Article Text

Abstract
Background In patients presenting with acute cardiac symptoms, abnormal ECG and raised troponin, myocarditis may be suspected after normal angiography.
Aims To analyse cardiac magnetic resonance (CMR) findings in patients with a provisional diagnosis of acute coronary syndrome (ACS) in whom acute myocarditis was subsequently considered more likely.
Methods and results 79 patients referred for CMR following an admission with presumed ACS and raised serum troponin in whom no culprit lesion was detected were studied. 13% had unrecognised myocardial infarction and 6% takotsubo cardiomyopathy. The remainder (81%) were diagnosed with myocarditis. Mean age was 45±15 years and 70% were male. Left ventricular ejection fraction (EF) was 58±10%; myocardial oedema was detected in 58%. A myocarditic pattern of late gadolinium enhancement (LGE) was detected in 92%. Abnormalities were detected more frequently in scans performed within 2 weeks of symptom onset: oedema in 81% vs 11% (p<0.0005), and LGE in 100% vs 76% (p<0.005). In 20 patients with both an acute (<2 weeks) and convalescent scan (>3 weeks), oedema decreased from 84% to 39% (p<0.01) and LGE from 5.6 to 3.0 segments (p=0.005). Three patients presented with sustained ventricular tachycardia, another died suddenly 4 days after admission and one resuscitated 7 weeks following presentation. All 5 patients had preserved EF.
Conclusions Our study emphasises the importance of access to CMR for heart attack centres. If myocarditis is suspected, CMR scanning should be performed within 14 days. Myocarditis should not be regarded as benign, even when EF is preserved.
- Myocarditis
- cardiac magnetic resonance imaging
- acute coronary syndrome
- coronary angiography
- sudden cardiac death
Statistics from Altmetric.com
- Myocarditis
- cardiac magnetic resonance imaging
- acute coronary syndrome
- coronary angiography
- sudden cardiac death
Introduction
Contemporary strategies for managing patients presenting with acute cardiac symptoms, an abnormal ECG and raised serum troponin presume a diagnosis of myocardial infarction (MI). Care pathways implement rapid pharmacological and percutaneous reperfusion therapy for acute coronary syndrome (ACS). Urgent or emergency coronary angiography confirms the diagnosis and percutaneous treatment is the standard of care. However, in up to 10% of such patients at angiography, no culprit coronary lesion is identified.1–3
Subsequently, the differential diagnosis includes apparently non-significant coronary disease (including unstable plaque event, embolus, spasm and flush ostial occlusion of a branch artery), takotsubo cardiomyopathy and myocarditis.4 Several studies based on cardiac MRI5 6 and/or endomyocardial biopsy7 demonstrate that the majority of such patients have myocarditis. While the importance of secondary prevention of future coronary events following ACS has been well defined, the prognosis of myocarditis presenting with acute chest pain in the absence of left ventricular (LV) systolic impairment is not.8
Cardiac magnetic resonance (CMR) provides structural and functional information, but is unique in its ability to detect regional differences in myocardial tissue characteristics. In this regard, late imaging after gadolinium infusion may detect regions of relative enhancement. Following a myocardial infarction, a sub-endocardial or transmural pattern of late enhancement is typical; following myocarditis, late gadolinium enhancement (LGE) is typically epicardial, in the mid-wall or patchy but may also be transmural. Additionally, the detection of increased regional myocardial T2 signal indicates regional increases in water content inferring inflammation.9 Together, LGE and T2 imaging may reliably differentiate between MI and myocarditis.5–7 10 11
In a high-volume heart attack centre, patients admitted with an initial diagnosis of ACS that subsequently had normal coronary angiography are routinely referred for CMR imaging. We report our experience and discuss the importance of this role for routine CMR in centres managing acute coronary syndromes.
Methods
Patients
The London Chest Hospital heart attack centre provides assessment and treatment for patients diagnosed with ACS in north-east London, a population of 1.8 million. The centre manages approximately 650 patients with ST elevation MI (STEMI) and 1100 with non ST elevation MI (NSTEMI) diagnoses each year. Between April 2008 and January 2010, we analysed the scans in all patients referred for CMR following an acute admission with a provisional diagnosis of ACS based on symptoms, raised serum troponin and culprit lesion-free emergency coronary angiography. We also studied patients who did not undergo emergency angiography after similar admissions because the admitting cardiologist considered ACS had a low pretest probability. In a subset of patients, follow-up CMR scans were requested for clinical indications, including the detection of widespread abnormalities on the initial scan, persistent symptoms or an uncertain diagnosis following the first scan.
Imaging protocol
All CMR studies were performed on a 1.5 T Philips Achieva scanner with a cardiac 32-channel phased array coil. Balanced steady-state free precession cine images were acquired with 25–30 phases/cycle and 8 mm slice thickness, 2 mm gap. Four-chamber, two-chamber and LV inflow/outflow views and a short-axis stack from mitral annulus to apex were obtained (typical voxel size 1.9×1.9 mm). T2-weighted black-blood with fat saturation (TSE-STIR) was performed in three short-axis slices covering the basal, mid and apical myocardial segments and in both 4-chamber and 2-chamber long axis (standard imaging parameters include TR of 2 heart beats, TE 80 ms, in plane voxel size 1.6×2.2 mm, slice thickness 8 mm, typical FOV 350 mm). T1 weighted inversion-recovery gradient echo images were acquired 10 min after injection of a dose of 0.2 mmol/kg of gadoterate meglumine (Dotarem) for LGE. Inversion time was adjusted to null signal from healthy myocardium (voxel size 2.07×2.16 mm, slice thickness 8 mm, FOV 300 mm).
All scans were reviewed independently by two CMR accredited cardiologists. LV end diastolic (LVEDV) and end systolic (LVESV) volumes and ejection fraction (LVEF) were calculated according to previously described methods.12 Regional wall motion abnormalities were assessed semi-quantitatively and their distribution was reported according to the 17-segment classification of the American Heart Association. T2-weighted images were assessed qualitatively. Areas of high signal intensity were interpreted as myocardial oedema, and their distribution was reported according to the 17-segment model.
LGE was assessed qualitatively and its distribution reported according to the 17-segment model. A distribution of LGE confined to a sub-endocardial distribution was considered diagnostic for myocardial infarction (MI). Sub-epicardial, mid-wall or patchy LGE was considered diagnostic for myocarditis in the context of acute cardiac symptoms, raised serum troponin and normal coronary angiography. Myocarditis was diagnosed if transmural LGE was associated with histological evidence of myocarditis, if a follow-up CMR scan demonstrated change from a transmural into a sub-epicardial enhancement pattern, or if the segmental distribution of LGE was not compatible with a coronary territory.
Statistical analysis
Comparisons were made with paired and unpaired Student t tests for continuous variables and the Fisher exact test for categorical variables. Continuous variables were expressed as mean±SD if normally distributed. A p value <0.05 was considered significant.
Consent and ethics
At the time of their scans, all patients consented to their anonymised images and clinical data to be used for educational and teaching purposes.
Results
Patients
During the period of study, 1822 patients were admitted with a diagnosis of acute coronary syndrome (779 with STEMI, 1043 with NSTEMI). Of these, 79 (4.3%) patients fulfilling criteria were identified. Following the CMR scan, a diagnosis of MI or cardiomyopathy was made in 15 patients (19%) who were therefore excluded from further analysis. In 10 (13%) of these 15 patients, sub-endocardial or transmural LGE was observed in a coronary distribution. A further 5 (6%) patients had typical features of takotsubo cardiomyopathy. In the remaining 64 patients, a diagnosis of myocarditis was considered likely (figure 1).
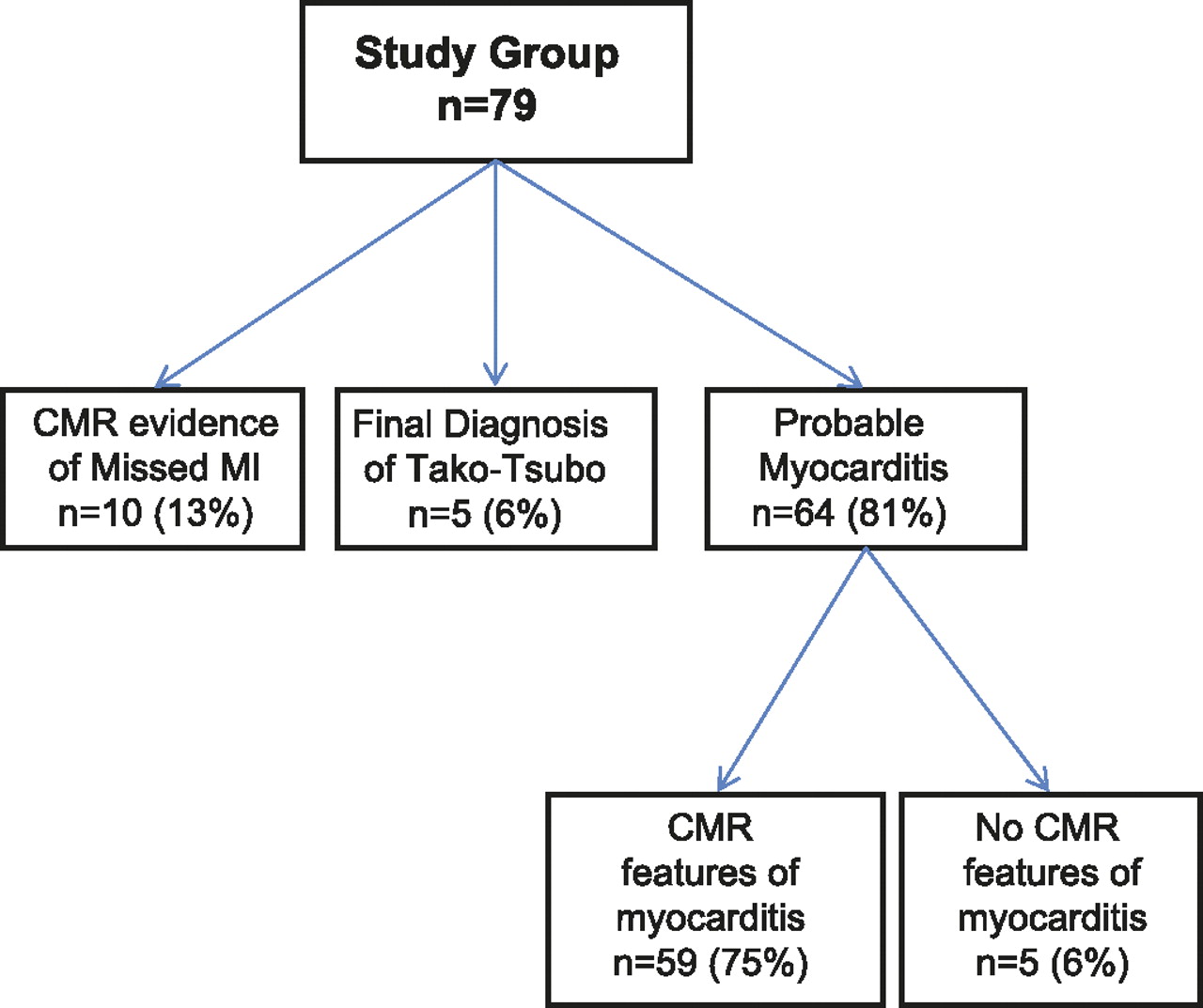
Flow chart demonstrating the final diagnoses in the study cohort admitted with acute cardiac symptoms, raised serum troponin and normal angiograms. CMR, cardiac magnetic resonance; MI, myocardial infarction.
Demographic and clinical findings
The mean age of 64 patients with probable myocarditis was 45±15 years (range 17–84); 70% were male. Serum troponin was raised in every patient. The presenting symptom was resting chest pain for the majority (91%). The clinical presentation was life-threatening in five patients (8%): three were admitted with sustained ventricular tachycardia (VT), another died 4 days after admission and a fifth re-presented with sustained VT 7 weeks later. All had preserved LV systolic function. Urgent coronary angiography was obtained in 55 patients (86%); 54 had unobstructed coronary arteries, and one patient with moderate coronary stenosis had CMR features of myocarditis and normal CMR stress perfusion imaging. In the nine (14%) individuals that did not undergo emergency angiography, the admitting cardiologist diagnosed pericarditis on the basis of clinical features including young age, symptoms and ECG changes. The mean age of patients not undergoing coronary angiography was 25±7 years (range 20–42; median 22) and was lower than in those investigated by angiography (49±14 years, range 17–84, median 47; p<0.0001). CMR was performed with a mean delay of 33 days (range 0–364; median 4) after onset of symptoms.
CMR findings
LV volumes and systolic function
End-diastolic volume was 150±42 ml and end-systolic volume was 65±29 ml. The mean ejection fraction (EF) was 58±10% (range 29–79); a normal EF (>54%) was measured in 71%. LV impairment was mild in 17% (EF 45–54%), moderate in 10% (EF 30–44%) and severe in 2% (EF <30%).12 Regional wall motion abnormalities were seen in 37% with a mean EF of 54±10%; in 12 (52%) of these, the EF was in the normal range. A pericardial effusion was detected in 10 (16%) patients.
T2 weighted imaging
T2 weighted imaging was obtained in 55 patients (86%) and hyperintense signals compatible with oedema were detected in 32 (58%). The average number of affected myocardial segments was 2.3±3.0 (range 0–13, median 1). Inferior, inferolateral and apical segments were preferentially affected; hyperintense T2 signals were less frequently detected in the septal segments. Figure 2A illustrates this pattern. All patients presenting with hyperintense T2 weighted signal had LGE in the same segments. Conversely, all patients with transmural LGE had evidence of co-localised hyperintense T2 signal.

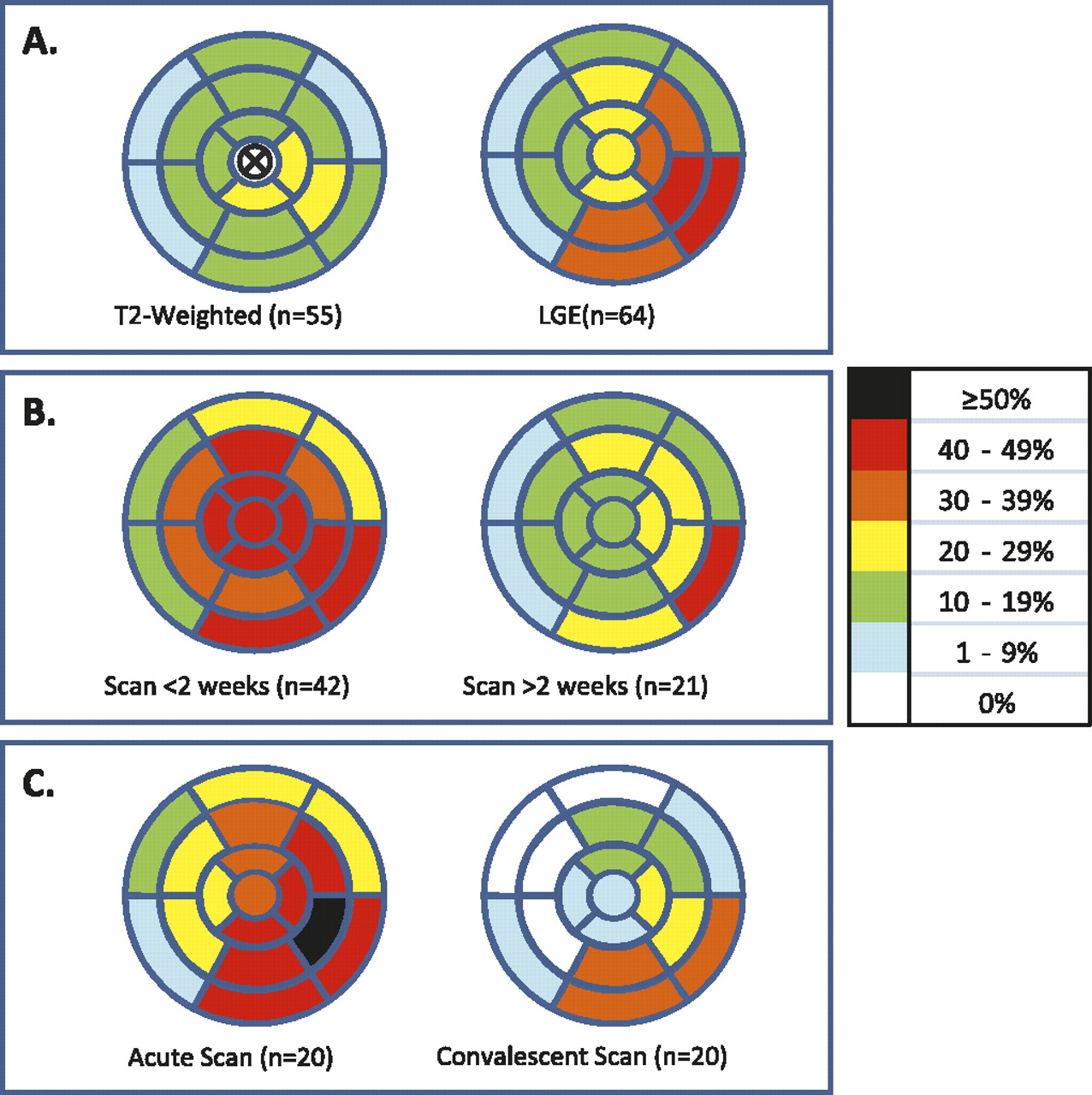
Bull's eye representation of myocardial involvement according to the AHA 17 segments model in acute myocarditis. (A) Relative frequency of segmental involvement of the myocardium with hyperintense T2-signal (left) and late gadolinium enhancement (LGE) (right) on initial scans. There is a preferential involvement of the inferior, inferolateral and apical segments. (B) Segmental distribution of LGE on initial scans performed <2 weeks (left) and >2 weeks (right) after symptom onset. LGE is less frequently detected in scans performed >2 weeks after symptom onset; there is still preferential involvement of the inferior and inferolateral segments and the septal segments are very infrequently involved. (C) Segmental distribution of LGE in initial scans (<2 weeks; left) and convalescent scans (>3 weeks; right). There is widespread myocardial involvement on the initial scans, with decrease in LGE for all myocardial segments except the basal inferolateral segment on convalescent scans.
Late gadolinium enhancement
LGE imaging was performed in all patients and was abnormal in 59 (92%). When present, LGE was sub-epicardial in 33 (56%), mid-wall in 9 (15%), patchy in 15 (25%) and transmural in 6 (10%). In one patient with transmural LGE, the distribution of enhancement did not follow any coronary territory, involving the anterior LV wall and the RV free wall, making it incompatible with a coronary injury. In a second patient with localised transmural LGE, a scan 57 days later demonstrated regression of transmural LGE to a typically epicardial myocarditic pattern. In the third patient with transmural LGE, LGE was also distributed in several myocardial segments, and giant cell myocarditis was demonstrated at post-mortem examination (figure 3).

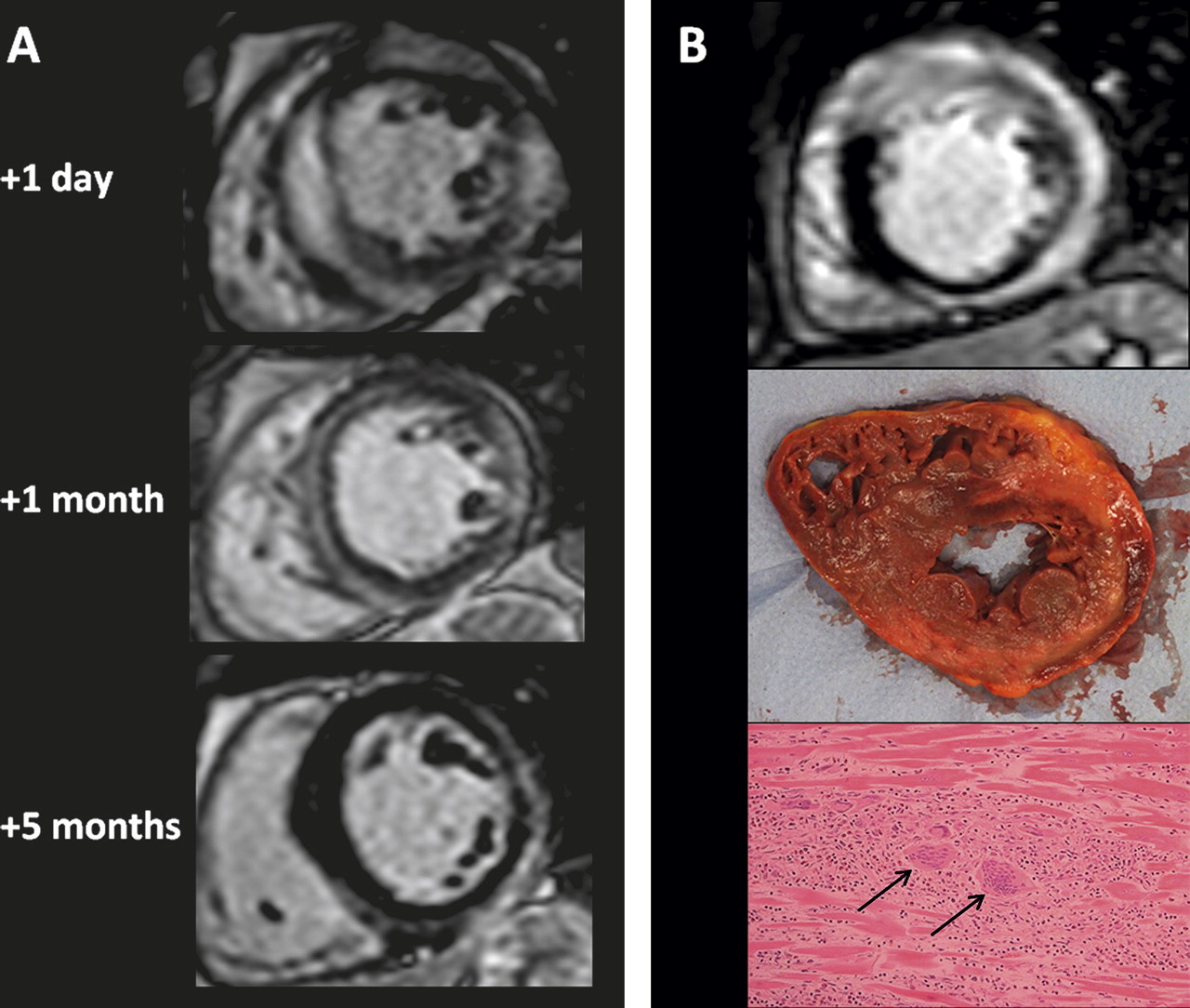
(A) Temporal evolution of the distribution and severity of late gadolinium enhancement (LGE) in acute myocarditis. The initial scan (1 day following admission) demonstrated widespread enhancement with almost transmural involvement of the septum and lateral wall associated with increased wall thickness. Basal inferolateral hypokinesia was noted, but left ventricular systolic function preserved (ejection fraction (EF) 59%). A repeat scan performed 1 month later showed no regional motion abnormalities and the myocardial wall thickness had normalised. The LGE enhancement remains evident in the same myocardial segments as before, but is clearly less severe. A third scan performed at 5 months shows almost complete resolution of septal LGE. The pattern of LGE adopts a classic myocarditic distribution, involving the epicardial layers of the inferior and lateral segments. (B) In another patient, the acute phase CMR (top picture) shows transmural LGE of the anterior wall with epicardial enhancement of the lateral and inferior walls. The basal anterior wall is thickened and hypokinetic but with preserved systolic function (EF 57%). This patient died suddenly 4 days after admission. The short-axis postmortem specimen corresponds approximately to the LGE image acquired 2 days earlier; transmural necrosis of the anterior wall with subepicardial necrosis of the lateral and inferior wall is evident macroscopically, matching well with the CMR images. Histology demonstrated myocyte necrosis, interstitial lymphocytic infiltration and giant cells (arrows); a diagnosis of giant cell myocarditis was made.
The number of affected myocardial segments was 4.3±3.9 (range 0–16; median 3) or 25% (range 0–94%; median 18%) of the 17 segments. LGE was mainly observed in the inferior and inferolateral walls as well as in the apical segments, and was less commonly seen in the interventricular septum (figure 2A).
In 3 of 5 patients without LGE, the interval between symptom onset and scan was prolonged (195–325 days). All three presented with chest pain; two described recent viral illness and had ST elevation on ECG consistent with pericarditis. A fourth underwent scanning 30 days after presenting with chest pain. The fifth was scanned 24 days after presenting with pulmonary oedema and a mild elevation in serum troponin; this patient had received Adriamycin for breast cancer several years previously, and had moderate global systolic impairment (EF 39%).
Effect of scan delay
We compared CMR findings between scans obtained within 2 weeks of presentation (n=42, median interval=3 days, range 0–10) with those obtained after this (n=21, median interval=39 days, range 19–364). The findings are summarised in table 1 and figures 2B and 4. There were no differences in EF or LV dimensions. High T2 signal was detected in 81% of early compared to 11% of late scans (p<0.0005), affecting 3.3±3.2 segments (range 0–13; median 3) compared to 0.3±1.0 (range 0–4; median 0; p<0.001). LGE was detected in 100% of early and 76% of late scans (p<0.005), affecting 5.3±4.2 segments (range 1–16; median 4) compared to 2.5±2.3 (range 0–8; median 2; p<0.01). A pericardial effusion was seen in 8 (19%) in the group scanned early and 2 (10%) in the group scanned later (NS).
Cardiac magnetic resonance findings according to scan delay
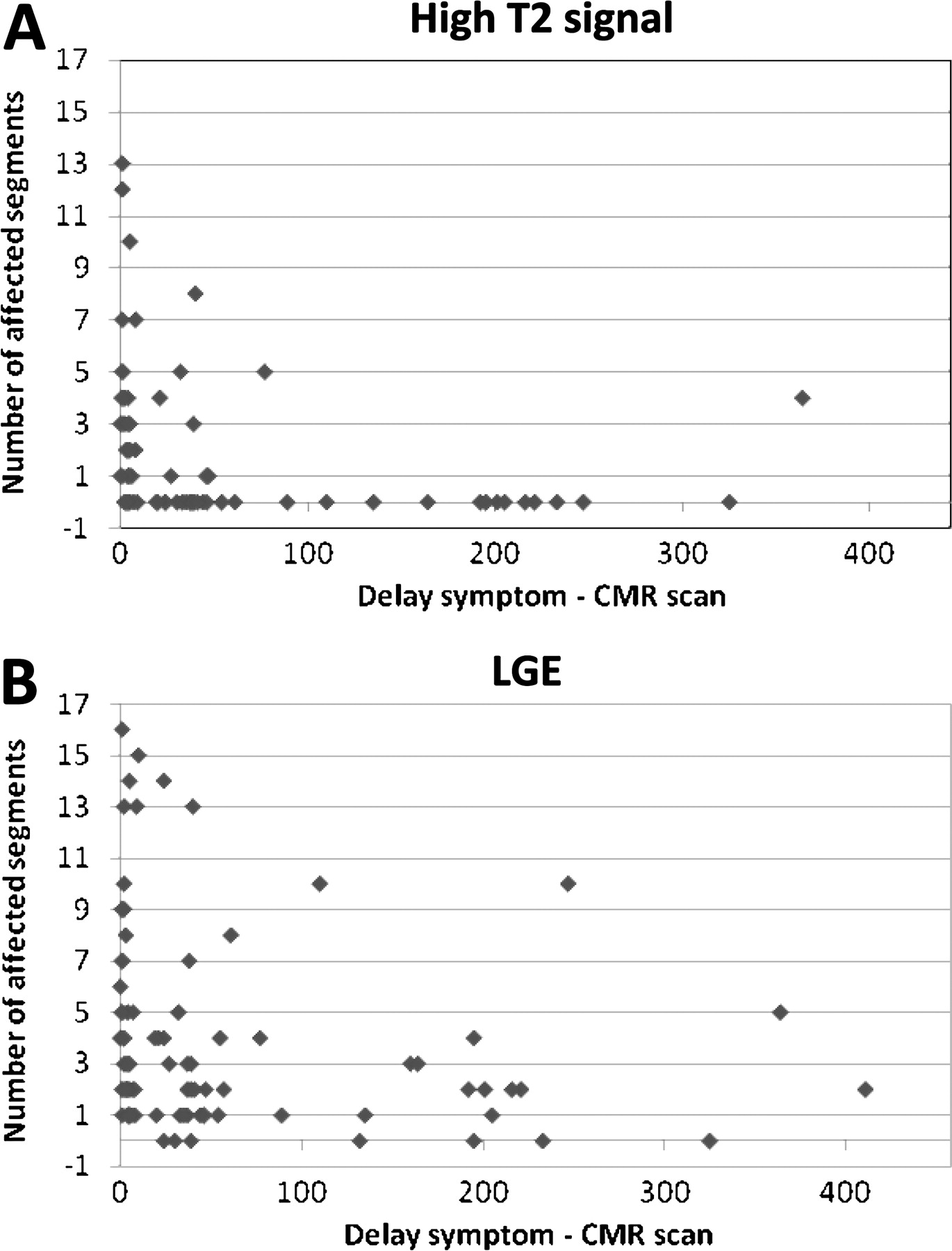
Associations between the delay from presentation to cardiac magnetic resonance (CMR) scanning and abnormal findings are shown for all scans (the analysis includes all initial and convalescent scans; n=91 for late gadolinium enhancement (LGE) and n=78 for T2). The number of myocardial segments with LGE and focal hyperintense T2 signal are shown in (A) and (B), respectively. Myocardial involvement appears to decrease with time; hyperintense T2 signals were unusual >50 days after presentation.
Follow-up scan
Twenty patients underwent a follow-up CMR scan. The initial scan was obtained with a mean delay of 4 days from presentation (range 0–10; median 3 days), and the follow-up scan was performed 76 days following presentation (range 21–221; median 45 days). The findings are summarised in table 2. There was no difference in LV volumes but there was an increase in EF (59±9 vs 62±8%, p<0.05).
Cardiac magnetic resonance findings at initial and follow-up scan (n=20)
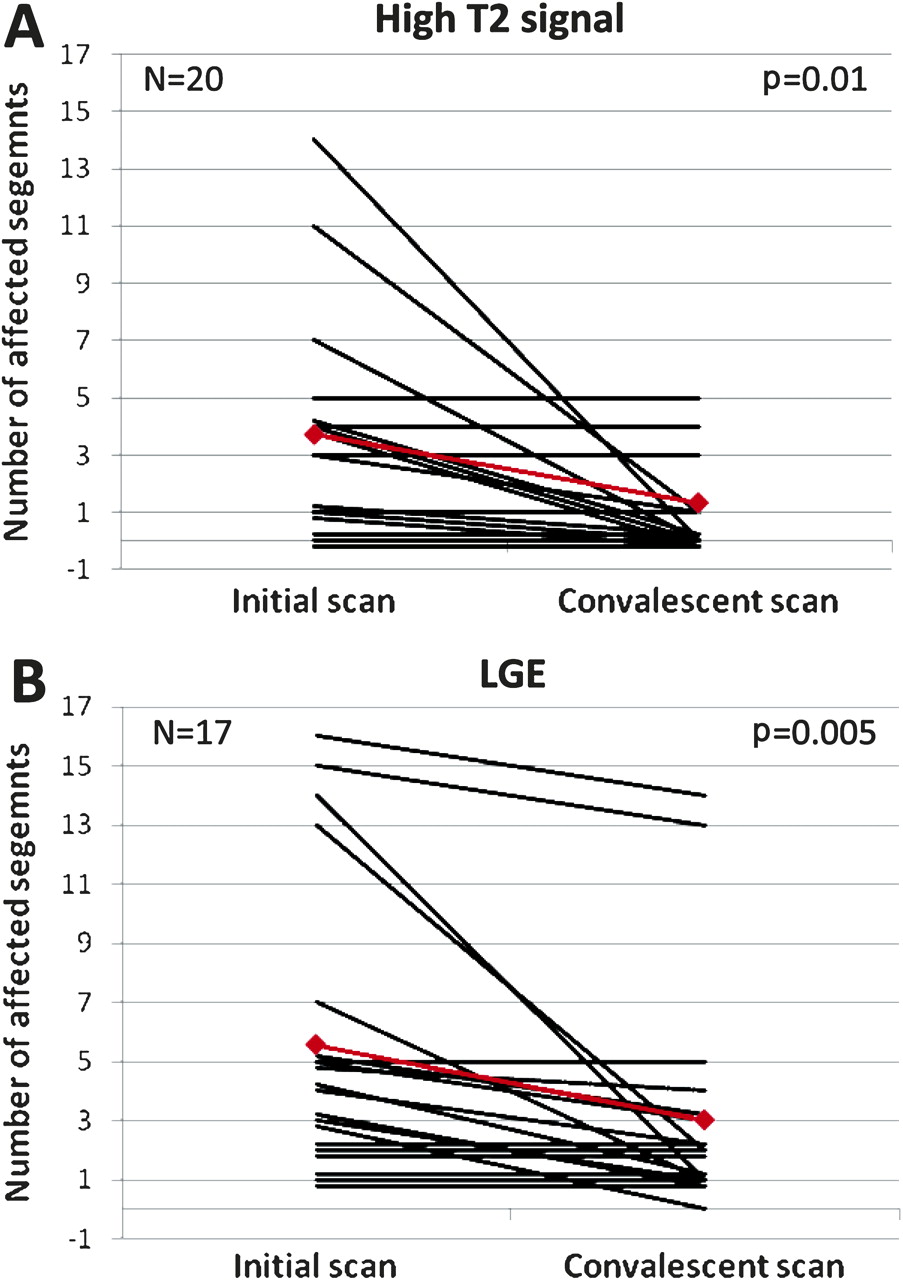
The frequency of high T2 signal decreased from 84% in the first to 39% in the second scan (p<0.01) and the number of affected segments decreased from 3.5±3.7 to 1.3±2.3 (p=0.01).The frequency of LGE was similar for both scans but the number of affected segments decreased from 5.6±4.9 to 3.0±3.8 (p=0.005). The distribution of LGE in the first and second scans is compared in figure 2C. We observed a consistent decrease in the extent of LGE with time, as depicted in figure 5. A pericardial effusion was present in five patients (25%) and persisted in four.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reduction in the number of myocardial segments with high T2 signal (A) and late gadolinium enhancement (LGE) (B) between acute (<2 weeks) and convalescent (>3 weeks) scan for individual patients. Mean values are depicted in red.
We next compared those patients with (n=7) and without (n=11) persistently high T2 signal on follow-up scanning. The delay between symptom onset and initial scan was similar (3±2 vs 3±3 days) but the delay to the follow-up scan was shorter in the group with persistent oedema (39±10, median 40 days vs 104±79, median 46 days, p<0.05).
Discussion
In our initial cohort of 79 patients, CMR performed within 2 weeks of presentation identifies a likely aetiology in most cases (figure 1). MI was diagnosed in 13% and stress cardiomyopathy in 6%. These proportions are remarkably similar to the findings in three similar studies.5–7 Our analysis has concentrated on the patients without CMR evidence of MI or cardiomyopathy; we detected evidence of myocarditis in the majority (59/64 patients (92%), representing 75% of the initial cohort). A final diagnosis was not made in only 5 (6%) of the original cohort.
Sensitivity and specificity of CMR for myocarditis
Published data on CMR findings in myocarditis are derived mainly from small series including many patients with chronic presentations of symptomatic LV systolic impairment. The results of several such studies were used to generate recommendations for the use of CMR in the evaluation of suspected myocarditis.11 These studies were validated against either clinical diagnosis or histological definitions of myocarditis. The specificity of LGE for the diagnosis of myocarditis ranged between 60% and 100% (pooled 86%) with the sensitivity far lower, between 27% and 95% (pooled 59%). For T2 imaging, the specificity was 50–100% (pooled 71%) and the sensitivity 45–100% (pooled 70%). When both T2 and LGE findings are included, the pooled data from 130 patients was considered to have a sensitivity of only 25%, but a specificity of 95%. Our study suggests that the sensitivity is greatly increased in patients presenting acutely with chest pain and raised cardiac troponin if CMR is obtained immediately after symptom onset.
Other data support this view. Baccouche et al studied patients with raised troponin and culprit-free angiograms with a combined diagnostic approach using CMR (LGE but no T2 imaging) and myocardial biopsy.7 Patients with active myocarditis as defined by the Dallas criteria were more likely to have abnormal LGE on CMR than those with borderline myocarditis. Patients with LGE also had higher elevations of serum creatine kinase.
Temporal dependence of high diagnostic sensitivity
The major contribution of the present study is the description of the extent to which the diagnostic utility of CMR for myocarditis is temporally dependent, and the importance of CMR scanning in ‘real-world’ practice in a busy ACS centre. Assomull et al report that CMR did not detect diagnostic myocardial abnormalities in 35% in a similar cohort. After excluding those patients with CMR evidence of MI or cardiomyopathy, they detected LGE evidence of myocarditis in only 59% and T2 evidence in 37%. Laraudogoitia et al report these abnormalities in 86% and 73%, respectively, of a similarly defined group, and our study detects abnormalities in 92% and 58%, respectively. These disparities may result from differences in time between presentation and scan.
We demonstrate differences between early (<2 weeks) and late CMR scans in sensitivity for the detection of the features of myocarditis. Evidence for the temporal dependence of CMR's diagnostic utility is derived from an analysis of interval between presentation and scan, and from a patient subset with serial scans. When only early scans were analysed, LGE was detected in all patients and T2 signals were abnormal in 81%. In the late scans, abnormalities were detected in 75% and 12%, respectively. In support of our findings, Laraudogoitia et al only detected hyperintense regional T2 signals in scans performed within 7 days of presentation.6 LGE patterns also alter over time in two important ways. First, a preference for lateral and apical segments becomes more evident. Second, transmural LGE resolves into a more subepicardial pattern (figure 3). Additionally, as transmural LGE was invariably associated with high T2 signal, it is likely to reflect interstitial expansion with water and does not reliably indicate regions of irreversible damage, as has been suggested.13
Importance of the correct diagnosis of myocardial infarction
For patients presenting with acute cardiac symptoms, raised serum troponin and no culprit coronary lesion, a recommendation that they receive lifelong secondary prevention is based on the possibility that the acute event resulted from undetected coronary disease.14 However, there is no evidence that lifelong secondary treatment is warranted in the majority.
Contemporary secondary prevention regimes are associated with major bleeding rates of 3.7% per annum or more,15 and pharmacological costs are estimated to be >£700 in the first year alone (UK, 2010). The risks of recurrent coronary events following denial of secondary prevention must also be balanced against the financial costs of complications, unnecessary treatment, investigations, and costs of health and employment insurance.
Importance of the correct diagnosis of myocarditis
Myocarditis presenting acutely with chest pain and normal LV function is reported to be benign.8 Few, if any, studies provide evidence for this view. The difficulty in establishing the diagnosis of myocarditis has undoubtedly contributed to the dearth of outcome data.
Sub-group analyses of prospective ACS cohorts describe high event rates, including death, in patients presenting with raised troponin and unobstructed angiograms. A sub-study of TACTICS-TIMI reports death, reinfarction or repeat hospitalisation within 6 months of the initial presentation in 6.3% of such patients.2 In those with normal angiograms and normal troponin, the event rate was 2.7%. In a larger study, Larsen et al report a 4% 1-year mortality in 273 patients with similar characteristics.1 Our findings (and those of other reports5–7)are that the majority of such patients have myocarditis. The high event rate in our cohort is more direct evidence that this condition is not benign.
Importance of serial scanning
Another novel observation is the additional specificity for a diagnosis of myocarditis resulting from serial changes in CMR abnormalities. In all cases where a second scan was performed, resolution in severity, segmental distribution and transmurality was evident (figures 3 and 5). Notably, in several cases where the acute scan demonstrated transmural LGE, a regression to an epicardial or mid-wall LGE lesion was evident in convalescent images. In our opinion, when widespread or florid abnormalities are present, their resolution on convalescent scanning provides reassurance that the outcome is unlikely to be malignant.
Future directions
Myocarditis is diagnosed in up to 20% of cases of unexpected sudden death,16–19 and viral myocarditis may be aetiologically important in up to 60% of cases of dilated cardiomyopathy.20–22 In combination with clinical follow-up, CMR findings in the acute and convalescent patient (such as florid or persistent high T2 signal) presenting with ‘ACS’ myocarditis may contribute to assessment of risks of both acute and long-term cardiac disease. A multicentre myocarditis registry or a prospective study of these patients may best provide the outcome data needed.
Clinical implications
The prognostic importance of the diagnosis of myocarditis in this group of patients is currently undefined. Future availability of CMR in acute cardiac centres will generate a growing uncertainty regarding the management of these patients that is sustained by concerns that persistent inflammation may lead to sudden death or systolic impairment. Our clinical management following a CMR diagnosis of myocarditis is therefore based on assessments intended to detect persistent inflammation or progressive systolic impairment, and the international recommendations for myocardial biopsy.23 Stable patients with preserved LV systolic function and an unchanging 12-lead electrocardiogram are discharged when serum troponin concentrations begin to decline. All patients are rescanned 8 weeks following the initial assessment and then reviewed as outpatients. Cardiac biopsy is considered for those patients with persistently raised cardiac troponin, impaired or worsening LV systolic function or where T2 imaging suggests persistent myocardial oedema. All patients are advised to avoid exercise until after convalescent review and those with impaired LV systolic function are considered for angiotensin converter enzyme inhibitor and β-blocker therapy.
Limitations
Although this is not a prospective study of the utility of CMR in culprit lesion-free ACS presentations with raised troponin, our unit's policy is to refer all such patients for CMR. In our study, CMR interpretation is not blinded. However, the scan is interpreted for evidence of missed MI, myocarditis or any other cardiac abnormalities. A blinded study would require the interpreting cardiologist to be blinded to a gold-standard diagnostic test; cardiac biopsies were not obtained in this study, and are not recommended for this indication.23
Conclusions
In acute myocarditis, CMR is more likely to detect diagnostically important evidence of myocardial damage if the scan is performed within 2 weeks of presentation. The prognostic importance of these abnormalities, their severity and any persistence is unknown and merits further study. A repeat CMR in selected individuals with equivocal early CMR findings after 4–6 weeks may be of diagnostic benefit and, in patients with very abnormal acute scans, improvements seen on follow-up scans may provide reassurance. In those with systolic impairment or when abnormal findings do not resolve, CMR targeted cardiac biopsy could be considered. However, as sustained VT and death occurred in the absence of significant LV impairment, myocarditis should not be considered benign when systolic function is normal.
In patients presenting with chest pain, ECG changes, raised troponin and apparently culprit-free coronary angiograms, CMR frequently contributes to important diagnoses (including missed MI) and may become an important component of diagnostic pathways in heart attack centres. In considering indications for secondary prevention following such admissions, CMR's ability to provide evidence for and against a diagnosis of missed MI may provide substantial safety and cost benefits.
References
Footnotes
See Editorial, p 1283
Funding This work forms part of the research themes contributing to the translational research portfolio of Barts and The London Cardiovascular Biomedical Research Unit which is supported and funded by the National Institute of Health Research.
Competing interests None.
Patient consent All patients consented to their anonymised images and clinical data to be used for educational and teaching purposes.
Provenance and peer review Not commissioned; externally peer reviewed.