Article Text

Abstract
Background and aims: Gastric mucosa associated lymphoid tissue lymphoma is a well defined B cell lymphoma yet often impossible to distinguish from severe chronic gastritis on morphological grounds alone. Therefore, it was suggested to use the clonality of the immunoglobulin (Ig) heavy chain (H) genes, as detected by polymerase chain reaction (PCR), as a decisive criterion. However, there is controversy as to whether B cell clonality also exists in chronic gastritis, hence rendering this approach futile at present.
Methods: An expert panel re-examined the histology and immunohistochemistry of a total of 97 cases of gastric biopsies, including clearcut marginal zone lymphoma, chronic gastritis, and ambiguous cases, applying the Wotherspoon criteria on the basis of haematoxylin-eosin and CD20 immunostainings. In addition, a new and advanced PCR system for detection of clonal IgH gene rearrangements was independently applied in two institutions in each case.
Results: The overall IgH clonality assessments of both institutions were in total agreement. Overt lymphoma (Wotherspoon score 5) was clonal in 24/26 cases. Chronic gastritis (Wotherspoon scores 1 and 2) was not clonal in 52/53 cases; the clonal case being Wotherspoon score 2. Of 18 cases with ambiguous histology (Wotherspoon scores 3 and 4) four were clonal.
Conclusions: Using advanced PCR technology, clonal gastritis is extremely rare, if it exists at all. Thus B cell clonality in Wotherspoon 3 and 4 cases is regarded as suitable for definitively diagnosing gastric marginal zone lymphoma.
- Ig, immunoglobulin
- PCR, polymerase chain reaction
- MALT, mucosa associated lymphoid tissue
- LEL, lymphoepithelial lesions
- gene rearrangement
- gastritis
- lymphoma
Statistics from Altmetric.com
- Ig, immunoglobulin
- PCR, polymerase chain reaction
- MALT, mucosa associated lymphoid tissue
- LEL, lymphoepithelial lesions
Primary gastric lymphoma (ICD-O 9699/3) arising in the marginal zone of the mucosa associated lymphoid tissue (MALT) is an indolent lymphoma which is acquired in the course of chronic gastritis of different aetiologies, including Helicobacter pylori infection and local autoimmunity.1 Histomorphological characteristics of gastric MALT lymphoma are infiltration of marginal zones of reactive follicles by centrocyte-like cells extending into interfollicular regions and replacing the plasma cell compartment. A histological hallmark for gastric MALT lymphoma is the presence of lymphoepithelial lesions (LEL), defined as groups of three or more neoplastic B cells in gastric gland epithelium.2 In newly formed dome-like regions of acquired gastric MALT, sporadic non-neoplastic LEL are thought to arise in severe chronic gastritis while LEL distant from lymph follicles are regarded as hallmarks of emerging gastric marginal zone lymphoma. Cytogenetically defined subtypes of gastric marginal zone lymphoma tend to further progress to more aggressive diffuse large B cell lymphoma.3,4 Recognition of this transformation is not a problem for the pathologist if the biopsy contains both neoplastic subpopulations. Serious problems however pertain to the other end of the spectrum which is the distinction between full blown chronic gastritis and covert gastric MALT lymphoma. This difficulty is reflected by the histomorphological scoring system proposed by Wotherspoon and colleagues2 which is broadly applied (table 1). It correlates histological features with the degree of probability of being reactive compared with neoplastic. The score leaves us with two ambiguous categories, scores 3 and 4, score 3 favouring a reactive and score 4 favouring a neoplastic infiltrate. In Wotherspoon 3 and 4 situations, additional tests need to be done to prove or discard malignancy.
Histological scoring of lymphoid infiltrations in the stomach according to Wotherspoon and colleagues2
A widely used method to help distinguish between reactive and malignant lymphoid lesions is the analysis of rearranged antigen-receptor genes.5 The rationale of this method is based on the observation that reactive lesions, with rare exceptions, are poly- or oligoclonal, meaning that they consist of numerous or at least several different lymphoid cell clones. This diversity of the cell clones can be identified by demonstrating differently rearranged antigen-receptor genes. In contrast, malignant lymphoid cell proliferations are clonal. This clonality is detectable by showing that a significant proportion of the lymphoid cells in a lesion contain identically rearranged antigen-receptor genes which are in B cells the immunoglobulin heavy chain (IgH) genes.
However, this elegant method, mainly performed by polymerase chain reaction (PCR) technology has—in common with every method—its limits and may lead to false negative or false positive results in some instances. There are two main reasons for false negative IgH PCR results preventing the detection of a clonal B cell population: (i) inability of the PCR primers to bind to their target sequences due to somatic mutations introduced in the germinal centre reaction, and (ii) very low number of clonal B cells in a sea of non-clonal reactive B cells. On the other hand, false positive results are most often found in extranodal sites where a limited number of reactive B cell clones are present in the absence of a polyclonal background as, outside the immune system, targets of local immunisation are also limited.
Initially it was thought that the IgH PCR is a valid tool for discrimination between gastritis and MALT lymphoma in gastric lesions of Wotherspoon 3 and 4. However, published data on B cell clonality of chronic gastritis are extremely divergent, ranging from 0%6 to 85%.7 The conclusion drawn from these findings—especially from studies with a high rate of clonality (table 2)—was that the frequent presence of “clonal” B cells, even in chronic gastritis, makes IgH PCR superfluous.
Review of the literature concerning IgH clonality in chronic gastritis
Since our own unpublished observations and several published data argue against the existence of a “clonal gastritis”, we initiated a multicentre study involving large numbers of clearcut gastritis specimens (Wotherspoon 1 and 2) and marginal zone lymphomas meeting the diagnostic criteria (Wotherspoon 5), together with ambiguous cases (Wotherspoon 3 and 4). For this purpose, a new IgH PCR system5 was applied in a blinded study, in two institutions, involving 97 cases which were reviewed by a panel of seven lymphoma experts from Germany and Switzerland. The results obtained demonstrated total agreement for the IgH PCR results between the two institutions and showed that overt gastric marginal zone lymphoma is clonal whereas chronic gastritis is not. Therefore, detection of clonal B cell populations in 22% of ambiguous gastric lesions (Wotherspoon 3 and 4) is regarded as a clear indication of the presence of covert MALT lymphoma.
MATERIAL AND METHODS
Cases
A total of 97 cases of chronic gastritis, ambiguous gastric lymphoproliferations, and primary gastric MALT lymphoma were collected from the files of the lymph node and haematopathology reference centres in Berlin, Frankfurt, Kiel, Lübeck, Ulm, Würzburg (Germany), and St Gallen (Switzerland).
Histology and immunohistochemistry
To economise and optimise the histological diagnostic procedure of gastric lymphoma, all archival material and stainings initially performed to determine the routine diagnosis were re-examined and the necessity and reliability of the antigens detected were re-assessed by the panel (SBC, ACF, M-LH, AM, PM, HS, and HHW, all being experienced haematopathologists). In the pilot phase, this panel agreed on haematoxylin-eosin staining and CD20 immunostaining (using L26 as the primary antibody, supplied by Dako, Glostrup, Denmark) as the minimal requirement for formal proof of the B cell nature of the infiltrates. This panel further agreed that LEL were best visible after CD20 immunohistochemistry. Sequential examination of haematoxylin-eosin and CD20 stained sections allowed easy consensus on the Wotherspoon score in each case at the multi-head microscope. During scoring, the panel pathologists were ignorant of IgH PCR data as that part of the study was carried out later in two institutions (Berlin and Frankfurt).
DNA extraction
DNA was independently extracted by the same method (Qiagen, Hilden, Germany) in two different laboratories (Berlin and Frankfurt) from serial sections of the same paraffin blocks. Extracted DNA was resuspended in 50 µl of distilled water and 300 ng of DNA were used for IgH PCR.
IgH PCR, pilot study
In a pilot study, 13 cases of MALT lymphomas (Wotherspoon 5), nine cases of chronic gastritis (Wotherspoon 1 and 2), and 14 ambiguous gastric lesions (Wotherspoon 3–4) were investigated by two types of IgH PCR. One protocol consisted of two rounds of IgH PCR (nested primer PCR) involving a set of FR1 VH family specific primers in the primary amplification and a set of FR2 VH family specific primers in the secondary amplification in conjunction with established JH primers (LJH and VLJH, respectively).8 As an alternative, we used an IgH PCR system, which was recently developed by a European Concerted Action (BioMed-2) of more than 30 expert laboratories in the field of clonality studies.8 The development of this IgH PCR system also included extensive evaluation of the sensitivity and specificity of this method. It consisted of two separate IgH PCRs employing family specific VH primers for two framework regions (FR2 and FR3). Amplification was performed as a single step PCR in conjunction with the newly developed BioMed-2 JH primer (JH22).
Whereas only 6/13 cases of MALT lymphomas were clonal by conventional nested primer IgH PCR, the BioMed-2 IgH primer sets revealed clonal B cell populations in all but two MALT lymphomas. Three of 14 Wotherspoon 3 or 4 cases displayed IgH clonality by conventional PCR while 4/14 Wotherspoon 3 or 4 infiltrates were clonal by BioMed-2 IgH PCR. None of the cases of chronic gastritis revealed a reproducible clonal B cell population by either method.
The results obtained in this pilot study demonstrated that the BioMed-2 IgH PCR was more reliable in detecting B cell clonality than all previous clonality assays. Because of this superiority of the single step BioMed-2 IgH PCR, we decided to perform the multicentre study comprising 97 cases exclusively with this procedure.
IgH PCR, multicentre study
Amplification of rearranged IgH genes of all 97 cases by means of BioMed-2 IgH PCR was independently carried out at least twice per case in two different laboratories (Berlin and Frankfurt). The IgH PCR was performed in a single PCR round without reamplification employing all three framework primer sets (FR1, FR2 and FR3) in separate assays each in conjunction with the common JH primer (JH22). PCR conditions, which were identical in both laboratories, consisted of 50 cycles of denaturation (95°C, 15 seconds), primer annealing (60°C, 40 seconds), and elongation (72°C, 45 seconds), and the reaction mixture contained 1.5 mM MgCl2, 0.8 mM dNTPs, 70 pmol VH primers, 30 pmol JH22 primer, and 2 U of AmpliTaq Gold polymerase (Applied Biosystems, Weiterstadt, Germany).
GeneScan analysis
For precise determination of the length of the amplified PCR products, the fluorescence labelled amplificates were separated on a DNA sequencer (model 310A, Applied Biosystems) and analysed by GeneScan Software (Applied Biosystems). As the same equipment and internal size standard was used in both laboratories (Berlin and Frankfurt), the PCR results were directly comparable.
RESULTS
Haematoxylin-eosin and CD20 stainings are sufficient to reliably score B cell infiltrates according to Wotherspoon criteria
Morphological and immunohistochemical criteria found useful for distinction between chronic gastritis and gastric MALT lymphoma are summarised in table 3, including the hitherto not described phenomenon of overgrowth of superficial reactive plasma cells by ascending neoplastic marginal zone B cells (fig 1A, B). LEL were best recognised after CD20 immunostaining which, at the same time, highlighted lymph follicles allowing decisive assessment of whether or not an LEL was follicle associated. Consensus of the pathologist panel was achieved in each case by close examination of the haematoxylin-eosin and CD20 immunostained sections.
Histological and immunohistochemical criteria useful in the distinction between gastric mucosa associated lymphoid tissue lymphoma and gastritis

Infiltration patterns of gastric mucosa associated lymphoid tissue (MALT) lymphoma (A, B), as evidenced by immunohistochemistry (scale bar 200 µm). As a hallmark of gastric MALT lymphoma, CD20 positive tumour cells were detected as lymphoepithelial lesions (arrow). In addition, MALT lymphoma cells colonised the tips of the lamina propria replacing the plasma cells incompletely (A) or completely (B).
Pseudoclonality is a problem
Dominant IgH PCR products in single PCR assays do not necessarily reflect the presence of a single clonal B cell population. In small specimens or in special sites with only a few B cells being present, IgH PCR may lead to detection of a non-representative singular dominant ( = pseudoclonal) PCR product (fig 2A). In order to avoid misinterpretation due to pseudoclonality, all IgH PCRs in this study were performed at least twice and the sizes of all amplificates were analysed by a high resolution GeneScan technique. Pseudoclonality was diagnosed in approximately half of the cases with Wotherspoon scores 3 and 4. Pseudoclonality was not demonstrated in MALT lymphoma (Wotherspoon 5) or chronic gastritis (Wotherspoon 1).

Demonstration of the different patterns of B cell clonality observed in chronic gastritis and gastric mucosa associated lymphoid tissue (MALT) lymphoma. All IgH polymerase chain reaction (PCR) products independently produced by both laboratories were analysed by the GeneScan technique (at least four analyses per case and per primer set). The red lines show the size standard; the blue lines represent the electropherograms of the size distribution of the PCR products. (A) Gastritis (Wotherspoon grade 4): individual dominant PCR products of different sizes (arrows) were generated among the different PCR assays of the same case (pseudoclonality). No reproducible dominant PCR product of the same size was detectable. (B) MALT lymphoma; a dominant PCR product of exactly the same size was reproducibly present in all PCR assays of the same case representing the clonal B cell population. (C) Gastritis (Wotherspoon grades 3 and 4); polyclonal and oligoclonal IgH rearrangement patterns were observed in most cases without an indication of a reproducible dominant PCR product. (D) Gastritis (Wotherspoon grade 4); a dominant PCR product of exactly the same size was reproducibly detectable in a moderate polyclonal background in all PCR assays of the same case, indicative of a small clonal B cell population. Note: All electropherograms were derived from IgH PCRs after amplification employing the primer combination BioMed-2 FR2.
BioMed-2 IgH PCR results are highly reproducible in independent institutions
The IgH PCR analyses were independently performed in a blinded fashion in two different laboratories, employing the BioMed-2 IgH PCR primer sets for all framework regions (FR1, FR2, and FR3) in conjunction with the BioMed-2 JH primer (JH22) in three separate PCR assays.5 Each case was analysed at least twice in both laboratories, employing all three FR primer sets, leading to at least 12 IgH PCR results in each case. In all cases the final conclusion regarding the presence or absence of a single B cell clone was identical in both institutions for all cases.
Overt MALT lymphomas are clonal
Twenty four of 26 cases (92%) of MALT lymphomas, morphologically diagnosed as Wotherspoon 5, displayed dominant amplificates of identical size as a clear indication of the presence of a clonal B cell population (fig 2B). In most cases (71%), clonal IgH rearrangements were detectable with all primer sets applied. In the remaining cases, IgH clonality was found in at least two of the three framework specific IgH PCRs with the exception of two cases, where IgH clonality was demonstrable with the FR1 primer set only.
Chronic gastritis is not clonal
Fifty three cases were scored as Wotherspoon 1 and 2 (that is, chronic gastritis). Approximately half of these cases revealed a clear polyclonal or oligoclonal IgH rearrangement pattern (fig 2C). In the remaining cases, dominant PCR products were identifiable in at least one of the three framework specific (FR1, FR2, or FR3) IgH PCR. Repetition of the IgH PCR with the same DNA demonstrated that the dominant PCR products were not or only partially reproducible. Therefore, these cases did not harbour a single B cell clone in the sense of a B cell lymphoma. In only one single case of Wotherspoon 2 gastritis was there a reproducible dominant IgH PCR product. Reassessment of histology confirmed Wotherspoon 2 score. Re-examining the file of this individual patient, two other gastric biopsies, one taken prior and one taken after the actual study sample, were found. Both additional samples also fulfilled Wotherspoon 2 criteria. However, in none of these specimens could a clonal B cell population be identified by IgH PCR. This finding leaves us with a singular yet longitudinally non-reproducible statement of B cell clonality in a morphologically reactive context.
IgH PCR reveals lymphomas among ambiguous lesions
Eighteen gastric B cell infiltrates were scored as Wotherspoon 3 or 4. In 14/18 cases (78%), PCR revealed an oligoclonal or polyclonal IgH rearrangement pattern. In eight of these cases dominant PCR products were found which were not reproducible in repetitive PCR assays. In four cases (22%) however, dominant amplificates of reproducible sizes were detectable in all PCR assays indicative of a true clonal B cell population (fig 2D).
DISCUSSION
Histological and/or immunohistological discrimination between gastric MALT lymphoma and reactive gastric lymphoproliferations is difficult or impossible in cases with lymphoid infiltration of scores 3 and 4, according to Wotherspoon.2 The seemingly first hand complementary approach to determine whether or not the B cell infiltrate is clonal is presently eroded by the large number of studies yielding alleged clonality in clearcut gastritis.7,9–13 Thus, to date, there has been no solution to this diagnostically and therapeutically relevant problem.
We have shown here that B cell clonality is indeed a discriminator in biopsies with ambiguous histomorphology, provided that the novel BioMed-2 IgH primer sets5 are applied and the pertinent problem of pseudoclonality is properly dealt with. In our hands, the conclusions drawn from repetitious PCR analysis on each biopsy proved highly reproducible, between institutions, and therefore can be recommended for general usage.
Both sensitivity and specificity were high for the final clonality statement as there were 24/26 cases of histologically clearcut lymphoma (Wotherspoon 5) as opposed to 1/53 cases of chronic gastritis. This single individual case of clonality assessment was found to be longitudinally non-reproducible and is, by definition, not a clinically relevant problem as the Wotherspoon score was 2 and hence histologically not suspicious.
Pseudoclonality was detectable in our study in nearly half of the cases of chronic gastritis and reactive gastric lymphoproliferations (Wotherspoon 3 and 4). The findings obtained in the two different PCR laboratories were completely in agreement and independently led to the same interpretation. We assume that this significant frequency of pseudoclonal cases might explain the high incidences of “clonal gastritis” in previous publications.
Against this background, we arrive at the core statement of this study. Given the fact that clonal gastritis, if it exists at all, is exceedingly rare, B cell clonality in biopsies scored Wotherspoon 3 and 4 has to be regarded as malignant. This was valid for 4/18 cases (thus a minority). These four cases should be regarded and treated clinically as gastric MALT lymphomas.
Diagnostic security has its price. It must be stated that our procedure more or less exhausts the primary diagnostic biopsy material. Additional tests such as interphase cytogenetics using methods such as fluorescence in situ hybridisation (for example, for detection of trisomy 3 or t(11;18)) might not be applicable due to insufficient amounts of neoplastic cells. Therefore, re-gastroscopy and re-biopsy prior to specific treatment is advisable.
It is well documented that gastric marginal zone lymphoma may be associated with a coexisting gastric diffuse large B cell lymphoma.14–16 Both clonal transition16 and collision lymphoma in the sense of clonally unrelated secondary lymphoma have been reported.17 Evidently, both types of B cell neoplasia fundamentally differ in response to current treatment protocols, including novel strategies for Helicobacter pylori eradication. Therefore, and according to the recommendation of the German Gastric Lymphoma Study Group, we propose extending the diagnostic procedure following a diagnosis of gastric MALT lymphoma by one further step; repeated gastroscopy and extended gastric biopsies, called gastric mapping. Gastric mapping requires eight biopsies from the gastric corpus and eight biopsies from the antrum, together with additional biopsies of macroscopically conspicuous areas (fig 3). Using this procedure, more lymphoma tissue is obtained, allowing reassessment of clonality by novel tissue, detection of potentially discriminative chromosomal aberrations by fluorescence in situ hybridisation probing, and exclusion or verification of coexisting large B cell component.

{kind=link}
{kind=link}
{kind=link}
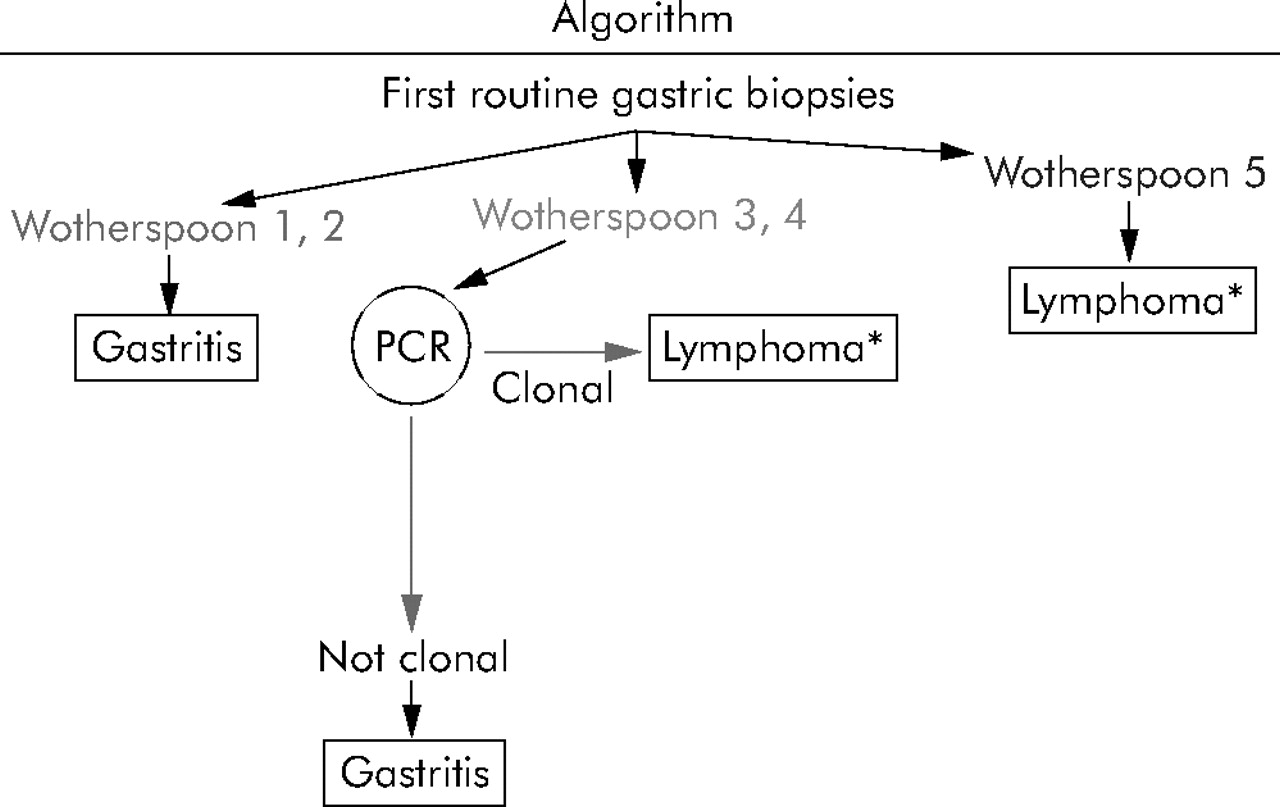
Algorithm suggested for the diagnostic procedure of gastric biopsies. PCR, polymerase chain reaction. *Lymphoma of MALT type; second biopsy recommended.
In conclusion, by combining strict application of Wotherspoon criteria with repetitious BioMed-2 IgH PCR, we have provided a tool suitable to robustly discriminate between full blown chronic gastritis and covert gastric MALT lymphoma in gastric biopsies.
Acknowledgments
We would like to thank Hans-Henning Müller and Susanne Hansen for excellent technical assistance.
REFERENCES
Footnotes
-
Published online first 19 January 2006
-
↵* M Hummel, S Oeschger, and T F E Barth contributed equally to this work.
-
Supported by grants from the Deutsche Krebshilfe (70-3173-Tr3 and 70-3139-Fe1), the Bundesministerium für Bildung und Forschung (01 GI 0396, “Kompetenznetz Maligne Lymphome”), the Mildred-Scheel-Stiftung (106367 to PM and TFEB), and the SAKK (Schweizerische Arbeitsgemeinschaft für Klinische Krebsforschung).
-
Conflict of interest: None declared.
Linked Articles
- Recent advances in clinical practice