Article Text

Abstract
BACKGROUND The CD44 variant (CD44v) isoforms have been noted as markers for tumour metastasis and prognosis in several adenocarcinomas.
AIMS To investigate whether CD44v, especially the CD44v2 (v2) isoform, may be a useful prognostic factor for patients with oesophageal squamous cell carcinoma, using a recently developed monoclonal antibody against a v2 epitope.
PATIENTS 233 patients (211 men and 22 women; mean age 61.9 years), with oesophageal squamous cell carcinomas curatively removed without additional treatment between 1987 and 1996 at the National Cancer Center Hospital, were analysed for CD44v expression.
METHODS The expression of CD44v was evaluated immunohistochemically using monoclonal antibodies against epitopes of the standard and variant protein, in paraffin embedded oesophageal squamous cell carcinoma tissue from 233 patients who had undergone cervical, mediastinal, and abdominal lymphadenectomy (three field dissection) for oesophagectomy. The data were evaluated for any correlation with clinicopathological indices or prognosis.
RESULTS Although total CD44 and CD44v6 (v6) were respectively observed in 99% and 97% of the cancer specimens, the expression of v2 was only 30%. Patients whose tumours were v2 positive had a significantly better prognosis than those whose tumours were v2 negative (p = 0.031). Furthermore, in patients without lymph node metastasis, v2 positivity alone was a significant independent factor of prognosis (relative risk of death associated with v2 negativity, 4.7; p = 0.037) in multivariate analysis.
CONCLUSIONS These results indicate that v2 is a useful marker for clinical prognosis in patients with oesophageal squamous cell carcinoma. Particularly in patients without lymph node metastasis, v2 status may thus have implications for the use of adjuvant chemotherapy and/or radiotherapy in patients with oesophageal cancer at an early stage.
- CD44 variants
- oesophageal squamous cell carcinoma
- metastasis
- prognosis
- immunohistochemistry
Statistics from Altmetric.com
CD44 is a heavily glycosylated cell surface molecule which is involved in cell-cell and cell-matrix interactions1 2 and mediates several functions, such as extracellular matrix cell adhesion,3 4 lymphocyte homing,5 6 T cell activation,7 and tumour metastasis.7 8 The CD44 family of polymorphic transmembrane glycoproteins is encoded by a complex gene7 9-12 which occupies a stretch of 60–80 kb assigned to the human chromosomal locus 11p13. Its human form is composed of at least 21 exons, 10 of which are constitutively expressed on almost all cell types, to produce a heavily glycosylated 85–90 kDa isoform known as standard form CD44. The remaining exons can be alternatively spliced in various combinations, and their products are incorporated into the polypeptide backbone encoded by the standard form exons. This results in a large array of protein isoforms (CD44v), which are differentially expressed in various tissues and at various stages in development.13 14
It was recently shown that the expression of v6, one variant isoform of CD44, distinguished metastatic from non-metastatic pancreatic carcinoma cell lines in the rat.8 Evidence that v6 itself has a role in metastasis came from the demonstration that transfection with cDNA encoding this isoform converted non-metastatic carcinoma rat cells into metastatic cells.8 Although the functions of CD44v isoforms in humans remain unclear, it is thought that they play an important role in the growth and metastasis of several kinds of tumours.15-19 However, there have been no reports on the relation between CD44v expression and oesophageal cancer. We analysed the correlations between clinicopathological indices and immunohistochemical staining of surgical specimens curatively resected from oesophageal squamous cell carcinomas, using anti-v6 antibody. In addition, we evaluated whether monoclonal antibody against an epitope encoded by exon 7 (v2)20 could be a prognostic factor, because several molecular biological studies have indicated that abnormal expression of v2 occurs in various types of human malignancies21 22 and no study has yet evaluated it in human oesophageal cancer.
Materials and methods
PATIENTS AND TISSUE SPECIMENS
Samples of formalin fixed paraffin wax embedded tumour tissue were examined from 233 oesophageal squamous cell carcinomas curatively removed without additional treatment between 1987 and 1996 at the National Cancer Center Hospital, Tokyo. All patients underwent cervical, mediastinal, and abdominal lymphadenectomy (three field dissection)23 for oesophagectomy, and were classified according to the tumour, node, metastases (TNM) classification24 based on the pathological reports. The pathological stage (pTNM) of each patient was defined at the time of operation. The patients included 57 of pTNM stage I, 108 of stage II, and 68 of stage III. The 211 men and 22 women had a median age of 61 (range 40–86) years. The median follow up period was 33.7 (range 2–117) months.
ANTIBODIES AND IMMUNOHISTOCHEMICAL ANALYSIS
Sections (3 μm) were cut on silane coated glass slides (Muto Pure Chemicals, Tokyo, Japan), deparaffinised in xylene, dehydrated through a graded series of ethanols, and washed in running water. They were then treated with Serotec target unmasking fluid (STUF; Serotec, Oxford, UK) for 10 minutes in a 600 W microwave oven and left to cool for 15 minutes. They were rinsed in two changes of deionised water and phosphate buffered saline, and preincubated with 20% normal rabbit serum in Tris buffered saline at 37°C for 60 minutes. After being washed with Tris buffered saline, separate sections were incubated with the primary monoclonal antibodies 2C5 (3.3 μg/ml; R&D Systems, Abingdon, Oxon, UK), 2F10 (10 μg/ml, R&D Systems), or M23.6.120 (20 μg/ml), which recognise epitopes of the CD44s, v6, and v2 portions respectively, in 1% normal rabbit serum diluted with Tris buffered saline at 4°C overnight in a wet box and then at 37°C for 10 minutes the next morning. After the primary antibody treatment, endogenous peroxidase activity was blocked with 0.3% H2O2 in methanol at 4°C for 10 minutes, and the sections were incubated with a 1:400 dilution of biotinylated anti-mouse IgG (Dako, Santa Barbara, California, USA). This was followed by incubation with horseradish peroxidase conjugated avidin-biotin complex (ABComplex; Dako) at room temperature for 60 minutes. Immunostaining was visualised with 3,3'-diaminobenzidine (Sigma, St Louis, Missouri, USA) for 20 minutes, and the reaction was stopped by washing with water. Finally, the sections were counterstained with Mayer's haematoxylin. Between all antibody incubations, they were washed three times for five minutes with Tris buffered saline on a shaking platform. Negative controls included sections treated with 1% normal rabbit serum alone in place of the primary antibody.
The status of CD44s and CD44v was assessed in a coded manner without knowledge of the clinical and pathological features of the case or the clinical outcome. Levels of CD44 protein expression were graded into four subgroups: (a) no detectable expression; (b) faint expression detected in <5% of tumour cells; (c) strong heterogeneous or localised expression in >5% of tumour cells, indicating immunopositive subpopulation; (d) strong homogeneous expression in >50% of tumour cells. For practical and statistical purposes, subgroups (a) and (b) were combined into the group designated “negative”, and subgroups (c) and (d) were combined into the group designated “positive”.
STATISTICAL ANALYSIS
Staining results were compared in all cases with clinicopathological features, including sex, age, pTNM classification, histological grading, vessel invasion, and survival. Each lesion was graded histologically according to the World Health Organisation classification.25 The correlation between CD44 peptide expression and clinicopathological indices was analysed by Fisher's exact test. We defined overall survival as survival from the date of surgery until 26 December 1996. The primary determinant in this study was survival time, as measured from the date of surgery until the time of the last follow up visit or death. Survival curves for 233 patients were constructed according to the Kaplan-Meier method,26and the differences between the curves were calculated. The p value was calculated by the log rank analysis. The prognostic significance of individual parameters in multiparametric analyses was determined by using Cox's proportional-hazards model.27 A p value of less than 0.05 was considered significant.
Results
IMMUNOHISTOCHEMICAL STAINING
All 233 oesophageal squamous cell carcinomas were stained with three monoclonal antibodies directed against the total CD44 (CD44v as well as CD44s), v6 (exon 11), and v2 (exon 7). Moreover, normal oesophageal mucosa adjacent to cancer tissue was examined for reactivity with the same antibodies. All normal squamous epithelium displayed uniform staining for total CD44, v6, and v2 in the prickle cell and basal cell layers (fig 1A–C). Normal mucosa adjacent to the cancer tissue provided positive internal controls for reliably assessing the presence or absence of CD44 immunoreactivity in the squamous cell carcinomas. Total CD44 and v6 were observed in 99% (231 of 233) and 97% (226 of 233) of the cancer specimens respectively (fig2A,B). The high immunoreactivity to total CD44 and v6 was not only shown in normal squamous epithelium but also in cancer tissue. In contrast, the expression of v2 in the cancer tissue was only 30% (70 of 233). The intensity of v2 staining was generally weaker than that of total CD44 and v6 staining. Reactivity with all the CD44 specific antibodies was localised mainly on the tumour cell membranes, and some cells showed positive staining in the cytoplasm of the cells, especially in the case of CD44 v2. Table 1 summarises the v2 staining status of the 233 patients.
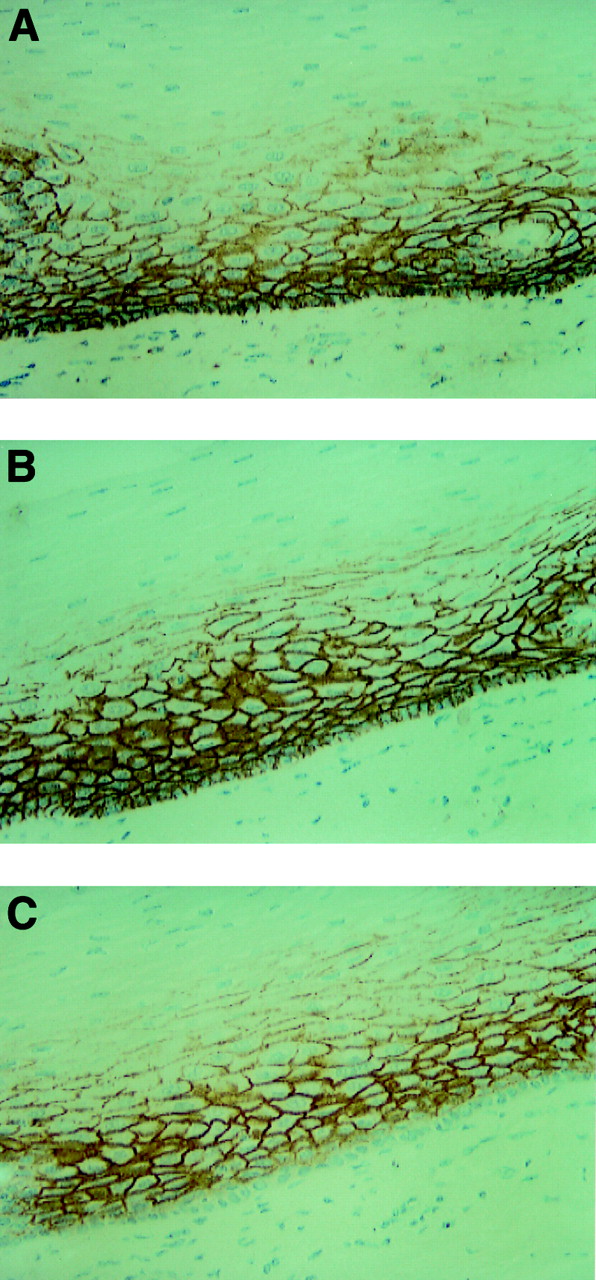
Immunohistochemistry of the adjacent normal squamous epithelium. (A) All normal squamous epithelium displayed uniform staining for total CD44 in the prickle cell and basal cell layers. v6 (B) and v2 (C) were also observed in the prickle cell and the basal cell layers. Normal mucosa adjacent to the cancer tissue provided positive internal controls for reliably assessing the presence or absence of CD44 immunoreactivity in the squamous cell carcinomas. Original magnification × 200.

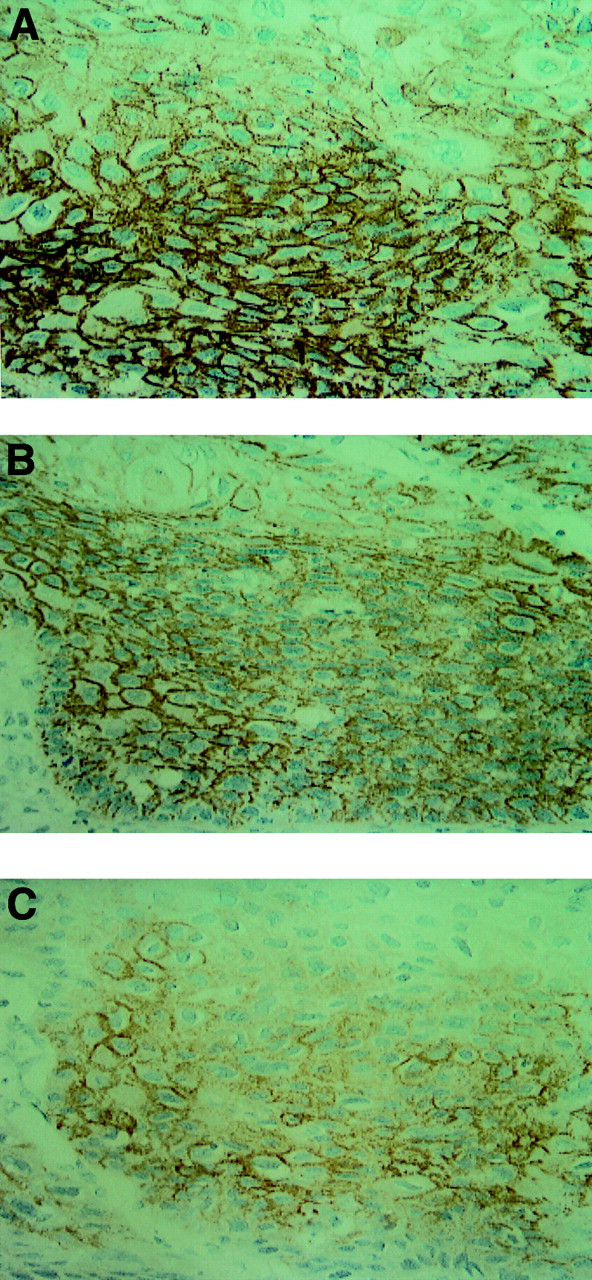
Immunohistochemistry of squamous cell carcinoma. Total CD44 (A) and v6 (B) were observed in 99% (231 of 233) and 97% (226 of 233) of the cancer specimens respectively. In contrast, the expression of v2 (C) in the cancer tissue was only 30% (70 of 233). The intensity of v2 staining was generally weaker than that of total CD44 and v6 staining. Original magnification × 400.
Correlation between CD44v2 status and clinicopathological indexes
CORRELATION BETWEEN THE EXPRESSION OF V2 AND CLINICOPATHOLOGICAL INDICES
Table 1 gives the relevant clinical characteristics of the 233 patients whose tumours were analysed immunohistochemically. Neither sex nor age correlated with positivity for v2 (p = 0.96 and 0.71 respectively). Also, there was no significant correlation between the expression of v2 and other clinicopathological indices such as histological grading, vessel invasion, pT classification, pN classification, or pTNM stage. The median follow up period was 34.0 months for patients with v2 positive tumours and 34.9 months for those with v2 negative tumours (p = 0.93).
EXPRESSION OF V2 AND PROGNOSIS
The relation between the expression of v2 and survival rate was examined in 233 curatively resected oesophageal squamous cell carcinomas during a follow up period of 2–117 months (median 33.7 months). Figure 3 shows survival curves of patients, stratified according to v2 status. Patients whose tumours were v2 positive had a significantly better prognosis than those whose tumours were v2 negative (p = 0.031). The five year survival rate for patients with v2 positive tumours was 72.4%, whereas the rate was 43.8% for patients with v2 negative tumours. At the conclusion of the study, 51 of 70 patients with v2 positive tumours (73%) were alive, compared with 84 of 163 patients (52%) with v2 negative tumours (p = 0.004). In multivariate analysis with Cox's proportional hazards model, v2 status was an independent prognostic factor (relative risk of death associated with v2 negativity, 2.0; p = 0.008) in all patients studied. However, the hazard ratio was lower than that of pT classification (relative risk of death associated with pT2 and 3, 2.3; p = 0.003) or pN classification (relative risk of death associated with pN1, 2.6; p<0.001). Other indices such as age, sex, histological grading and vessel invasion were not significant independent indicators of prognosis.

Survival curves of all patients studied according to v2 status. Patients whose tumours were v2 positive had a significantly better prognosis than those whose tumours were v2 negative (log rank test; p = 0.031). The five year survival rate for patients with v2 positive tumours (median follow up period 34.0 months) was 72.4%, whereas it was 43.8% for patients with v2 negative tumours (median follow up period 34.9 months).
Figure 4 shows survival curves for patients without lymph node metastasis according to v2 status. As in the data from node negative patients studied, patients whose tumours were v2 positive had a significantly better prognosis than those whose tumours were v2 negative (p = 0.022). The five year survival rate for patients with v2 positive tumours (median follow up period 45.9 months) was 83.8%, whereas the rate was 65.1% for patients with v2 negative tumours (median follow up period 43.0 months). In contrast with the data from all patients including node positivity and negativity, the multivariate analysis with Cox's proportional hazards model showed that only v2 status was an independent prognostic factor (relative risk of death associated with v2 negativity, 4.7; p = 0.037) in the patients without lymph node metastasis. However, pT classification, histological grading, and vessel invasion were not significant prognostic indicators. Tables 2 and 3 give the maximum likelihood estimated from the multivariate analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival curves of patients without lymph node metastasis according to v2 status. Patients whose tumours were v2 positive had a significantly better prognosis than those whose tumors were v2 negative (log rank test; p = 0.022). The five year survival rate for patients with v2 positive tumours (median follow up period 45.9 months) was 83.8%, whereas it was 65.1% for patients with v2 negative tumours (median follow up period 43.0 months).
Multivariate analysis with Cox's proportional hazards model for CD44v2 status and clinicopathological indexes in all patients studied
Multivariate analysis with Cox's proportional hazards model for CD44v2 status and clinicopathological indexes in patients without lymph node metastasis
Discussion
Recent clinicopathological studies have disclosed that the expression of individual variant exons is associated with poorer prognosis in several adenocarcinomas—for example, that of exon 14 (v9) is increased in gastric adenocarcinoma,28 that of exon 11 (v6) in the colon, breast,29 30 and pancreas,22 31 32 and that of exon 7 (v2) in the pancreas21 and breast.22 On the other hand, several reports have provided data indicating that CD44 expression is associated with longer survival in neuroblastoma33 and that decreased expression of v6 correlates with decreased survival in laryngeal squamous carcinoma34 and tumours of squamocellular origin.35 It is difficult to interpret this large body of information and to compare the various studies. However, we can infer from many reports published previously that the promoter and splice control is strictly regulated in normal cells in an organ specific manner, whereas the strict promoter and splice control is lost or changed in many human cancers. To date, there have been no reports on correlations between clinicopathological indices and CD44v in oesophageal cancer. On the basis of this background, we studied the correlation between the expression of CD44v, especially v2, and survival of patients with squamous cell carcinoma.
In our study, all normal squamous epithelium displayed uniform staining of total CD44, v6, and v2 in the prickle cell and the basal cell layers. This result was consistent with other data for tumours of squamocellular origin.33-35 Whereas total CD44 and v6 were observed in 99% and 97% of the cancer specimens respectively, the expression of v2 in the cancer tissue was only 30%. Furthermore, the intensity of v2 immunoreactivity was generally weaker than that of total CD44 and v6. Also, no significant association was found between the expression of v2 and clinicopathological indices of patients, including all stages. Concerning prognosis, patients with v2 positive tumours had a longer survival time than those with v2 negative tumours (p = 0.031). This result suggested that downregulation of v2 was associated with a poor prognosis in patients with oesophageal squamous cell carcinoma. In multivariate results of all patients studied, whereas v2 status was an independent prognostic factor (relative risk of death associated with v2 negativity, 2.0; p = 0.008), the hazard ratio was lower than that of pT classification or pN classification. As expected, the pN classification was an important prognostic factor36-38 (relative risk of death associated with pN1, 2.6; p<0.001).
We then evaluated the association between v2 status and prognosis in the patients without lymph node metastasis, which was the most useful prognostic factor. The result showed not only that v2 positivity gave a significantly better prognosis (p = 0.022) but also that v2 negativity was predictive of mortality (relative risk of death associated with v2 negativity, 4.7; p = 0.037) in the group of node negative patients. Other indices such as pT classification, pTNM stage, histological grading, and vessel invasion were not significant prognostic indicators.
To predict future development of metastasis is of great importance, as patients in such categories may benefit from adjuvant chemotherapy and/or radiotherapy. However, there has been no clear prognostic marker for patients without lymph node metastasis. Our findings here therefore seem to be quite important, because v2 status may assist in determining whether adjuvant therapy should be given to patients with oesophageal squamous cell carcinoma at an early stage.
Acknowledgments
We thank Miss S Nakadaira and Miss K Kobayashi for technical assistance and Miss H Orita for preparing the manuscript. This work was supported in part by the Grants-in-Aid for Cancer Research from the Ministry of Health and Welfare, Japan, the Japanese Foundation for Multidisciplinary Treatment of Cancer, and the Research Fund for Digestive Molecular Biology.
References
Footnotes
- Abbreviations used in this paper:
- CD44s
- CD44 standard
- CD44v
- CD44 variant
- CD44v2
- CD44 variant 2
- CD44v6
- CD44 variant 6