up of SSBO patients, dysplasia developed in nine patients (seven LGD, two HGD). Table 2 shows the demographics and clinical features of SSBO patients with dysplasia. However, only one patient in the CIM group developed LGD. The dysplasia incidence in SSBO patients was 4.6% per year compared with 1.5% per year in CIM patients. The time to dysplasia development (fig 1) was significantly longer (p=0.0077) in CIM patients compared with SSBO patients (per log rank test). Based on actuarial probabilities, only 4.2% of the CIM patients compared with 31% of the SSBO patients had developed dysplasia within three years.
Characteristics of patients with short segment Barrett's oesophagus (SSBO) and dysplasia

Dysplasia free interval. SSBO, short segment Barrett's oesophagus; CIM, cardia intestinal metaplasia.
Of the 29 patients with dysplasia in SSBO, 25 have been followed up. Of the five patients with SSBO and HGD (fig 2), one developed adenocarcinoma of the oesophagus over 24 months. No HGDs or cancers were detected in CIM patients during follow up.

{kind=link}
{kind=link}
Outcome of dysplasia in patients with short segment Barrett's oesophagus. HGD, high grade dysplasia; LGD, low grade dysplasia
The patient who developed dysplasia in the CIM group was a 64 year old white man who had evidence of LGD on his second endoscopy, one year after the initial diagnosis. He had evidence ofHelicobacter pylori infection, did not undergo eradication therapy, and on his third endoscopy had persistent CIM but no evidence of dysplasia.
PATIENTS WITH BOTH SSBO AND CIM
From the study population, 10 patients were identified who had evidence of both lesions (SSBO and CIM). The patients in this group were all men, mean age was 63 years (range 48–73), and the mean length of Barrett's oesophagus was 1.4 cm. Three of these 10 patients had evidence of dysplasia (two LGD, one HGD) in their oesophageal intestinal metaplasia without dysplasia in their cardia.
Discussion
Detection of intestinal metaplasia in the distal oesophagus as well as within the gastric cardia is being reported with increasing frequency. The prevalence of SSBO has been reported to vary from 2% to 12% and that of CIM from 5% to 23% in patients undergoing routine upper endoscopy. The detection of intestinal metaplasia in the distal oesophagus (Barrett's oesophagus) potentially commits the patient to regular surveillance endoscopy with biopsy. The incidence of adenocarcinoma in patients with Barrett's oesophagus is estimated to be 30–50 times that of the general population19 and is on the increase. However, the exact incidence of cancer in patients with SSBO is unknown, and the role of CIM as a premalignant lesion is still unclear.
This study prospectively evaluated two well defined groups of patients for the development of dysplasia and/or adenocarcinoma of the oesophagus and the gastric cardia. The prevalence and incidence of dysplasia were significantly higher in the SSBO group compared with the CIM group (11.3% and 4.6% versus 1.3% and 1.5% respectively). Significant age, ethnic, and sex differences were also noted between the two groups. Is a comparison between these two groups valid and what are the implications of this study? SSBO and CIM patients were defined prospectively by standardised criteria at the two medical centres with a long standing interest in these entities. No consenting patients meeting the study criteria were excluded from the analysis. The demographics and dysplasia risk of patients with SSBO are different from those in CIM patients; indicating two distinct lesions with possibly separate pathophysiologies. The prevalence of dysplasia in SSBO patients in this study is comparable to that recently reported (8%) in a group of well defined patients evaluated prospectively.14 The dysplasia risk was significantly different between SSBO and CIM patients during a relatively short follow up period but future studies with larger patient numbers and longer follow up are needed to validate these results.
Why is it important to separate SSBO from CIM and are they different entities? The distinction between intestinal metaplasia in the distal oesophagus versus the gastric cardia has not been well characterised, but recently a few studies have shed light on this issue. Recent data suggest that the aetiology of CIM is more likely to be secondary toH pylori infection rather than GORD. Goldblum et al studied patients with carditis (inflammation in the gastric cardia) and CIM.20This study found that H pylori infection was closely associated with both carditis and CIM and that CIM was associated with H pylori carditis as well as intestinal metaplasia in other parts of the stomach. There also seems to be a variance in the prevalence of SSBO and CIM based on different ethnic groups being evaluated. The prevalence of CIM has been shown to be equally prevalent in African Americans and whites; whereas Barrett's oesophagus is significantly more prevalent in whites.12 This difference may be secondary to a difference in pathophysiology and/or genetics.
Dias Pereira et al evaluated the prevalence of intestinal metaplasia in patients with columnar lining in the distal oesophagus and in those with a normal appearing squamocolumnar junction.21 This study included patients with SSBO and CIM. Reflux symptoms as well as erosive oesophagitis were more frequent in patients with SSBO than in CIM patients, indicating that GORD may be a possible cause of SSBO. Patients with SSBO had a higher male:female ratio (2.8:1), which is very similar to long segment or traditional Barrett's oesophagus. As opposed to SSBO, patients with CIM were predominantly women and had a lower frequency of GORD symptoms.
Recently Hackelsberger et al studied 23 patients with SSBO and 42 with CIM.22 The prevalence of CIM in the entire study group was 13.4% and was significantly associated with older age, H pylorigastritis, and intestinal metaplasia elsewhere in the stomach. SSBO patients, on the other hand, were more likely to be men with evidence of GORD symptoms, erosive oesophagitis, but no association withH pylori or gastric intestinal metaplasia. Thus, CIM is a relatively common finding if biopsy specimens are obtained from below a normal squamocolumnar junction and occurs mainly in older H pylori infected men who also have evidence of multifocal gastric intestinal metaplasia. In a recent study, the demographics and dysplasia/cancer prevalence were studied in 45 CIM, 64 SSBO, and 40 patients with long segment Barrett's oesophagus.14 Patients with SSBO were predominantly white men with GORD symptoms. In contrast, patients with CIM were similar in sex and ethnicity to the control group and had a higher prevalence ofH pylori infection. Dysplasia or cancer was noted in 10% of SSBO and 6.4% of CIM patients.
There is an increasing body of evidence to suggest that intestinal metaplasia in the region of the GOJ may comprise two distinct entities: SSBO (intestinal metaplasia in the distal oesophagus); and CIM (intestinal metaplasia in the gastric cardia). The dysplasia risk, as shown by our study, is significantly different between these groups of patients. The most important finding in this study is the lower prevalence and incidence of dysplasia in CIM patients, even though they were significantly older than SSBO patients. The cancer risk associated with CIM remains unclear and although there is a potential association of CIM with cardia cancer, it seems to be very low, given that CIM is a very common finding. The concepts of SSBO and CIM are still evolving and confusion arises from the use of different terminologies, perhaps due to the difficulty in precisely defining the exact junction between the stomach and the oesophagus. This is particularly true in patients with large hiatal hernias, erosive oesophagitis, strictures, postfundoplication, or tumours at the GOJ.
The metaplasia−dysplasia−adenocarcinoma sequence is well defined for intestinal metaplasia of the distal oesophagus (Barrett's oesophagus), but not for intestinal metaplasia of the gastric cardia. The demographics of SSBO patients include elderly white men with associated GORD symptoms, whereas CIM may be equally prevalent in men and women, with no ethnic predilection. Patients undergoing upper endoscopy for reflux symptoms and found to have short tongues of columnar appearing mucosa should have these tongues biopsied. If these biopsies reveal intestinal metaplasia, the diagnosis of SSBO is confirmed. However, there is lack of information on the cancer risk of CIM patients and thus the taking of biopsy specimens at or below a normal appearing squamocolumnar junction is not currently recommended. Future larger prospective studies should separate SSBO from CIM in order to enhance our understanding of the pathophysiology and the malignant potential of each clinical entity. The possible role of intestinal metaplasia as a premalignant lesion of cardia cancer is not yet clear and our series indicates a very low prevalence and incidence of dysplasia within CIM. Thus, surveillance of CIM is not recommended aside from study protocols.
Acknowledgments
This work was presented as DDW Poster of Distinction at the Digestive Diseases Week, May 1999, Orlando, Florida, USA.
References
Footnotes
- Abbreviations used in this paper:
- CIM
- cardia intestinal metaplasia
- GOJ
- gastro-oesophageal junction
- GORD
- gastro-oesophageal reflux disease
- HGD
- high grade dysplasia
- LGD
- low grade dysplasia
- LSBO
- long segment Barrett's oesophagus
- OGD
- oesophagogastroduodenoscopy
- SSBO
- short segment Barrett's oesophagus