Article Text

Abstract
Background Coronary microvascular dysfunction has been reported along with myocardial viral infection. Whether intramural coronary vessels infection plays a role in patients with cardiac syndrome X (CSX) is unknown.
Methods Thirteen consecutive patients (four men, nine women, mean age 51±10.5 years) with drug-resistant CSX underwent left ventricular endomyocardial biopsy. Myocardial tissue was examined for histology, immunohistochemistry and for the presence of cardiotropic viruses by PCR analysis. In the presence of a viral infection on the whole tissue, laser microdissection was performed to analyse the viral genome selectively in intramural vessels and cardiomyocytes. Controls were surgical cardiac biopsies from patients with chronic stable angina and from patients with mitral stenosis and normal cardiac function (normal controls).
Results Histology showed hypertrophy and degeneration of cardiomyocytes with interstitial and replacement fibrosis in all CSX, while focal lymphocytic myocarditis was additionally recognised in three patients. No vasculitis was observed. Viral genomes were detected in nine of 13 CSX (Epstein–Barr virus in four, adenovirus in three, human herpes virus (HHV) 6 in one, Epstein–Barr adenovirus co-infection in one). Laser microdissection showed that Epstein–Barr and adenovirus localised both in cardiomyocytes and intramural vessels, while HHV-6 infection was confined to the vessel wall.
Conclusions Viral genomes can be detected in intramural vessels of up to 69% of drug-resistant CSX. Coronary small vessels infection represents an alternative pathophysiological mechanism of this syndrome and can explain the poor response to anti-ischaemic drugs.
- Coronary microcirculation
- endomyocardial biopsy
- laser microdissection
- microvascular
- myocarditis
- syndrome X
- virus
Statistics from Altmetric.com
- Coronary microcirculation
- endomyocardial biopsy
- laser microdissection
- microvascular
- myocarditis
- syndrome X
- virus
The observation of typical effort angina and electrocardiographic and/or metabolic evidence of myocardial ischaemia in patients with angiographically normal epicardial coronary arteries and no other recognised causes of chest pain has been defined in 1973 as cardiac syndrome X (CSX), to underline the puzzling characteristics of this entity.1
Multiple studies have subsequently demonstrated the presence of coronary microvascular dysfunction, suggested by reversible perfusion defects at stress myocardial scintigraphy2 and at cardiovascular magnetic resonance,3 impaired response of coronary blood flow and/or resistance to endothelium-independent stimuli, impairment of endothelium-dependent coronary microvascular dilation4 and increased vasoconstrictor reactivity of small coronary artery vessels.5 Mechanisms that might influence coronary microvascular dysfunction, including altered autonomic tone,6 insulin resistance,7 enhanced ion transport across cell membrane,8 increased endothelin 1 release9 and oestrogen deficiency,10 have also been involved.
However, the cause of microvascular dysfunction is largely unknown, because few studies have directly investigated the structure and function of small coronary vessels.
Myocardial viral infection has recently been associated with coronary microvascular dysfunction, while increased plasma levels of inflammatory markers11 and evidence of systemic chronic infections12 have been detected in CSX.
The aim of the present study was to investigate the potential role of intramural coronary vessel infection in patients with CSX.
Materials and methods
Patient population
We studied 13 consecutive patients (four men, nine women, 51±10.5 years) with drug-resistant CSX. CSX was defined on the basis of the following parameters: (1) a history of effort chest pain for more than 6 months; (2) smooth coronary arteries in multiple angiographic views; (3) electrocardiographic ST segment deflection on exercise stress testing.
Inclusion criteria were: (1) recurrent episodes of angina pectoris despite maximal tolerated drug treatment, including a combination of at least two anti-ischaemic (beta-blockers, calcium antagonists and nitrates) or one anti-ischaemic and one alternative drug (xanthine derivatives, ACE inhibitors, statins and imipramine); (2) age between 18 and 75 years, inclusive; (3) written informed consent.
The relevance of chest pain was evaluated with a standardised questionnaire modified from Master13 and in all cases patients with CSX were confirmed to have chronic episodes of chest pain, referred to as ‘pressure or constriction’, mainly precipitated by physical effort or emotional stress and occurring several times a week. This severe clinical presentation that significantly limited daily activities and impaired quality of life leading to frequent hospital readmissions prompted the execution of the endomyocardial biopsy study.
Patients with CSX were excluded in cases of moderate to severe hypertension, diabetes, significant valvular heart disease, autoimmune disease, recent pregnancy, alcohol abuse, left ventricular hypertrophy on echocardiogram, abnormal resting electrocardiogram (ECG), vasospastic angina (ruled out on the basis of the clinical history and the intracoronary ergonovine test results) and inability to understand the patient information or give informed consent.
As control groups for clinical, histological and molecular biology studies we recruited 15 patients with chronic stable angina and 20 patients with mitral stenosis and normal cardiac function (normal controls), comparable to patients with regard to age and gender.
The study was approved by the local ethics committee, and written informed consent was obtained from each patient after the study protocol was explained.
Cardiac studies
All patients underwent non-invasive cardiac studies, consisting of basal ECG, Holter monitoring, ECG stress test and two-dimensional echocardiography. Invasive cardiac studies, after informed consent, included coronary and left ventricular angiography and left ventricular endomyocardial biopsy. In particular, a coronary angiography was performed at the time of study enrolment in all patients. All patients were also submitted to atrial pacing according to previously published protocols.9 14
Endomyocardial samples (six to eight for each patient) were performed and collected as described previously.15 16 At the time of cardiac catheterisation, blood samples were collected and stored at −80°C. All patients underwent routine laboratory tests, including C-reactive protein and erythrosedimentation rate, serological tests for the most common cardiotropic viruses and immunological studies.15
Immunohistological studies
Histological and immunohistochemical studies were performed according to previously published protocols.15 16 Dallas criteria were adopted for histological diagnosis of myocarditis and implemented by the characterisation of inflammatory infiltrates.15 16
Cellular localisation of viral antigens was performed by means of the following antibodies: Epstein–Barr virus (EBV) nuclear antigen 1 (1:10; Chemicon, California, USA),16 Mouse anti-adenovirus monoclonal antibody (clone A62020069A; Biogenex, California, USA), mouse monoclonal antibody to gp116/64/54 of human herpes virus (HHV) 6A and B (Advanced Biotechnologies, Maryland, USA).17
Molecular biology studies
Two to three frozen myocardial specimens from each patient were used for PCR and reverse transcriptase PCR analysis.15 16 The viruses screened included: enterovirus, adenovirus, EBV, parvovirus B19, HHV-6, herpes simplex 1 and 2 viruses, influenza virus A and B, hepatitis C virus, cytomegalovirus. The purified PCR products were sequenced directly on an automated ABI model 310 A sequencer (Applied Biosystems, California, USA). Blood samples of patients whose myocardium was infected by a viral agent were analysed by PCR for the presence of the same virus.
Laser microdissection
In the presence of a viral infection on the whole tissue, laser microdissection was performed to analyse the viral genome selectively in intramural vessels and cardiomyocytes. Briefly, formalin-fixed, paraffin-embedded endomyocardial biopsy samples were subjected to laser microdissection with the MMI UV-cut system (Molecular Machines & Industries, Florida, USA) integrated with a Nikon TE2000-S/E inverted microscope (Nikon, New York, USA).16 Cardiomyocytes and intramural vessels were dissected separately from haematoxylin and eosin tissue sections by means of an ultraviolet laser, performing circumferential dissection of selected tissue areas precisely following a drawn incision path under direct microscopic visualisation. The microdissected tissue areas were measured, documented and collected on an adhesive cap of nanotubes for nucleic acid extraction. A minimum of 100 cardiomyocytes and eight intramural vessels, randomly selected along the tissue sections, were collected for each patient (mean 129.5±22.9 and 12.8±.0, respectively). The specificity of selected cells was evaluated by direct microscopic visualisation. Negative controls included reagents without template and caps without microdissected cells.
Statistical analysis
Categorical data were presented as absolute frequencies and percentage values and quantitative measurements as mean±SD. The three groups were compared by Kruskal–Wallis analysis of variance for the quantitative variables and by χ2 test for the categorical variables. A p value of 0.05 or less was considered statistically significant.
Results
Data of the 13 patients with CSX are summarised in table 1. Comparison among CSX, chronic stable angina and normal controls is shown in table 2. In particular, all patients had smooth epicardial coronary arteries at coronary angiography.
Main clinical, histological and molecular characteristics of 13 patients with drug-resistant CSX
Comparison of baseline, histological and molecular characteristics among CSX patients, CSA patients and normal controls
Two patients had flu-like syndrome in the 6 months preceding the symptom onset. No patient referred to a history of infective mononucleosis, but all of them had a past EBV, cytomegalovirus and HHV-6 infection, as documented by the antibody profile. Serology for the other viruses screened was negative. In particular, no patient had a hepatitis C or HIV infection. White blood cell count, erythrosedimentation rate and C-reactive protein were within normal limits in all patients. Immunological tests were normal. Three patients (nos 3, 5 and 8) were postmenopausal women not on oestrogen therapy. Two patients with mild hypercholesterolaemia were treated with statins, with normalisation of cholesterol levels but without an improvement in anginal attacks.
Atrial pacing showed in all patients horizontal or downsloping ST segment depression greater than 0.1 mV, with (10 patients) or without (three patients) angina.
Immunohistological studies
In all CSX patients histology showed the presence of degenerative changes in the cardiomyocytes, consisting of Periodic acid-Schiff (PAS) and Sudan black negative cytoplasmic vacuoles due to areas of myofibrillolysis. In addition, an increased interstitial and perivascular fibrosis and focal areas of replacement fibrosis were present.
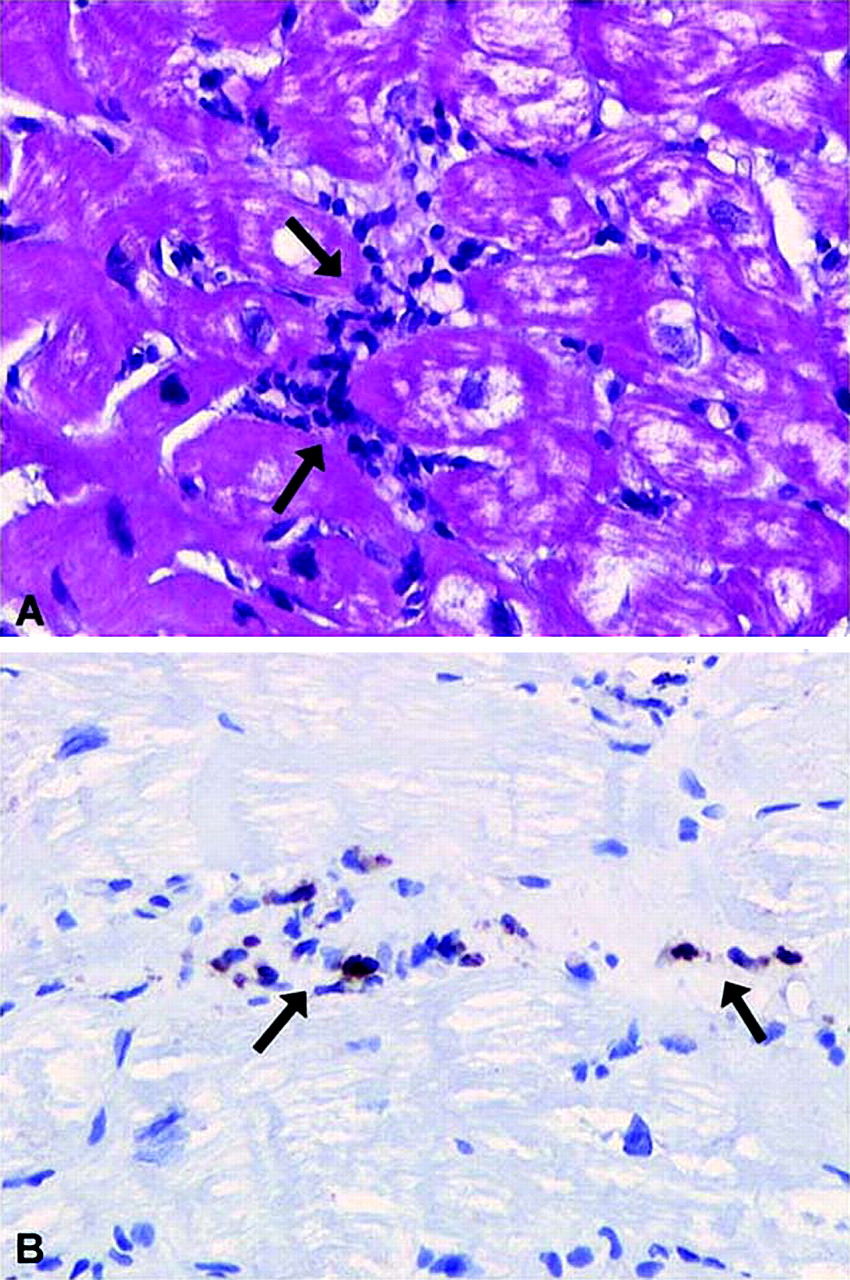
In three cases focal myocarditis was evident (figure 1A), mainly represented by T lymphocytes (CD3+, CD45RO+,CD8+) (figure 1B). No vasculitis was observed in any patient. All controls had normal or nearly normal histological findings. In particular, none had myocarditis, whereas focal cardiomyocyte degenerative changes were present in three out of 15 patients with chronic stable angina.

Left ventricular endomyocardial biopsy from patient 9 showing inflammatory infiltrates (arrows, panel A, haematoxylin-eosin, 200×), mainly represented by activated T lymphocytes (arrows, panel B, immunoperoxidase for CD45RO, 200×) with necrosis of the adjacent cardiomyocytes, indicating focal myocarditis. Cytoplasmic vacuolisation of cardiomyocytes indicates the coexistence of degenerative changes.
Molecular biology studies
In all cases, the presence of a sufficient target nucleic acid for PCR analysis was confirmed by amplification beta-globin for DNA and 3GPDH for RNA. In nine patients (69%), a viral infection was detected on the whole tissue (EBV in four, adenovirus in three, HHV-6 in one, EBV–adenovirus co-infection in one). PCR products sequencing confirmed the viral positivity and showed a minor variability among the isolates pertaining to different patients, which indicates that no false positives caused by cross-contamination were amplified.
Viruses were absent both in normal and in chronic stable angina control tissue. Blood samples from CSX patients were virus negative.
Laser microdissection
The presence of EBV, adenovirus and HHV-6 in cardiomyocytes and/or intramural vessels was determined in patients virus positive on the whole tissue (table 1).
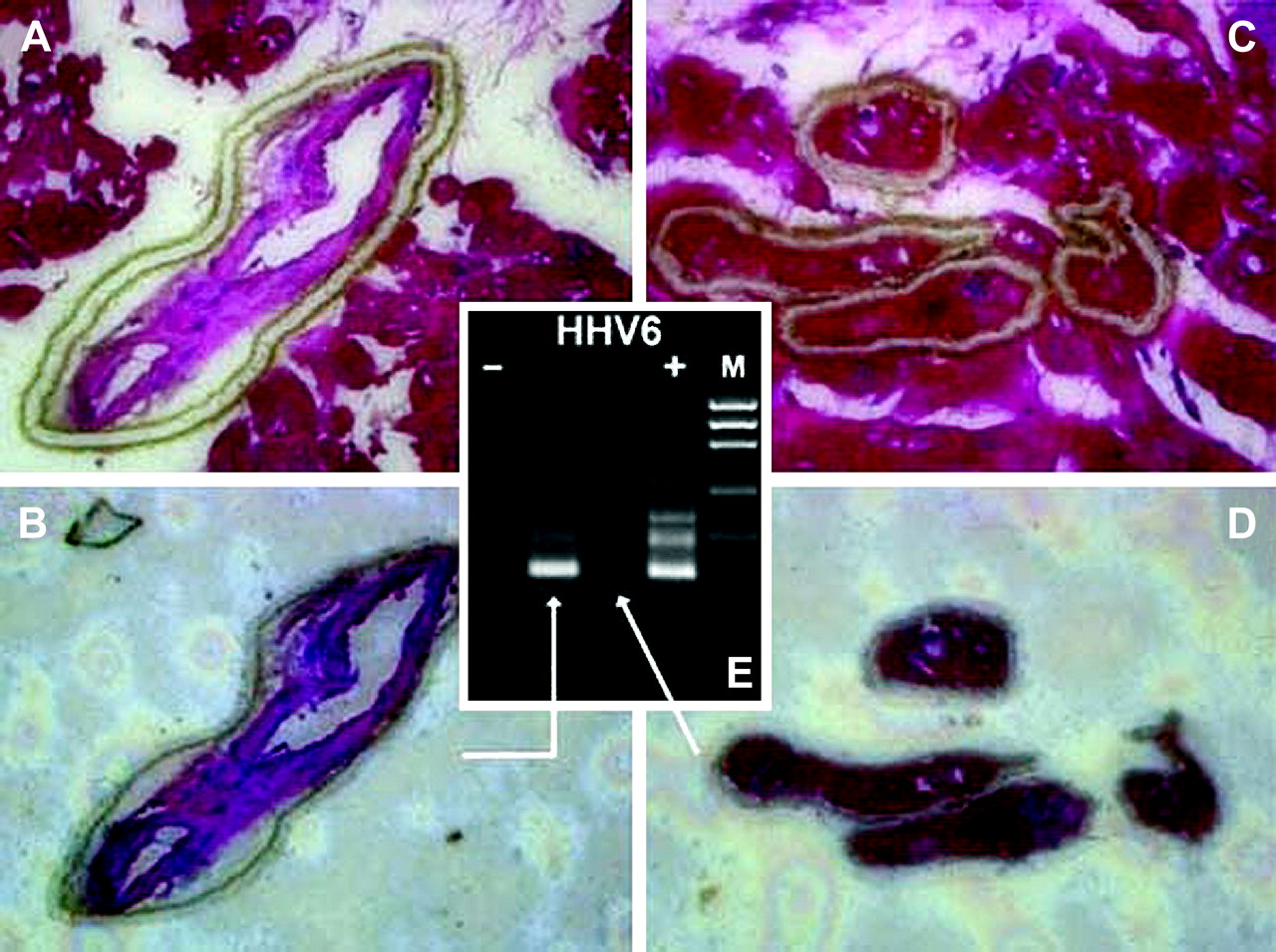
Adenovirus and EBV genome was detected in both microdissected cardiomyocytes and intramural vessels from patients nos 1, 9, 10, 13 and 6, 7, 8, 9, 11, respectively (table 1). Conversely, HHV-6 genome was confined to the vessel wall (patient no 12, figure 2). These results were confirmed on three repeated microdissection procedures. All the negative controls always showed no PCR product.

Laser microdissection in endomyocardial biopsy from patient 12 with human herpes virus (HHV) 6 myocardial infection. An intramural vessel (panel A) and four cardiomyocytes (panel C) were visually selected from haematoxylin-eosin stained sections (200× magnification) and the path of the selected tissue was traced before the laser activation. The excised vessel and cardiomyocytes are visualised on the adhesive cap in panels B and D, respectively. PCR analysis of separately microdissected vessels and cardiomyocytes using primers designed to amplify a 133 bp sequence of HHV-6 showed viral genome in intramural vessels but not in cardiomyocytes (panel E). Products were detected by ethidium bromide staining of 2% agarose gel. Lane 1, HHV-6-negative control (no template); lane 2, intramural vessels; lane 3, cardiomyocytes; lane 4, positive control (infected cells); lane 5, molecular weight marker.
Detection of virus protein in cardiomyocytes and intramural vessels
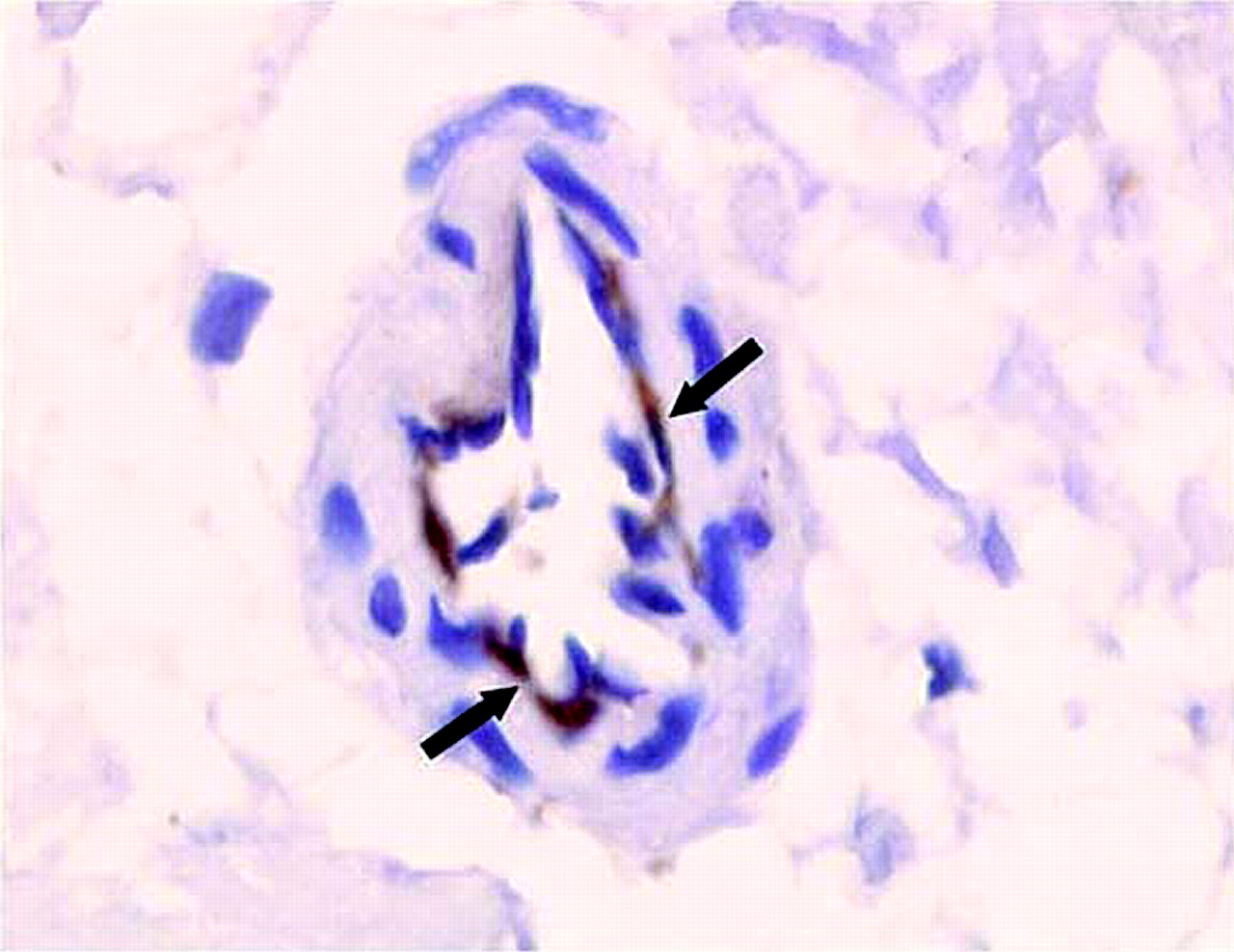
Immunostaining for EBV and for adenovirus antigens revealed a granular nuclear staining in rare cardiomyocytes and endothelial and/or smooth muscle cells of intramural vessels from all infected hearts. Immunostaining for HHV-6 in patient 12 showed a cytoplasmic positivity in endothelial cells of intramural vessels, but the immunostaining was not evident in cardiomocytes (figure 3).

{kind=link}
{kind=link}
{kind=link}
Immunohistochemistry for human herpes virus (HHV) 6. Intramural coronary arteriole from patient 12 showing immunostaining for HHV-6 antigen in endothelial cells (immunoperoxidase for gp116/64/54, 400×).
No labelling for viral antigens was seen in the cardiomyocytes or intramural vessels of controls.
Discussion
CSX is a heterogeneous syndrome mainly caused by dysfunction of small intramural coronary arteries that can be affected by either structural18 or functional abnormalities involving smooth muscle and/or endothelial cells.
The causes of microvascular dysfunction are largely unknown. Different mechanisms have been implicated, including traditional cardiovascular risk factors, such as hypertension and diabetes, insulin resistance,6 oestrogen deficiency in women10 and low grade inflammation, suggested by an increase in blood concentrations of C-reactive protein and IL-1 receptor antagonist.19 Moreover, the existence of myocardial ischaemia has been either questioned20–22 or demonstrated,14 suggesting this syndrome represents a conundrum with different possible pathogenetic mechanisms, most of them still not investigated.
From a therapeutic point of view different drugs have been tested, including statins, which improved endothelial function and quality of life23 through a reduction in oxidative stress and vascular inflammation.
Our study shows for the first time that myocardial viral infection can be detected in a high prevalence of patients with CSX refractory to maximal multidrug treatment. The infectious agents were localised in the small coronary vessels and were thus most likely implicated in the microcirculatory dysfunction of this syndrome.
Role of viral infection in CSX
Recent studies have demonstrated dysfunction of the systemic and coronary microcirculation in patients with myocardial virus persistence.24 Viral infection has been associated with endothelial dysfunction independently from myocardial leucocyte infiltrates and endothelial activation, suggesting a direct toxic effect of the infectious agents.24
In our study a selected group of patients who fulfilled strict diagnostic criteria for CSX showed in 69% of cases evidence of a myocardial viral infection.
Laser microdissection of the infected hearts revealed that viruses localised in the cardiomyocytes and in intramural vessels or, in the case of HHV-6, only in the vessel wall.
None of our patients had serological evidence of an active infection or the presence of a viral genome in the blood, thus ruling out a contamination from circulating cells.
Although the number of patients in the present study was limited mainly because of the restricted indication to perform an endomyocardial biopsy study in this group of patients (ie, drug-resistant angina), the prevalent detection of herpes viruses (ie, EBV and HHV-6, 67% of viruses detected) is relevant, as these viruses seem to have a preferential tropism for endothelial cells, and have been identified in the coronary microcirculation of patients presenting with unexplained chest pain.
In particular, a high prevalence of myocardial EBV infection has been described in patients with myocarditis mimicking an acute myocardial infarction.25 In patients presenting with chest pain and normal coronary anatomy, herpes viruses were detected even in the absence of histological signs of myocarditis. HHV-6 has been shown to infect adult heart microvascular endothelial cells and to upregulate the production of monocyte chemoattractant protein 1 and IL-8, leading to the attraction of immunocompetent cells and the development of inflammatory processes.26
Human herpes viruses are ubiquitous agents that usually infect a high percentage of the general population and can persist in several cell types. It can be hypothesised that in some patients, after a primary infection, the viral genome might persist in endothelial and/or smooth muscle cells, and in some cases (ie, EBV infection) also in cardiomyocytes, and under the influence of unknown factors it might reactivate and induce myocarditis. On the other hand, even in the absence of active replication and cytopathic effects, the virus can produce microvessel damage and dysfunction, through the synthesis of proteins that stimulate chemokine and proinflammatory cytokine production.27 It can be surprising that in the myocardium of our patient population we did not detect parvovirus B19, a well known endotheliotropic virus that has been associated with myocarditis presenting with chest pain. Possible explanations are the general low percentage of this virus detected by PCR in our studies14 compared with the high percentage reported from different countries,28 suggesting a different geographical distribution of this virus, as well as the restricted number of patients studied.
Adenovirus infection accounted for the remaining 33% of our virus positive results. Adenovirus represents the most common viral agent detected in adult patients with myocarditis28 and its receptor has been identified in several cell types, including cardiomyocytes, smooth muscle and endothelial cells.29 Adenovirus infection has been implicated in infarct-like clinical manifestations most likely related to microvascular dysfunction.
The absence of viral agents in the remaining 31% of our cases could be ascribed to different mechanisms of endothelial damage or alternatively viral agents not screened in our study.
Histological changes in CSX
Previous histological studies in CSX supported the presence of structural abnormalities of intramural coronary vessels, including medial hypertrophy and lumen narrowing, perivascular fibrosis, vessel inflammation and apoptosis of endothelial cells.18 30 In our group of patients none had normal histology and the prevalent morphological findings were represented by cardiomyocyte degeneration, increased fibrosis and by focal lymphocytic myocarditis.
The observed histological changes can be interpreted as the result of both myocardial inflammation/infection and microvascular ischaemia. In particular, cardiomyocyte degeneration, which was a constant marker in our patients, can be explained by either a cytopathic viral effect or can be the result of chronic myocardial ischaemia.
Limitations of the study
The main limitations of the study are represented by the small cohort of subjects with drug-resistant CSX enrolled and the poor investigation of coronary flow and/or endothelial dysfunction demonstrating the impairment of coronary microcirculation. Nevertheless, the latter is known to be compromised in both patients with CSX and with myocardial virus persistence.
Conclusions
Microvascular infection can be the cause of drug-resistant CSX. This observation expands the pathophysiological mechanisms of this syndrome and offers new chances to improve patients' management and quality of life.
References
Footnotes
Linked articles 206870.
Funding This study was funded by grant EX ART.56 entitled ‘HIV-related and unrelated inflammatory cardiomyopathy: identification of causal agents and pathogenetic mechanisms providing a tailored therapy’.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of La Sapienza University.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Correction