Article Text

Abstract
Aims—To investigate the expression of catenins (α, β, and γ) in non-small cell lung carcinoma (NSCLC) and its relation to clinicopathological factors and prognosis.
Methods—The expression of catenins was analysed immunohistochemically in 261 patients with resected NSCLC, diagnosed between 1978 and 1996 in eastern Finland. The cell proliferation index of the tumours was analysed by means of an image analyser. The staining results were compared with clinicopathological characteristics and survival.
Results—Normal catenin staining was found significantly more often in adenocarcinomas than in squamous cell carcinomas or anaplastic/large cell carcinomas. Reduced staining of α-catenin, β-catenin, and γ-catenin was related to poor differentiation of the tumour. The tumours with reduced staining of β-catenin or γ-catenin often had higher cell proliferation activity. Nuclear staining of β-catenin and γ-catenin was found in 16 (7%) and 29 (13%) cases, respectively. This nuclear staining correlated directly with increased cell proliferation and inversely with membranous staining. In survival analyses the predictors of overall and disease free survival were stage and tumour type. The expression of catenins did not affect survival.
Conclusions—The expression of α-catenin, β-catenin, and γ-catenin is related to histological type and differentiation in NSCLC, although catenins have no independent prognostic value. However, this study supports the important role of the nuclear accumulation of β-catenin and γ-catenin in highly proliferative cells.
- catenin
- lung cancer
- proliferation
- differentiation
Statistics from Altmetric.com
E-cadherin–catenin complexes regulate the functional integrity of the epithelium by mediating specific intercellular adhesion.1 The cytoplasmic domain of E-cadherin forms complexes with β-catenin or γ-catenin, which in turn bind to α-catenin, which anchors the complex to the cytoskeleton. The presence of all catenins is essential for the full adhesive function of the cell. In addition, catenins are also involved in cell proliferation, differentiation, and migration.2
α-Catenin might serve as an invasion suppressor molecule, and reduced expression of α-catenin has been related to poor differentiation of tumours, infiltrative growth, and lymph node metastasis.3 Furthermore, the disappearance of membranous α-catenin is predictive of an unfavourable outcome in prostate, ovarian, and colorectal cancer.4–6 Similarly, reduced β-catenin expression is related to poor differentiation and more aggressive tumour growth,7 although not all reports are in agreement.3, 8, 9 β-Catenin forms a complex with the adenomatous polyposis coli (APC) protein, which is mutated in most human colon cancers.10 As a consequence, β-catenin expression has been observed in the nucleus and the cytoplasm, instead of the usual localisation on the cell membrane.10 Cytoplasmic or nuclear accumulation of β-catenin seems to be associated with the progression of colorectal and oesophageal cancers.11, 12 Although the role of γ-catenin in cadherin–catenin complex formation is not firmly established, it has been shown that the association of E-cadherin with α-catenin and β-catenin is not sufficient to modify the behaviour of highly malignant cells, and γ-catenin is essential in this context.13 Altered expression of γ-catenin has been correlated with shortened survival in patients with bladder cancer.14 However, its role in the progression and differentiation of many tumours is not clear.
Lung cancer is still a leading cause of death in men.15 To date, despite an active search for new prognostic biomarkers, the stage of disease is still the most valuable prognostic factor in non-small cell lung cancer (NSCLC).16 The few studies concerning the prognostic role of catenins in NSCLC have found the reduced expression of β-catenin and γ-catenin to be associated with an unfavourable outcome.17, 18 However, correlations with other clinicopathological factors have not been found.17, 19 Therefore, we studied the expression of all three catenins (α, β, and γ) in a large sample of resected NSCLC specimens and compared the results with the clinicopathological features and survival of the patients.
Materials and methods
PATIENTS AND FOLLOW UP
The study population comprised 261 patients with resected NSCLC treated in eastern Finland from 1978 to 1996 (table 1). There were 239 men and 22 women in the study cohort. The mean age of the patients was 63 years. Most patients (222) underwent either radical lobectomy (50% of cases) or pneumonectomy (35% of cases). Palliative resection was performed in 10% of the patients and explorative thoracotomy only in 5% of the patients. None of the patients received radiotherapy or chemotherapy before surgery. Postoperative radiotherapy was given to 61 patients and chemotherapy to 11. TNM classification and stage of the disease20 were determined by reviewing radiological examinations, findings during surgery, and the histopathological evaluation of the tumour. Follow up was performed regularly by a senior physician according to routine protocol. All clinical data were collected retrospectively by reviewing the patients' files.
Clinicopathological characteristics of the patients
HISTOPATHOLOGICAL EVALUATION
The histological diagnosis and grade of differentiation were re-evaluated (V-MK and SH) using haematoxylin and eosin stained sections according to the WHO classification.21 There were 163 squamous cell carcinomas, 68 adenocarcinomas, and 30 anaplastic/large cell carcinomas in our study. The most representative slide was used in the immunohistochemical analyses.
IMMUNOHISTOCHEMISTRY
Catenins
Briefly, the paraffin wax embedded samples were cut into 5 μm thick sections and dewaxed in graded alcohols. For the antigen retrieval, the sections were heated in a microwave oven for three periods of five minutes in Tris/HCl buffer, pH 9.7 (α-catenin), or citrate buffer, pH 6.0 (β-catenin and γ-catenin). The slides were washed with phosphate buffered saline (PBS) for two times five minutes and endogeneous peroxidase activity was blocked by 5% H2O2 for five minutes. The sections were washed twice with PBS and treated with 1.5% normal serum (ABC Elite kit; Vector, Burlingame, California, USA). The primary antibody (Transduction Laboratories, Lexington, Kentucky, USA) was used at a dilution of 1/200 (in 1% bovine serum albumin in PBS (α-catenin), 1/1000 (β-catenin), or 1/100 (γ-catenin). Slides were incubated overnight at 4°C, washed with PBS, and treated with the biotinylated secondary antibody and avidin–biotin peroxidase reagent (Vector). Diaminobenzidine was used as a chromogen. The slides were washed with PBS, lightly counterstained with haematoxylin, dehydrated, cleared, and mounted in Depex (PDH, Poole, Dorset, UK). A sample of normal colonic mucosa, known to be positive for all catenins, was used as a positive control. In the negative controls, the same samples were stained without adding the primary antibody.
Ki-67
To determine the proliferative activity of the tumour, anti-Ki-67 (MIB1; Immunotech, Marseille, France) was used as a primary antibody, diluted 1/200. The indirect ABC technique was used as described above.
EVALUATION OF STAINING
All samples were evaluated (RP, PH, and V-MK) unaware of the clinical data. In the case of disagreement (less than 10% of the cases) the slides were reviewed again and a consensus was reached. The staining reaction localised on the cell membranes was graded into three groups according to the percentage of the positively stained carcinoma cells as follows: < 10%, 10–90%, and ≥ 90% of the tumour cells showing a positive staining pattern. Tumours showing 90% or more positively stained cells were categorised as normally stained, others were classified as reduced.22 Nuclear staining of β-catenin and γ-catenin was recorded as positive or negative. In positive samples nuclear staining was seen in more than 20% of cancer cells.
For the Ki-67 staining, the percentage of the stained nuclei (proliferation index; PI) was determined by a continuous scale using the CAS 200 (Becton Dickinson, Elmhurst, Illinois, USA) image analyser as described previously.23 The data were available for analysis from datasheets of our previous study.24
STATISTICAL ANALYSIS
SPSS version 8.0 was used in the analyses. The Mantel-Haenzel or Pearson χ2 test, when appropriate, was used to clarify the relation between staining results and other variables studied. The cell proliferation associated with catenins was analysed with Kruskall-Wallis and Mann-Whitney U tests. Overall (OS) and disease free survival (DFS) were estimated by means of the Kaplan-Meier test and Cox's multivariate hazards model. In DFS analyses only the patients who were treated with radical resection of tumour were included. Deaths by any other cause than lung cancer were considered as censored events—corrected survival rates were used.
ETHICS
Our study plan was approved by the ethical committee of the Kuopio University Hospital and the Finnish Ministry of Social Affairs and Health.
Results
Two hundred and thirty one samples were immunostained successfully for α-catenin, 229 for β-catenin, and 231 for γ-catenin. Some samples were discarded because of technical problems, such as partial folding of the tissue section or lack of invasive carcinoma in the section. The distribution of clinicopathological characteristics (stage, sex, grade, Karnofsky scale, histological type of tumour) among the patients with tissue samples for immunohistochemistry did not differ from the original patient group (n = 261). Benign bronchial glands showed normal staining patterns for α-catenin, β-catenin, and γ-catenin. In addition, normal staining reactions for all catenins were found in the bronchial pseudostratified columnar epithelium and basal cells.
STAINING OF CATENINS AND CLINICOPATHOLOGICAL PARAMETERS
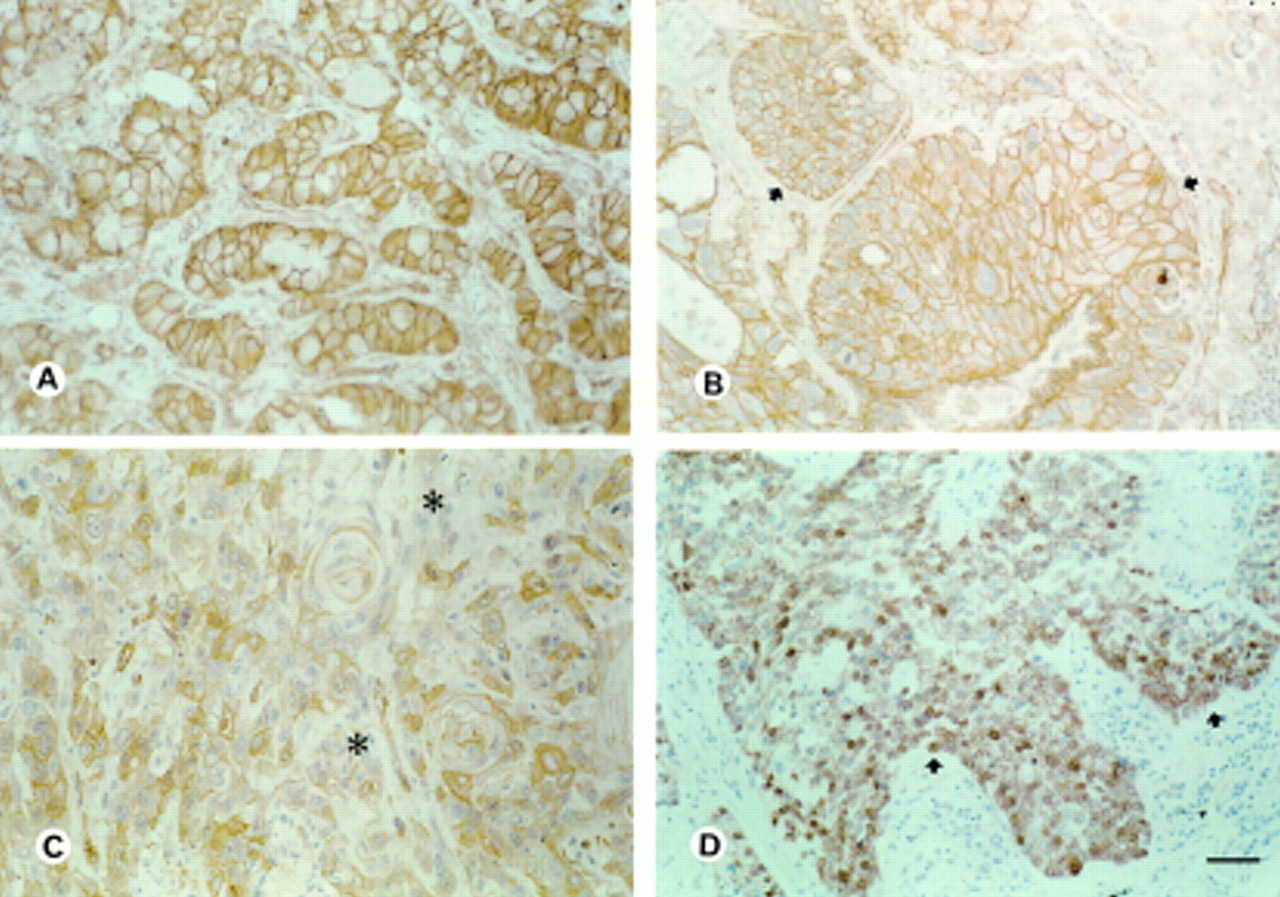
Table 2 summarises the results. Normal staining for α-catenin, β-catenin, and γ-catenin was found significantly more often in adenocarcinomas (62%, 66%, and 58% of cases, respectively) than in squamous cell or anaplastic/large cell carcinomas (p < 0.0001 for all; fig 1A and B; table 2). Poorly differentiated tumours more often showed reduced staining for all catenins (p = 0.005, p = 0.007, and p = 0.005 for α-catenin, β-catenin, and γ-catenin, respectively; fig 1C). Nuclear staining of β-catenin and γ-catenin was found in 16 (7%) and 29 (13%) cases, respectively, and was seen more often in squamous cell carcinomas (11 cases with β-catenin and 24 cases with γ-catenin) than in adenocarcinomas or anaplastic/large cell carcinomas. Nuclear staining correlated inversely with the membranous staining pattern (p = 0.001 and p = 0.0003, respectively; fig 1D).
Distribution of staining of different catenins as related to clinicopathological factors
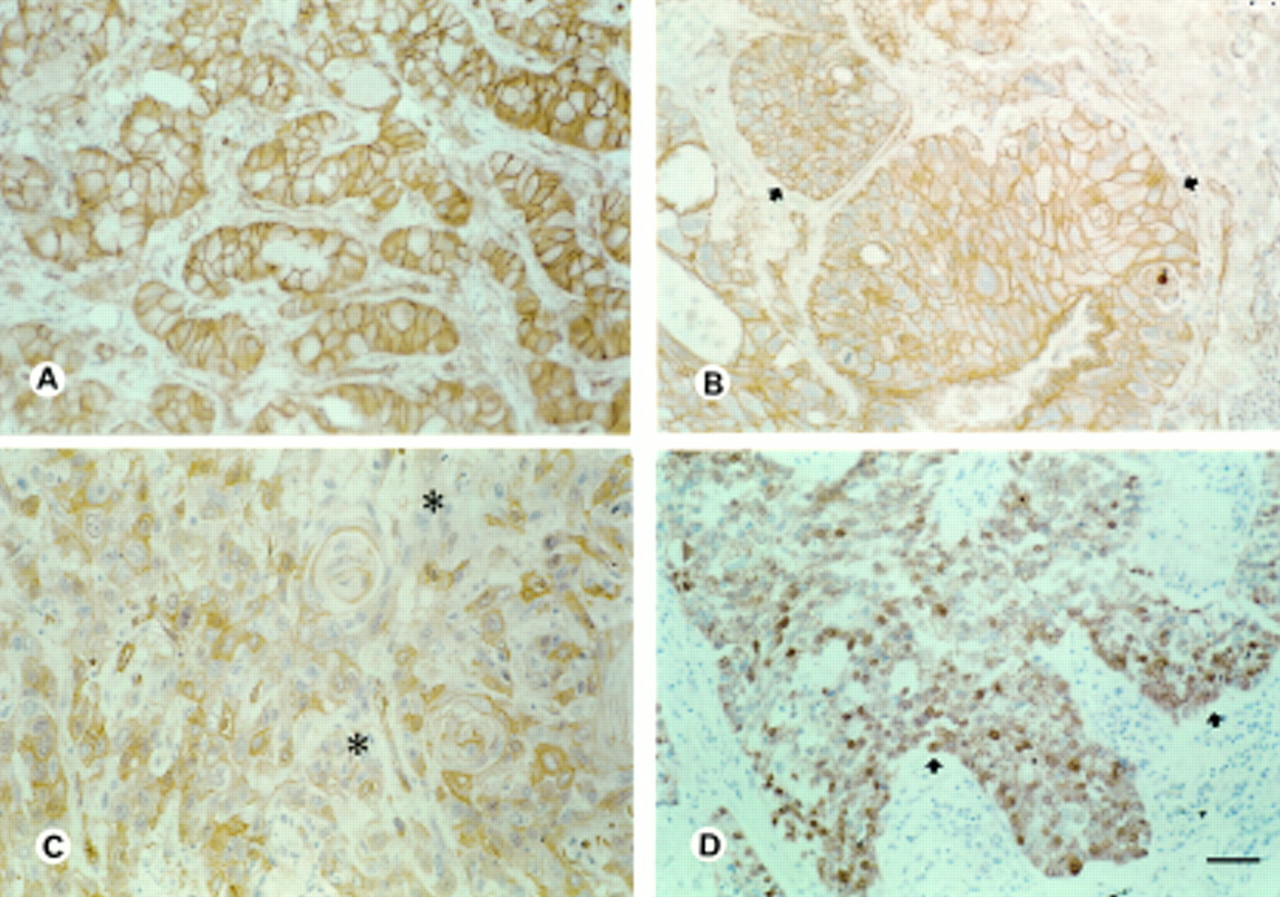
(A) Normal (≥ 90%) membranous expression of α-catenin in bronchial adenocarcinoma. (B) Normal expression (arrows) of α-catenin in squamous cell carcinoma. (C) Reduced expression (< 90%, asterisks) of β-catenin in squamous cell carcinoma. (D) Nuclear expression (arrows) of β-catenin in poorly differentiated squamous cell carcinoma. Bar, 50 μm.
CELL PROLIFERATION
Tumours with reduced β-catenin or γ-catenin staining had higher PI values (p = 0.0001 for β-catenin; p = 0.006 for γ-catenin) than did those with a normal staining pattern. Furthermore, nuclear positivity for β-catenin and γ-catenin was associated with a higher PI (p = 0.01 and p = 0.002, respectively). α-Catenin staining was not related to cell proliferation. Moreover, PI was associated with tumour type (p = 0.001) and grade (p = 0.004).
SURVIVAL ANALYSIS
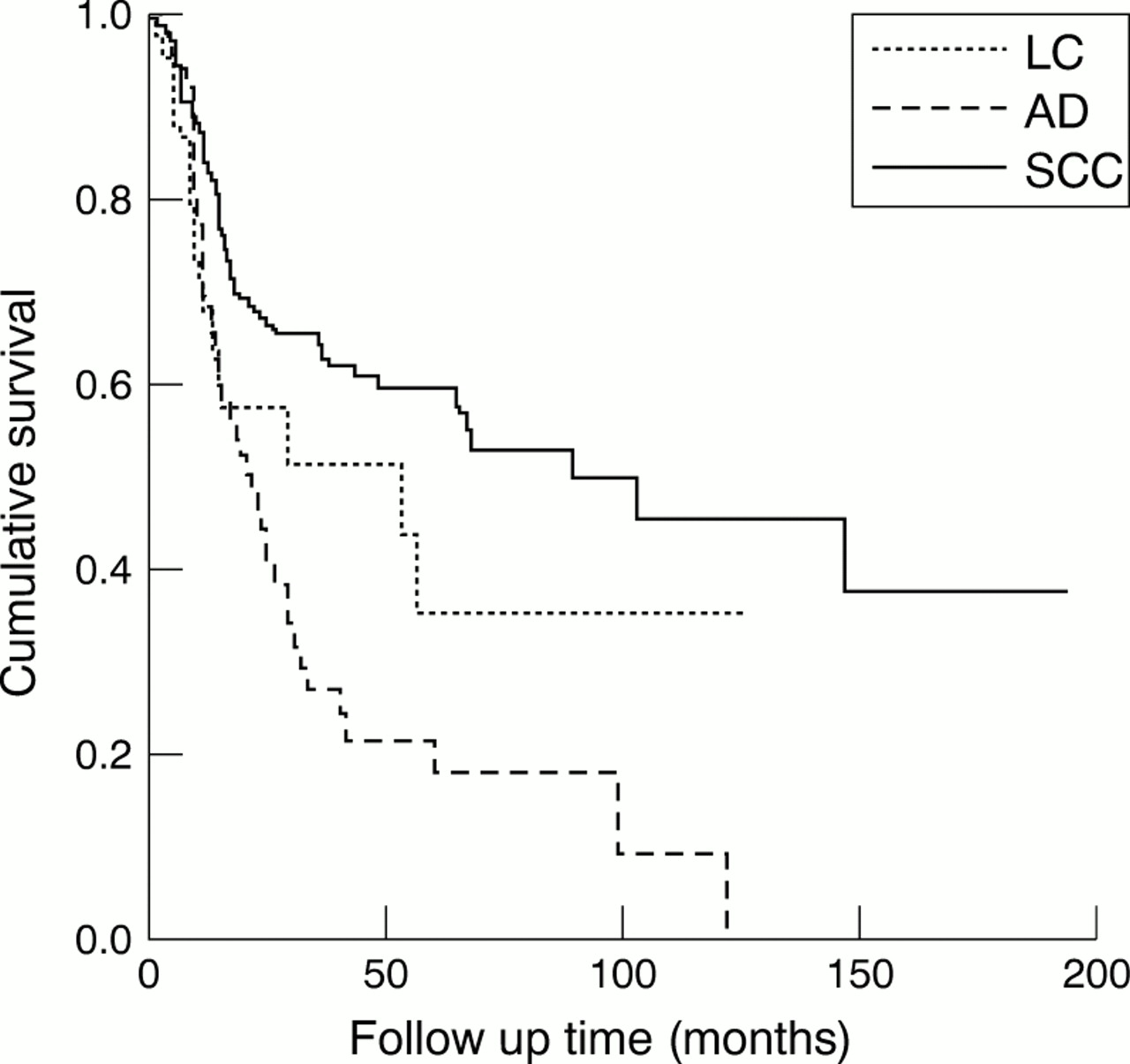
At the end of follow up 136 (52.1%) patients had died of lung cancer and 56 (21.5%) were alive. A recurrent tumour was noted in 124 cases (47.5%) during follow up. In univariate survival analysis, more advanced stage (II–IV) was a sign of poor OS (p = 0.0006). Patients with adenocarcinoma or large cell/anaplastic carcinoma had poorer OS than did patients with squamous cell carcinoma (p = 0.0003). Similarly, the stage (p = 0.006) and histological type of the tumour (p = 0.0001) significantly predicted DFS (fig 2). The expression of catenins did not predict survival. In Cox's multivariate analysis including stage and histological type of tumour, both retained their independent prognostic value to predict OS and DFS (p < 0.0005 for both).

{kind=link}
{kind=link}
In disease free survival analysis there was a significant difference in survival between different histological subtypes of non-small cell lung carcinoma (p = 0.0001). AD, adenocarcinoma; LC, large cell/anaplastic carcinoma; SCC, squamous cell carcinoma.
Discussion
Alterations in E-cadherin–catenin complexes act as an important link in the progression of different cancers.13 Lung cancer is the most frequent cancer worldwide, and despite some downward trends in mortality prognosis remains poor.15 Few studies have investigated the prognostic value of catenins in lung cancer.18, 19 In our present study, we investigated the distribution of different catenins in a large population of patients with resected NSCLC. Altered expression of catenins was found to correlate with the tumour type, with anaplastic/large cell and squamous cell carcinomas more often showing reduced staining of all catenins compared with adenocarcinomas. In addition, reduced staining of catenins was often seen in poorly differentiated tumours. Furthermore, nuclear staining of β-catenin and γ-catenin was related to increased proliferative activity of the tumour.
The distribution of catenins seems to be related to tumour type. Previous results indicate that lung adenocarcinomas often show normal staining for catenins, which supports our observations.19 Squamous cell carcinomas at different localisations show variable staining of catenins, although staining is mostly reduced.22, 25, 26 In many human cancers, reduced expression of α-catenin and β-catenin has been associated with poor tumour differentiation,27–29 which is in line with our present study. In addition, lack of expression of α-catenin and β-catenin has been shown to correlate with a more advanced stage in laryngeal, ovarian, and bladder cancers.5, 27, 29 In NSCLC, reduced expression of E-cadherin has been associated with increased lymph node metastases,30 but the expression of α-catenin and γ-catenins has not been related to TNM classification of the tumour,17, 19 a finding that is supported by our study.
In our study, increased proliferative activity of the tumour was associated with reduced expression of β-catenin and γ-catenin. This supports the theory that a reduction in the expression of catenins is a sign of more aggressive tumour behaviour.3 However, a similar relation between cell proliferation and reduced expression of catenins was not found in some previous studies.5, 31 Furthermore, the tumours in our series that showed nuclear β-catenin staining also had significantly higher PI values. According to recent studies, the nuclear accumulation of β-catenin is a consequence of the disturbance of the system that normally degrades cytosolic β-catenin.10 Nuclear β-catenin interacts with the Wnt/lef transcription pathway, resulting in changes in gene expression and cell differentiation during the malignant process.10 Recently, Nhieu and colleagues32 found an association between cell proliferation and nuclear accumulation of β-catenin in hepatocellular carcinoma, which is in agreement with our findings. Interestingly, we found that nuclear staining of γ-catenin was also related to increased cell proliferation. However, the role of γ-catenin in these regulatory events remains unclear.
Nuclear staining of β-catenin has been linked with clinicopathological factors in some previous studies.11 In particular, increased nuclear staining of β-catenin has been demonstrated in colorectal carcinoma, being predominantly located at the invasion front.11 This suggests a role for nuclear β-catenin in tumour cell migration and invasion. In addition, the nuclear accumulation of β-catenin was related to unfavourable prognosis in pharyngeal cancer.33 In our study, we found no correlation between nuclear staining and clinicopathological parameters or survival. One explanation for these results might be the relatively low number of cases included in the analysis. However, other studies on carcinomas have found no evidence of nuclear accumulation of β-catenin or have questioned the clinical prognostic value of nuclear staining.1, 11, 34 It seems that the expression of nuclear β-catenin might be tumour type dependent, and studies with a larger number of positive cases are needed to clarify its clinicopathological value.
The loss of expression of catenins has been related to an unfavourable outcome in many human cancers,4, 5, 22 although conflicting data also exist.35 In NSCLC, reduced expression of β-catenin and γ-catenin has been related to poor prognosis,17, 18 which contradicts our data. One explanation for our divergent results could be the relatively high number of recurrences noted in the adenocarcinomas. However, the analyses within the histological subgroups did not change the results.
Taken together, we have shown that the expression of different catenins (α, β, and γ) in NSCLC is related to the histological type and differentiation of the tumour. Furthermore, our study supports the important role of β-catenin and γ-catenin in regulating the proliferative activity of the tumour. However, we found no association between the catenins and the other clinicopathological parameters and survival. We conclude that catenins play an important role in regulating the behaviour of NSCLC, although they have no independent clinical prognostic value beyond the well known factors affecting the survival of patients.
Acknowledgments
This study was supported by EVO funds from the Kuopio University Hospital. Financial support was also received from Savon Syöpärahasto and from the Research Foundation of ORION Corporation, Finland. The technical assistance of Mrs A Parkkinen, Ms R Eskelinen, and Ms H Kemiläinen is gratefully acknowledged.