Article Text

Abstract
Background—Helicobacter pylori species comprise different strains, cytotoxic and non-cytotoxic, which can be identified on the basis of their genomic pattern.
Aims—(1) To evaluate the polymorphism of the vacA gene and to ascertain whether thecagA gene is present in patients with gastric adenocarcinoma. (2) To study the anti-H pylori antibody profile using western blotting.
Patients—Twenty one patients with gastric adenocarcinoma and 71 with H pyloriassociated benign disease (nine gastric ulcer, 29 duodenal ulcer, 25 antral gastritis, and eight duodenitis).
Methods—The polymerase chain reaction was used to verify the presence or absence ofcagA and to study the polymorphism of vacA in gastric mucosal samples obtained during endoscopy for patients with benign diseases and at surgery for patients with gastric adenocarcinoma. Fasting sera were used to assess anti-H pylori antibodies against different H pyloriantigens by western blotting.
Results—cagAgene and the allele s1 of vacAwere significantly less frequent in patients with antral gastritis (60% and 60%) compared with patients with gastric adenocarcinoma (94% and 100%) and with other non-malignant gastroduodenal diseases (93% and 87%) (χ2=16.01, p<0.001; and χ2=13.97, p<0.01). In patients with gastric adenocarcinoma, antibodies against a 74 kDa H pylori antigen were less frequently found than in patients with benign diseases.
Conclusions—H pylori infection caused bycagApositive/vacA s1 strains is a frequent finding in patients with gastric adenocarcinoma. Prospective studies are needed to confirm whether the low incidence of positive serological response to the 74 kDa H pyloriantigen in patients with gastric adenocarcinoma is important.
- Helicobacter pylori
- western blot
- cagA
- vacA
- gastric adenocarcinoma
Statistics from Altmetric.com
Epidemiological studies on large series show thatHelicobacter pylori is a group 1 carcinogen for gastric adenocarcinoma, which is one of the most frequent cancers worldwide, the odds ratio for developing gastric cancer being 3.8 to 8.7 in H pylori infected subjects.1-9 The pathophysiological mechanism by whichH pylori could lead to gastric cancer has not yet been defined, although many hypotheses have been put forward.1 ,5 ,8-14 It has been suggested thatH pylori may favour the transformation of normal mucosal cells into cancer cells as it promotes cell replication and also chronic mucosal inflammation with a wide polymorphonuclear infil- trate.15-18 Furthermore the reduced mucosal ascorbic acid content and increased lipid peroxidation present inH pylori infected patients may contribute to gastric carcinogenesis.19-21
H pylori infection can also cause gastric and duodenal ulcer, type B chronic gastritis, and gastric MALToma.22-24 The wide spectrum of diseases associated with H pylori infection may depend on the heterogeneity of H pylori, and/or the heterogeneity of the host response to the same H pylori strain.
Of the two main H pylori strains, type I produces a vacuolating cytotoxin, whereas type II usually does not.25 The genome of almost all type I strains has a gene coding for CagA, a highly immunogenic, high molecular weight protein, which is not present in most type II strains. The gene coding for the vacuolating cytotoxin, vacA, is polymorphic and present in all strains. The polymorphism ofvacA, mainly located in the region coding for the signal peptide (s) and in the mid portion of the gene (m), accounts for the phenotypic differences between type I and type II strains: both types synthesise a VacA protein, which is active as a vacuolating cytotoxin in type I, and inactive in type II strains.25 ,26
The immunological host response to H pylori infection is characterised by the production of antibodies, which are easily detected in sera. Currently available methods, which use antigen preparations derived from sonicated or lysed bacteria, enable the detection of serum antibodies against a pool ofH pylori antigens.2 ,4 ,18 ,27More recently, the immunological response towards the CagA protein has been assayed using enzyme linked immunosorbent assay (ELISA) procedures.12-14 ,25 ,28 However, little is known about the serological response to the different H pylori antigens in patients with benign or malignant gastroduodenal H pylori associated diseases.
Our aims were therefore: (1) to evaluate the frequency ofcagA and of the alleles s1, s2, m1, and m2 ofvacA in patients with gastric adenocarcinoma, comparing findings with those in control patients with benign gastroduodenal diseases; and (2) to study, in the same patients, the anti-H pylori antibody profile using western blotting.
Materials and methods
In total, 92 patients from the north east of Italy were enrolled in the study. Of these, 21 (13 men, eight women; aged 31–84 years) had gastric adenocarcinoma (located in the upper third of the stomach in four, in the middle third in nine, and in the lower third in eight patients). Tumours were stage I in three cases, stage II in two, stage III in 12, and stage IV in four. In all patients a histological confirmation of the diagnosis of adenocarcinoma was obtained using samples taken intraoperatively. Two tissue samples, obtained from the neoplastic area and from the adjacent (at least 3 cm) non-neoplastic mucosa, were stored at −80°C until DNA extraction. Gastric juice was not available for these patients.
The reference controls were 71 patients with benign gastroduodenal diseases, chosen on the basis of the presence ofH pylori (histological assessment by staining with Giemsa and/or Whartin Starry); all underwent upper gastrointestinal endoscopy. The diagnoses, made on the basis of clinical history and endoscopic and histological findings, were: benign gastric ulcer (nine patients: seven men, two women; aged 44–73 years); duodenal ulcer (29 patients: 18 men, 11 women; aged 27–72 years); antral gastritis (25 patients: 11 men, 14 women; aged 28–79 years); and duodenitis (eight patients: seven men, one woman; aged range 24–70 years). Gastric and duodenal ulcers were noted at endoscopy; the benign nature of the gastric ulcers was confirmed by the histological assessment of biopsy specimens (8–10) taken at the ulcer margin. The patients with duodenitis had endoscopic findings of diffuse erythema, oedematous folds, friability, and erosions of the duodenum, but they did not have ulcers. Antral gastritis was histologically diagnosed18 and was present in almost all patients with H pylori associated benign gastroduodenal diseases. The 25 patients classified as having antral gastritis had no visible pathology; they had microscopic antral gastritis only.
The patients with benign gastroduodenal diseases underwent upper gastrointestinal endoscopy during which a gastric juice sample and six antral and four body biopsy specimens were taken. Gastric juice was stored at −20°C until DNA extraction, while the mucosal biopsy specimens were fixed in formalin and embedded in paraffin wax. Two antral and two body specimens were stained with haematoxylin and eosin for the microscopic evaluation of gastritis; the remaining four antral and two body specimens were stained with Giemsa and/or Whartin Starry for the histological assessment of H pyloriinfection.
DNA was extracted from frozen gastric juice obtained from patients with benign gastroduodenal diseases and from frozen tissue samples of patients with gastric adenocarcinoma, following the standard phenol chloroform technique as previously described.29Using the polymerase chain reaction, the followingH pylori genes were studied: urease A (ureA) with the primers URE1 (5′GACATCACTATCAACGAAGG3′) and URE2 (5′TGAAAACCACGCTCTTTAG3′)29; cagAwith the primers HPC1 (5′TCAAATACACCAACGCCTCC3′) and HPC2 (5′AGCTTCTTGTGGGGACAATC3′), constructed using a specific PC program (Primer, version 0.5, Whithead Institute for Biomedical Research, Cambridge, USA); and the polymorphism of vacAwith the primers VA1-F, VA1-R, VA3-F, VA3-R, VA4-F, and VA4-R under the conditions described by Atherton et al.26
From each fasting patient a serum sample was obtained for the determination of total anti-H pyloriantibodies (ELISA procedure) and western blotting. Both tests were performed using commercial kits supplied by Alifax (Padova, Italy) and Arnika (Milano, Italy) respectively. The antigen used for the ELISA determination of anti-H pylori antibodies was obtained from lysed bacteria and comprised more than 20 epitopes. The latter was achieved using the H pyloristrain ATCC 43504 antigens first electrophoresed on sodium dodecyl sulphate polyacrylamide and then transferred onto nitrocellulose strips. Diluted sera were incubated with the strips; after washing, an anti-IgG alkaline phosphatase conjugated antibody and the corresponding substrate were added. The coloured end products, evidenced as stained bands, corresponded to the antigen-antibody complexes.
Data were analysed by the χ2 test, analysis of variance (one way ANOVA), and Bonferroni’s test for pairwise comparisons.
Results
We studied patients with gastric adenocarcinoma and compared them with four groups of patients with benign gastroduodenal diseases (gastric ulcer, duodenal ulcer, antral gastritis, and duodenitis). The mean age of patients with gastric adenocarcinoma (66 (SEM 3) years) was significantly higher than that of patients with duodenal ulcer (51 (2) years), antral gastritis (52 (3) years), or duodenitis (47 (5) years), but not that of patients with benign gastric ulcer (60 (3) years) (one way ANOVA: F=5.6, p<0.001).
In agreement with the histological assessment, theureA gene was found in all patients with benign gastroduodenal diseases, thus confirming the presence ofH pylori infection. In patients with gastric adenocarcinoma the histological assessment of H pylori was not available and, to diagnose the infection, we evaluated the results of the polymerase chain reaction, which was performed in two tissue samples: one from the tumour mass and another from the adjacent non-neoplastic mucosa. In these patients the results of the polymerase chain reaction obtained in the neoplastic samples were identical to those obtained in the adjacent non-neoplastic mucosa:ureA was found in 17/21 (81%) cases.
Table 1 shows the cagA gene andvacA polymorphism in patients with benign diseases and those with gastric adenocarcinoma who were positive forureA. cagA and the alleles s1 and m1 of vacA were significantly less frequent, while the alleles s2 and m2 ofvacA were significantly more frequent in patients with antral gastritis than in any of the other patient groups.
cagA gene and vacA polymorphism in patients with benign gastroduodenal diseases or gastric adenocarcinoma. All patients had positive results for ureA gene
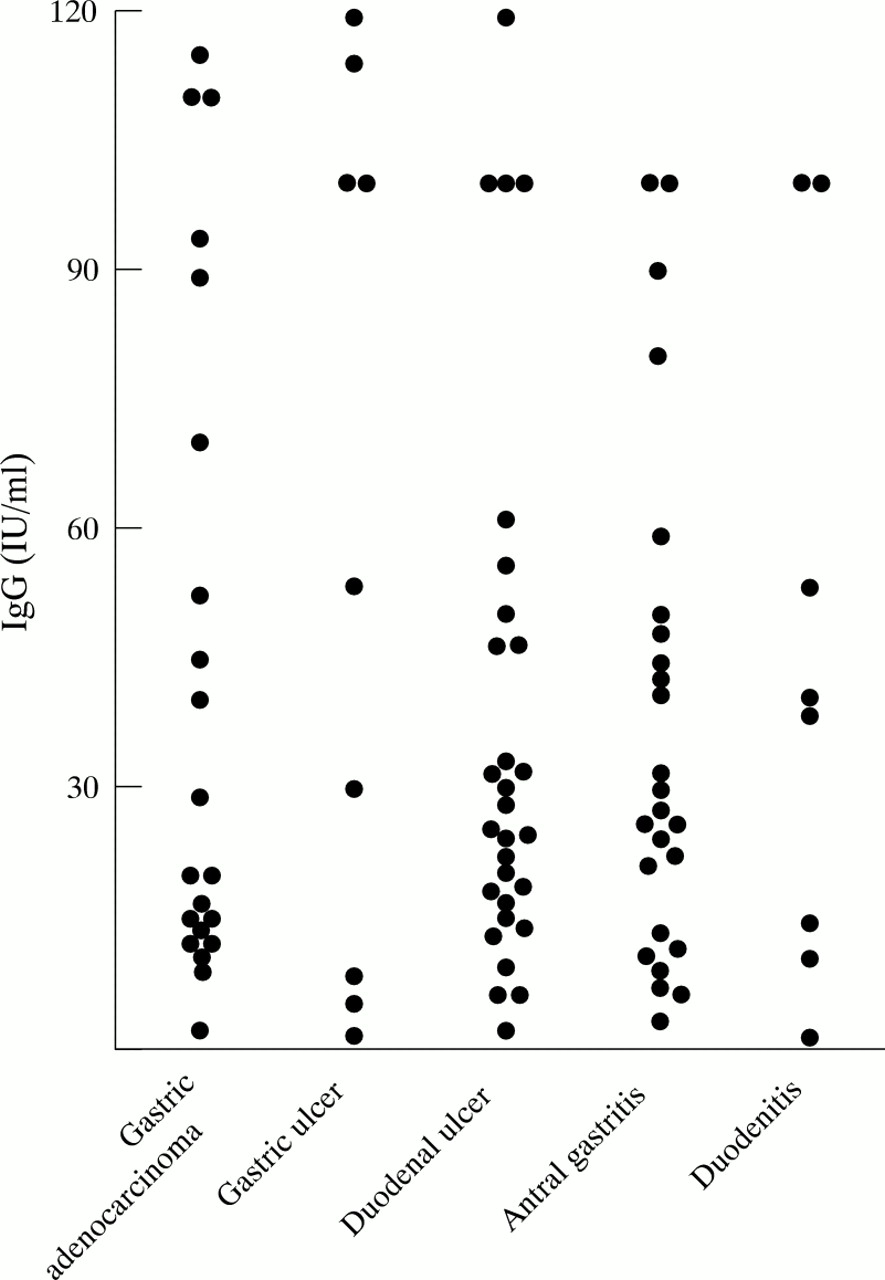
Figure 1 shows the serum anti-H pyloriantibodies levels found in our material. No significant difference was found between the five studied groups (one way ANOVA:F=0.98, NS). Four patients belonging to the gastric adenocarcinoma group were H pylorinegative and had values for anti-H pyloriantibodies of 2, 9, 12, and 52 IU/ml. Considering that the cut off limit for this method, calculated on a large series ofH pylori negative subjects, is 10 IU/ml, the sensitivity in the present series was 84%.
{kind=link}
Individual values of anti-H pylori antibodies.
Overall analysis of western blots showed that at least 22 bands were present with molecular weights ranging from 24 kDa to 136 kDa. Only four antigens were known (CagA, VacA, UreB, and UreA of 136 kDa, 86 kDa, 66 kDa, and 26 kDa respectively); the nature of the others was not identified.
Table 2 shows the percentage of positive cases for each band after subdividing the patients on the basis of diagnosis.
Percentage of positive cases for each band detected by western blotting. Patients were considered overall and on the basis of the diagnosis
Discussion
Our main aim was to ascertain whether there was an association between H pylori specific genotype pattern and malignancy. Seventy one H pyloripositive patients with benign gastroduodenal diseases were compared with 21 patients with gastric adenocarcinoma. Seventeen (81%) of the latter were found to have H pyloriinfection, confirming previous data on the high frequency ofH pylori infection in patients with gastric adenocarcinoma, especially when the bacterium is investigated in surgical samples, as in our study.4 ,10 ,30 ,31 Of the four H pylori negative patients with gastric adenocarcinoma, two had a tumour of the upper third of the stomach, which may have a non-H pylori associated aetiology. Both the neoplastic and the non-neoplastic mucosal samples from H pylori infected adenocarcinoma patients were positive for H pylori(polymerase chain reaction). The high frequency of positive results in neoplastic samples, partly in disagreement with previous data,30 ,31 may have depended on the different methods used to identify this bacterium: we used the polymerase chain reaction which has a high sensitivity and may therefore significantly enhance the detection rate of histology.29 However, the ability to detect H pylori by polymerase chain reaction from gastric adenocarcinoma specimens may be because these are contaminated with gastric juice, and does not necessarily imply direct colonisation of gastric adenocarcinoma by H pylori.
One of the major virulence factors of H pylori is an 86 kDa protein, a vacuolating cytotoxin, which can induce cell vacuolisation.25 This protein is coded by the polymorphic vacA gene: the s1 sequence of the region encoding the signal peptide and the m1 of the mid portion of the gene are associated with a high cytotoxicity. Sequences s2 and m2 are found in non-cytotoxic strains, while the s1 and m2 combination is associated with moderate cytotoxicity.25 ,26
Furthermore, unlike non-cytotoxic strains, the vast majority of cytotoxic H pylori strains have thecagA gene.25 ,26 A large number of studies have shown the association between CagA positive serology and peptic ulcer disease25 ,28 ,32 and gastric cancer.12 ,14 In agreement, cagAgene, assessed by polymerase chain reaction, was found to be associated with ulcer status.32-34 Further studies have assessed the association between vacA genotype and benign gastroduodenal pathologies, showing the association between the alleles s1 and m1 and peptic ulceration.32 ,35 In this study we found a significant association between cagA and the alleles s1 and m1 of vacA and diseases of either a neoplastic or non-neoplastic nature, in particular gastric and duodenal ulcer and gastric adenocarcinoma. This finding, in agreement with previous data,25 ,26 ,32-34 indicates that H pylori cytotoxin plays a role in promoting the development of severe mucosal damage, although it does not seem to be singly involved in the pathophysiological cascade leading to gastric adenocarcinoma. Furthermore, the higher mean age of patients with gastric adenocarcinoma suggests that long persistence of H pylori infection together with long exposure periods to different carcinogens are probably involved in the pathogenesis of gastric cancer.
The carcinogenic effect of H pylori probably depends not only on its ability to produce the vacuolating cytotoxin, but also on other virulence factors. We therefore evaluated the serological pattern of antibodies elicited againstH pylori antigens by means of western blotting. Twenty two bands of different molecular weights were clearly identified. Of these only four have been defined in nature: CagA of 136 kDa, VacA of 86 kDa, Urease B of 66 kDa, and Urease A of 26 kDa. The serological pattern of anti-CagA antibodies in patients with benign or malignant diseases confirmed the above mentioned findings on theH pylori genotype; in particular, positive findings were highly frequent in patients with gastric or duodenal ulcer and in those with gastric adenocarcinoma. Anti-VacA were found less frequently than anti-CagA; this discrepancy is probably due to the different immunogenetic properties of vacuolating cytotoxin with respect to the CagA protein.25
In patients with gastric adenocarcinoma the antibodies against the 74 kDa band were less frequent than in patients with benign diseases. However, a modified antibody response to H pylori in patients with gastric adenocarcinoma has recently been described: an increased frequency in the antibody response to a 45 kDaH pylori antigen was reported by Mitchellet al,13 and a reduced antibody response to 33 and 66 KDa H pylori antigens was reported by Klaamas et al.36
The final observation regarding western blotting results concerns the absolute sensitivity of the antibody, anti-55 kDa H pylori antigen, which was found in all H pylori positive cases. This sensitivity largely overcomes that of the routine determination of anti-H pylori antibodies (84% in the present series). Preliminary results indicate that in H pylori negative subjects the anti-55kDa antibody is rarely found (3/18), suggesting that it also has a good specificity (83%). If this is confirmed in large series, this antibody might have significant diagnostic advantages in the assessment of H pyloriinfection.
Acknowledgments
Filippo Navaglia is supported by a fellowship from the Associazione Italiana per la Ricerca sul Cancro.