Article Text

Abstract
Aims: Pancreatic adenocarcinoma is an aggressive gastrointestinal malignancy with only a few long-term survivors even after radical surgery. Patients with ampullary cancer have a better prognosis but adjuvant therapy needs further improvement. Epithelial cell adhesion molecule (Ep-CAM) is strongly expressed in a variety of epithelial cancers and represents a promising target for immunological tumour therapy. Thus, the aim of this study was to investigate Ep-CAM expression and its potential prognostic impact in pancreatic and ampullary carcinomas.
Methods: Ep-CAM expression was investigated retrospectively by immunohistochemistry in paraffin-embedded primary tumour tissue samples from a series of consecutive patients with pancreatic (n = 153) and ampullary cancer (n = 34).
Results: Ep-CAM overexpression was observed in 85 of 153 pancreatic cancer specimens (56%) and in 29 of 34 ampullary cancer samples (85%). Overall, Ep-CAM failed to be an independent prognostic marker. However, subgroup analyses showed that Ep-CAM overexpression correlated with shorter overall survival among patients with ampullary cancer and advanced stage pancreatic cancer. In the latter subgroup, survival gradually worsened with increasing Ep-CAM scores. Furthermore, in ampullary cancer, Ep-CAM overexpression was found to correlate with tumour stage.
Conclusions: Ep-CAM overexpression was detectable in the majority of cases with pancreatic and ampullary cancer. Therefore, Ep-CAM represents an attractive target for immune-based therapeutic interventions in these tumour entities. However, the prognostic value of Ep-CAM overexpression remains undetermined.
- epithelial cell adhesion molecule
- Ep-CAM
- pancreatic cancer
- ampullary cancer
Statistics from Altmetric.com
Pancreatic cancer is an aggressive malignancy characterised by rapid progression and dismal prognosis. The majority of patients present with unresectable tumour due to local extension or metastatic disease, and the median survival after diagnosis is 4–8 months.1 At present, pancreaticoduodenectomy provides the only means of cure, and even patients with resectable disease have 5 year survival rates of only 15–20%.2 Despite the introduction of new chemotherapeutical agents and combination regimens, pancreatic cancer remains a chemoresistant tumour. Therefore, there is a need for the identification of clinically relevant molecular targets for novel therapeutic approaches.
Ampullary cancer may originate from the pancreas, duodenum, distal common bile duct or from the ampulla of Vater itself. In contrast to primary carcinoma of the pancreas, ampullary cancer is rather uncommon and has a better outcome after resection but clinicopathological studies are limited to series with small sample size. Clinical features and anatomical locations may be similar to those of pancreatic cancer, as are the therapeutic approaches.
Epithelial cell adhesion molecule (Ep-CAM; 17-1A, GA733-2) is a calcium-independent homophilic cell adhesion molecule with an apparent molecular mass of 39–42 kDa.3 It is expressed in the majority of healthy epithelial tissues and in a subset of human carcinomas. Based on these findings, Ep-CAM has attracted major interest as a target for cancer immunotherapy.4–6 In fact, anti-tumour responses have been observed in a wide variety of in vitro and in vivo models6–8 as well as in cancer patients following Ep-CAM-targeted treatment.9 Thus, it is important to investigate tumours in terms of frequency and intensity of Ep-CAM expression to evaluate which malignancies may be susceptible to anti-Ep-CAM treatment.
Ep-CAM expression is unknown in pancreatic and ampullary cancer. In this paper we have studied Ep-CAM expression and its association with survival by retrospective analysis of histological specimens and clinical records in our patients.
METHODS
Patients and tissue samples
The study was conducted according to the regulations of the local ethics committee and Austrian law. A total number of 153 consecutive patients with pancreatic ductal adenocarcinoma and 34 patients with ampullary carcinoma diagnosed between 1987 and 2003 at the Department of Pathology, Medical University of Innsbruck, were included in this retrospective study. Patients with other pancreatic malignancies, such as intraductal papillary mucinous adenocarcinoma, acinar cell carcinoma and malignant endocrine tumours, and tissue samples obtained from distant metastases, were excluded. All tumours were reclassified on H&E-stained slides and histological type and tumour grade were reassessed by a pathologist (AT) using standard diagnostic criteria. Clinical data were obtained by reviewing the charts and contacting the physicians-in-charge. Tumours were histologically classified according to the World Health Organization classification and staged according to the International Union Against Cancer (UICC) tumour-node-metastasis classification.10 11 For subgroup analysis, patients were divided into localised (T1 or T2 tumours without lymph-node metastases) and advanced disease (UICC stage ⩾II). Overall survival was defined as the period of time from initial diagnosis to death or last contact (ie, date of last follow-up visit).
Immunohistochemistry
Ep-CAM expression was determined by immunohistochemistry on paraffin-embedded primary tumour tissue samples using the murine monoclonal antibody ESA (NovoCastra, Medac GmbH, Hamburg, Germany) as described previously.12 Breast cancer samples with different Ep-CAM expression (no, low, moderate or high expression) and breast cancer cell lines (Ep-CAM positive, MCF-7; Ep-CAM negative, Hs-578T) were used as positive and negative controls. In addition, 10 samples of normal pancreatic tissue were collected from surgical specimens obtained from patients at the Innsbruck Medical University. Ep-CAM overexpression was evaluated by two independent observers (PO and DF) using light microscopy in a blinded fashion. Discordant cases were re-evaluated on a double-headed microscope to achieve a consensus. Antigen expression was defined as the presence of specific staining on surface membranes of tumour cells. Ep-CAM overexpression was evaluated for each tissue sample by calculating a total immunostaining score as the product of a proportion and intensity score. The proportion score described the estimated fraction of positive-stained tumour cells (0, none; 1, <10%; 2, 10–50%; 3, 51–80%; 4, >80%). The intensity score represented the estimated staining intensity (0, no staining; 1, weak; 2, moderate; 3, strong). The total score ranged from 0 to 12. As described previously, Ep-CAM “overexpression” was defined as a total score >4.12
Statistical analysis
Statistical analysis was performed using the Statistical Package of Social Sciences (SPSS, V.10.0, Chicago, Illinois, USA). The association between Ep-CAM expression and clinicopathological variables were assessed by the χ2 test. Survival rates were calculated by using the Kaplan–Meier method and compared by the log-rank test. Factors shown to be of prognostic significance in the univariate models were evaluated in a multivariate Cox regression model. p<0.05 was considered statistically significant.
RESULTS
Patient characteristics
Demographic data and tumour characteristics are summarised in table 1. At the time of last clinical follow-up (June 2005) 156 (84%) patients had died, and 31 (16%) patients were still alive. Median overall survival was 7 months (range, 1–134) for patients suffering from pancreatic cancer, and 19 months (range, 3–119) for patients with ampullary cancer (p<0.01). Most patients (84%) underwent primary surgical intervention, including 124 patients with pancreatic cancer (29 patients were considered inoperable) and 33 patients with ampullary cancer (one inoperable). Palliative surgery included palliative bypass or endoscopic bile duct stenting. Patients received standard therapy, based on their clinical stage and performance status. In 18 patients with pancreatic and three patients with ampullary cancer, exact staging according to UICC was not feasible.
Immunohistochemistry
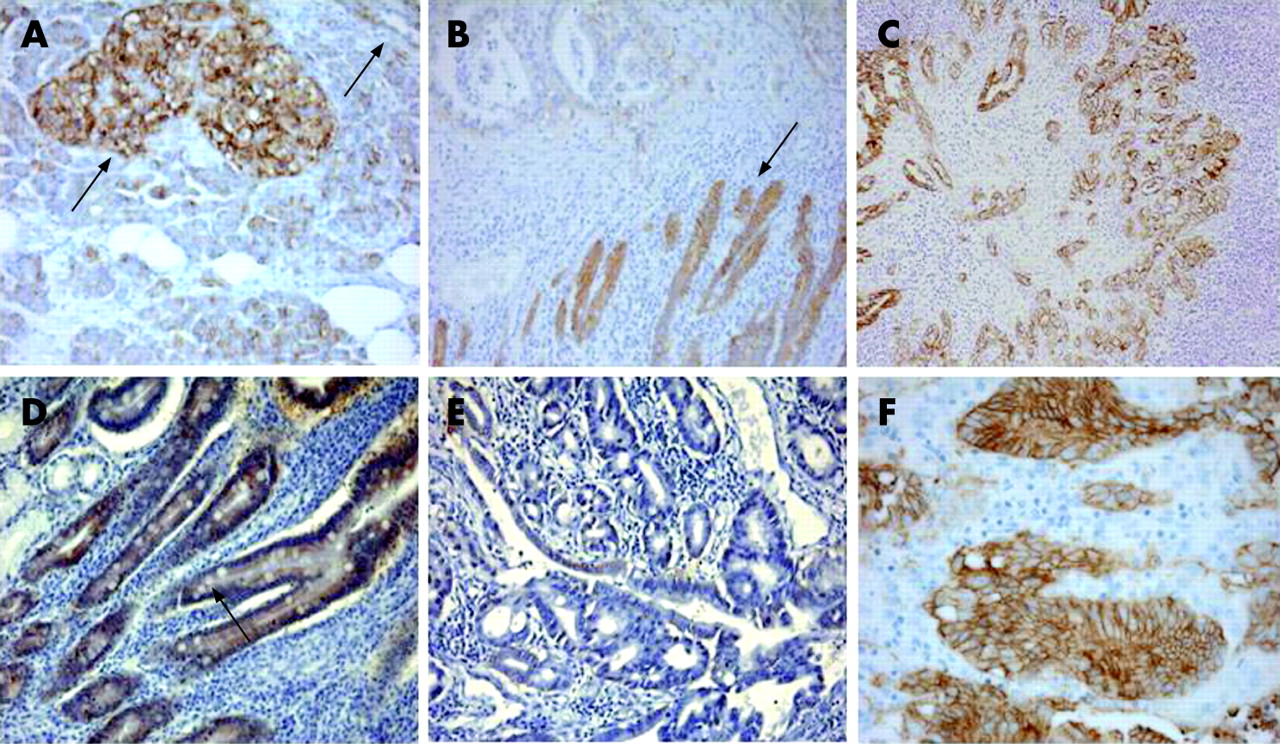
As reported previously, islets of Langerhans displayed a strong Ep-CAM staining,13 whereas in normal pancreatic epithelium Ep-CAM expression was weak to moderate (fig 1A). In contrast, a moderate-to-strong homogenous membranous expression of Ep-CAM was noted in most carcinoma specimens (fig 1B,C). Of note, in pancreatic cancer, strong Ep-CAM expression (score 9–12) was found in 35 of 153 (23%) cases, moderate expression (score 6–8) in 50 (33%) cases, and weak expression (score 1–4) in 68 (44%) cases. No tumour lacked Ep-CAM expression. In ampullary cancer, 15 of 34 (44%) cases showed strong expression of Ep-CAM, 14 cases (41%) stained moderately, and five cases (15%) were weakly positive for Ep-CAM (fig 1D–F). Thus, according to previously defined criteria,12 Ep-CAM was found to be overexpressed in 85 of 153 (56%) cases of pancreatic cancer, and in 29 of 34 (85%) cases of ampullary cancer.

Clinicopathological variables and patient survival
By univariate analysis we compared Ep-CAM overexpression to age, sex, tumour grading and stage (table 2). Ampullary cancer patients with advanced disease (UICC stage ⩾II) demonstrated a significantly higher Ep-CAM expression than patients with localised disease (UICC stage I, p<0.01). In contrast, no correlation between Ep-CAM expression and clinical or pathological features was found in pancreatic cancer.
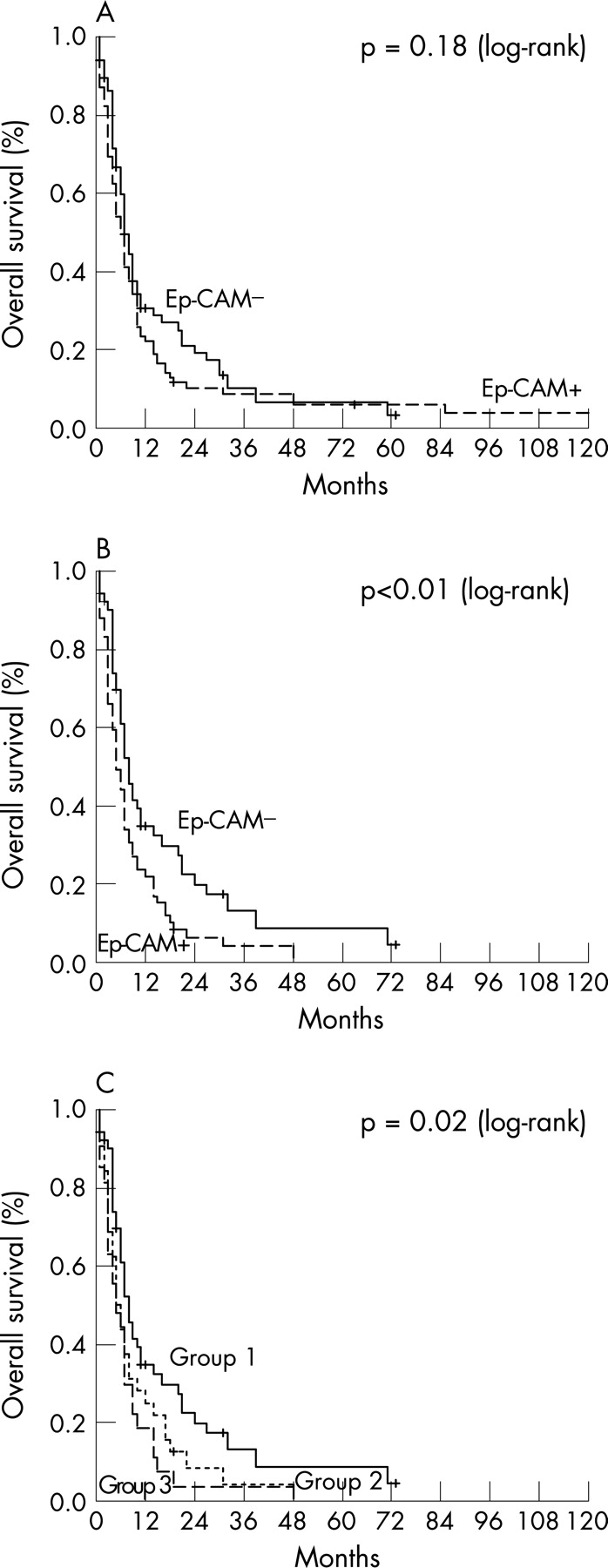
To assess the impact of clinicopathological features and Ep-CAM overexpression on survival we used Kaplan–Meier analysis and the log-rank test for censored survival data. Consistent with previous findings, patients with ampullary cancer had a significantly better overall survival than patients suffering from pancreatic cancer. At 120 months of follow-up, 29% of patients with ampullary cancer were still alive compared with 4% of patients with pancreatic cancer (p<0.01). For the total cohort of pancreatic cancer patients, only age (p = 0.03) and tumour stage (p = 0.01) were of prognostic significance, whereas sex, histological grade and Ep-CAM overexpression (p = 0.18, fig 2A) were prognostically not relevant. However, in the subgroup of patients with advanced disease, Ep-CAM overexpression was significantly correlated with shorter overall survival (p<0.01, fig 2B). Furthermore, in this subgroup overall survival decreased significantly with increasing Ep-CAM scores (p = 0.02, fig 2C). Multivariate analysis including age, stage and Ep-CAM overexpression (table 3) identified only the presence of advanced disease as an independent prognostic marker for pancreatic adenocarcinoma (p = 0.01; relative risk, 1.9; 95% confidence interval, 1.1 to 3.3). In patients with ampullary carcinoma, Ep-CAM overexpression (p<0.01, fig 3) and advanced stage (p = 0.01) were associated with a worse outcome. However, due to the small sample size, multivariate analysis was omitted.


{kind=link}
{kind=link}
{kind=link}
Take-home messages
This is the first study to assess the expression of Ep-CAM, an epithelial cell adhesion molecule, in pancreatic and ampullary cancer.
We show that Ep-CAM is expressed or overexpressed in nearly all cases of pancreatic and ampullary cancer.
Although we found Ep-CAM overexpression to correlate with shorter survival among subgroups of patients with advanced stage pancreatic cancer, we were not able to identify Ep-CAM overexpression as an independent prognostic marker.
Taken together, we provide evidence that Ep-CAM may be a useful therapeutic target for immune-based therapy of pancreatic and ampullary cancer.
DISCUSSION
This is the first report on Ep-CAM expression and its prognostic relevance in pancreatic and ampullary cancer. Our primary findings were as follows: strong Ep-CAM expression (“overexpression”) was detectable in the majority of specimens of pancreatic (56%) and ampullary cancer (85%). Univariate analyses were suggestive of worse survival for patients with Ep-CAM overexpression in ampullary and advanced pancreatic cancer. In multivariate analyses, however, Ep-CAM overexpression failed to be an independent prognostic marker.
One potential way to improve outcome in cancer therapy may be by targeting defined proteins expressed on the malignant cells.14 The finding that Ep-CAM is homogenously overexpressed in the majority of patients may render this molecule an attractive target for immunological approaches in pancreatic and ampullary cancer. In patients suffering from colorectal cancer, substantial anti-tumour responses following treatment with the Ep-CAM-specific monoclonal antibody edrecolomab have been reported. In that randomised placebo-controlled clinical trial involving 189 patients, the investigators found a significant improvement of overall and disease-free survival, significantly reduced recurrence rate and reduction of distant metastases in the edrecolomab group.9 Recently, novel and more potent Ep-CAM-specific humanised monoclonal antibodies, MT201 (adecatumumab), ING-1 and catumaxomab, have been developed and their anti-tumour activity has been demonstrated in various animal models6 7 and early clinical trials.15 Recently, Mosolits et al were able to demonstrate that a recombinant Ep-CAM peptide vaccine is safe and induces long-lasting humoral and cellular Ep-CAM-specific immune responses in cancer patients.16 Promising clinical results have come from a randomised phase 2 trial comprising 240 patients with advanced epithelial cancers in which anti-Ep-CAM vaccination with the IGN101 antibody resulted in a significant reduction of circulating tumour cells and prolonged survival for metastatic rectal cancer patients.17 18
The exact pathophysiological role of Ep-CAM in cancer is still unclear. There is, however, growing evidence that Ep-CAM expression contributes to a more aggressive type of cancer.19 20 Overexpression of Ep-CAM exerts a growth-stimulating effect on malignant cells resulting in increased proliferation, enhanced tumour cell migration and invasive potential by antagonism of E-cadherin.3 21 22 Our results are in keeping with these data, since Ep-CAM overexpression was associated with inferior survival in patients with ampullary and advanced pancreatic cancer. In addition, overall survival gradually worsened with increasing Ep-CAM expression scores, a finding that has also been observed in a similar study performed on breast cancer specimens.23 This parallels in vitro studies conducted by Munz et al. who found a close correlation between Ep-CAM expression, c-myc induction and consequently direct stimulation of tumour cell proliferation in various cancer cell lines.21 However, due to the limitations inherent in retrospective analyses, the prognostic value of Ep-CAM overexpression needs to be validated in larger, prospective studies.
We recently showed that Ep-CAM overexpression predicts poor survival in gallbladder cancer.24 Considering that biliary tree, duodenum, pancreas and ampulla of Vater originate from a common endodermal bud,25 we hypothesised a prognostic impact of Ep-CAM expression in ampullary cancer as well. Indeed, all tumour specimens obtained from patients with advanced-stage ampullary cancer displayed Ep-CAM overexpression. The five patients with Ep-CAM-negative tumours all had limited disease and showed an excellent outcome. However, the numbers are too small to draw firm conclusions from these data.
In summary, we show for the first time that the Ep-CAM antigen is expressed in the majority of pancreatic and ampullary carcinomas. Thus, Ep-CAM may be an attractive target for active and passive immunotherapy in patients with these tumour entities.
Acknowledgments
We thank Ines Tschörner for excellent technical assistance.
REFERENCES
Footnotes
Funding: This work was supported by the Tiroler Verein zur Förderung der Krebsforschung.
Competing interests: None.