Article Text

Abstract
Aims: To describe the clinicopathological features of a large number of surgically treated and followed up primary gastric lymphomas and thereby gain a better understanding of their biology, with particular reference to the prognostic factors of high grade tumours.
Methods: A retrospective study of 152 patients.
Results: High grade gastric lymphomas, both pure and with a residual low grade component, differed from low grade mucosa associated lymphoid tissue (MALT)-type lymphomas in that they were more frequently large, ulcerated, at an advanced stage, and highly proliferating. In addition, patients were older and had a worse outcome. The prognosis of high grade lymphomas was influenced by patient age, tumour stage, depth of infiltration in the gastric wall, and the invasion of adjacent organs. Adjuvant postsurgical treatment prolonged survival only in patients with advanced stage and deep neoplastic infiltration.
Conclusions: There is a sharp distinction between low grade MALT-type lymphomas and tumours with a high grade component, justifying their different treatment approach. The postsurgical management of high grade lymphomas should be based on the accurate evaluation of the neoplastic extension.
- stomach
- lymphoma
- mucosa associated lymphoid tissue
- survival
- DLCL, diffuse large cell lymphoma
- LG, low grade marginal zone derived MALT-type lymphoma
- LG + HG, low grade mixed with variable proportions of confluent sheets of blastic cells outside the follicles
- MALT, mucosa associated lymphoid tissue
Statistics from Altmetric.com
- DLCL, diffuse large cell lymphoma
- LG, low grade marginal zone derived MALT-type lymphoma
- LG + HG, low grade mixed with variable proportions of confluent sheets of blastic cells outside the follicles
- MALT, mucosa associated lymphoid tissue
Primary gastric lymphomas represent about 25% of all extranodal lymphomas and 3–5% of all gastric tumours. Most are B cell lymphomas arising from acquired mucosa associated lymphoid tissue (MALT) of the stomach and often remaining localised for a long time.1, 2
Although primary gastric lymphoma has been investigated extensively,3–30 its optimal histological classification, the most accurate staging system, and the exact role of the different therapeutic options are still debated. Surgical resection has been the traditional treatment, alone or in association with chemotherapy and/or radiotherapy. However, the treatment of low grade MALT-type lymphomas has been revolutionised by the recognition of an aetiological link with Helicobacter pylori infection.31 Eradication of the bacterium correlates with morphological regression of the lymphoma in a large proportion of cases.10, 11, 14, 32 Discrepant remission rates (41–100%) reported in the literature mostly depend on the H pylori infection status and tumour characteristics.33 Different treatment, such as chemotherapy/radiotherapy or surgery, is required in patients with low grade disease when deep infiltration in the gastric wall and lymph node involvement are both assessed by endoscopic ultrasonography, and when histology reveals a high grade component. The optimal management of high grade lymphomas remains a matter of debate: the prognostic and therapeutic value of surgery is widely accepted, although conservative strategies, such as chemotherapy and/or radiotherapy have recently been used with success.26, 34
“The treatment of low grade MALT-type lymphomas has been revolutionised by the recognition of an aetiological link with Helicobacter pylori infection”
Our present retrospective study of 152 patients with surgically resected primary gastric lymphomas was undertaken with a view to contributing to the knowledge of this disease. In particular, we analysed the prognostic impact of several clinicopathological parameters in high grade lymphomas, including the effect of adjuvant postoperative treatment.
MATERIAL AND METHODS
All the gastrectomy specimens diagnosed as lymphoma from 1976 to 1996 were retrieved from the archives of the institute of pathology of Ancona University (Italy) and reviewed. Clinical data and information regarding staging procedures, treatment before or after surgery, and follow up were obtained from medical charts and from clinicians. Only primary gastric lymphomas were considered. Cases with advanced tumour stage were included only when gastric involvement constituted the bulk of the disease. Stage was defined according to Musshoff's modification35 of the Ann Arbor staging system.
Formalin fixed and paraffin wax embedded sections from gastric specimens were stained with haematoxylin and eosin and Giemsa. Sections immunostained with antibodies against CD20 (clone L26; Dako, Copenhagen, Denmark), CD3 (polyclonal; Dako), CD5 (clone 4C7; Novocastra, Newcastle, UK), CD10 (clone 56C6; Novocastra), and immunoglobulin light chains (polyclonal; Dako) allowed us to classify each case according to the REAL/WHO system.36 Twenty nine tumours were low grade marginal zone derived MALT-type lymphomas (LG), 70 showed a low grade component mixed with variable proportions of confluent sheets of blastic cells outside the follicles (LG + HG), whereas 53 were classified as pure diffuse large cell lymphomas (DLCL). Three cases of mantle cell lymphoma, three cases of peripheral T cell lymphoma, and one case of Burkitt's-like lymphoma were also observed. Depth of infiltration in the gastric wall, status of surgical margins, extension to lymph nodes, and invasion of other structures and organs were evaluated. Sections from other specimens collected at diagnosis (bone marrow, spleen, and liver), or during follow up (bone marrow, gastric stump, colon, and skin) were also reviewed. Proliferative activity was evaluated on sections immunostained for the Ki67 antigen (clone MIB-1; Dako). It was expressed as percentage of cells with nuclear staining, selecting at low magnification the areas with the highest degree of positivity and counting at least 1000 cells.
Data were coded and entered into an IBM personal computer. Statistical analysis was performed with the SPSS software. The Student's t test and the χ2 test were applied to identify significant differences between two or more groups of data. Survival analysis was performed on the LG + HG and DLCL samples only. Thirteen patients who died from postsurgical complications were excluded, in addition to the cases in which the cause or the date of death were not known. One hundred and nine cases remained available. Survival curves were calculated according to the Kaplan-Meier method, and the log rank test was used to evaluate differences between the curves. All the variables with prognostic value were included in Cox's multiple regression survival analysis to identify the most useful prognostic factors.
RESULTS
Clinical features
None of the patients received neoadjuvant (preoperative) chemotherapy. Four patients were treated with antibiotics to eradicate H pylori before undergoing surgery because of persistence of the tumour. All patients underwent resection of the stomach: there were 90 total and 69 partial gastrectomies. Sixty three patients also received postoperative chemotherapy, two received radiotherapy, and three received both. Chemotherapy protocols were not uniform. They followed the conventional protocol for low grade or high grade lymphoma. Low grade lymphomas were treated with CP (chlorambucil and prednisone) or CVP (cyclophosphamide, vincristine, and prednisone). High grade lymphomas were treated with CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone), MACOP-B (methotrexate, doxorubicin, cyclophosphamide, vincristine, prednisone, and bleomycin), or PROMACE/MOPP (cyclophosphamide, doxorubicin, etoposide, prednisone, vincristine, nitrogen mustard, procarbazine methotrexate, and leucovorin).
Descriptive statistical analysis
Table 1 summarises the clinical and morphological features of each histological type of gastric lymphoma. Because of the small numbers, the cases of mantle cell, T cell, and Burkitt's-like lymphoma were not considered in the following analysis.
Clinical and morphological features of primary gastric lymphomas
Age showed a normal distribution. Patients with LG lymphoma were significantly younger than those with DLCL (Student's t test, p = 0.019).
Postoperative adjuvant treatment was given more often for DLCL than for both LG and LG + HG lymphomas (χ2 test, p = 0.004 and 0.002, respectively).
The location of the tumour in the stomach was not related to the histological type (χ2 test, p = 0.93). Nonetheless, the histological type was related to macroscopic appearance and size: LG lymphomas were more frequently flat and small, whereas LG + HG and DLCL tumours were more frequently ulcerated (χ2 test, p = 0.008) and large (Student's t test, p = 0.03).
Deep infiltration through the gastric wall to the subserosal fat tissue was seen in significantly more DLCL tumours (44 of 70 cases) than both LG + HG and LG lymphomas (χ2 test, p = 0.0005 and 0.0006, respectively). LG tumours were more frequently limited to the mucosa than were the other types.
The three groups were significantly different with regard to pathological stage. Patients with DLCL were very rarely found in stage IE1, and patients with LG + HG and DLCL were more frequently at an advanced stage (χ2 test, p = 0.016).
The proportion of nuclei positive for MIB-1 dramatically increased from LG to LG + HG (Student's t test, p = 0.0001). There was no difference between LG + HG and DLCL (p = 0.36), based on the fact that MIB-1 was counted in selected areas with higher positivity.
After a mean follow up period of 52.2 months (range, 0.3–176), 104 patients were alive; 33 patients died of the tumour and 15 of unrelated causes. The cumulative proportion of survival progressively worsened with increasing histological grade, and the difference between LG and DLCL was significant (Kaplan Meier log rank test, p = 0.017).
During the follow up period, the histological examination of other tissue specimens documented the recurrence of the tumour in six cases. As shown in table 2, two of these patients subsequently died of disease.
Patients with postsurgical recurrence of primary gastric lymphoma
Survival analysis of LG + HG and DLCL
One hundred and nine cases were available for survival analysis. The mean follow up period was 56.4 months, ranging from two to 176 months. Sixty nine patients were alive and 31 had died from the lymphoma. Nine patients, who died from unrelated causes after a follow up period ranging from nine to 119 months, were considered alive in the interval between diagnosis and death.
Figure 1 shows the disease specific overall survival curve. Five year survival was 74.1% and no deaths occurred after 87 months. Table 3 shows the results of the univariate statistical analysis. Patient age (fig 2), tumour stage (fig 3), depth of infiltration (fig 4), and infiltration of adjacent organs (fig 5) all affected outcome in the overall series. These results were confirmed repeating the analysis in the LG + HG and DLCL groups separately, excluding the fact that the age was not important in the LG + HG group and the depth of infiltration did not affect prognosis in patients with DLCL.
Significance level (p value) of the univariate survival analysis (Kaplan-Meier method, log rank test) with the different clinicopathological features used as selecting variable
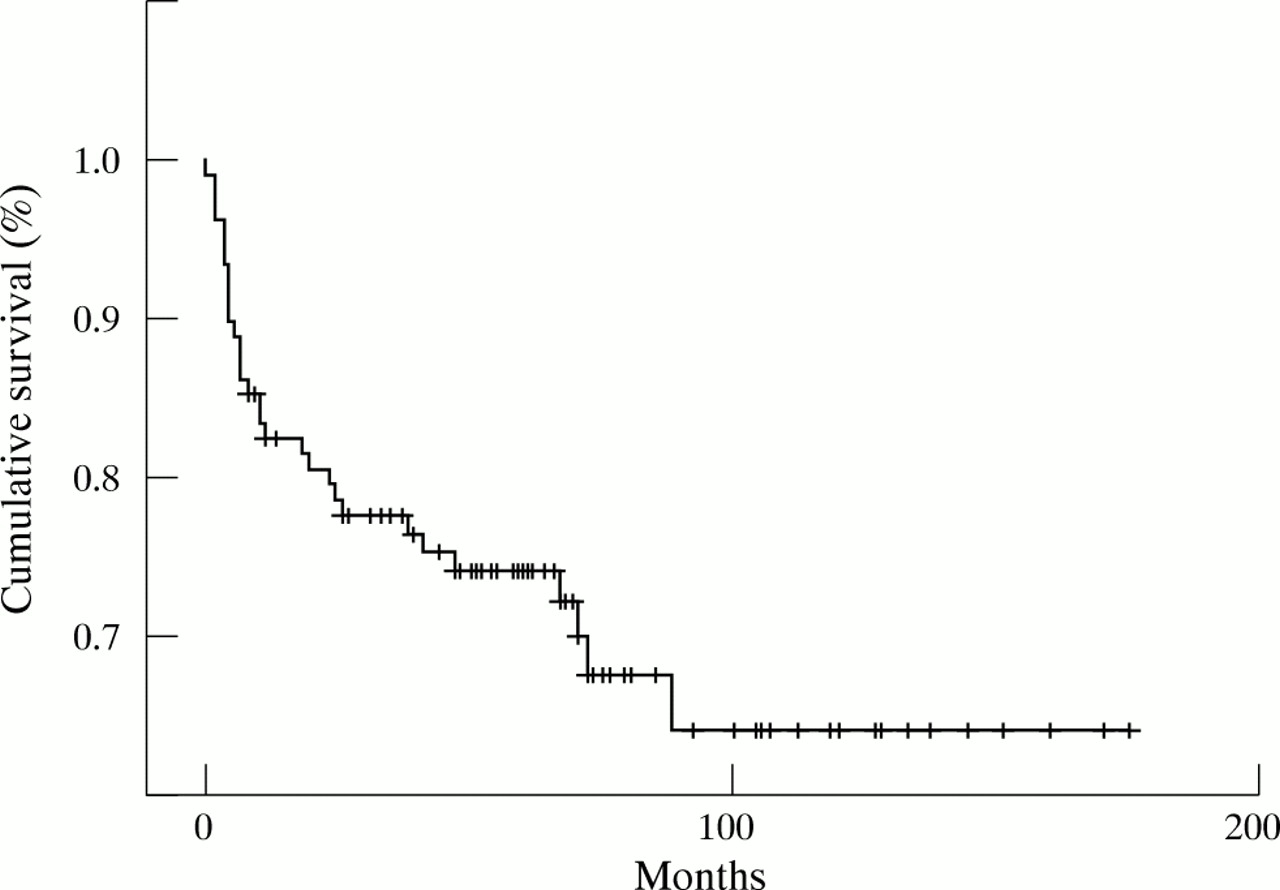
Overall survival curve of patients with LG + HG (low grade mixed with variable proportions of confluent sheets of blastic cells outside the follicles) and DLCL (diffuse large cell lymphoma) lymphomas: 74.1% of patients were alive at five years and 64% at 87 months. The proportion then remained constant.

Kaplan-Meier survival analysis with age as selecting variable (cutoff value, 64 years). The difference between the two curves is significant (log rank test, p = 0.003).

Kaplan-Meier survival analysis with tumour stage as selecting variable. The difference between the curves is significant (log rank test, p = 0.005).

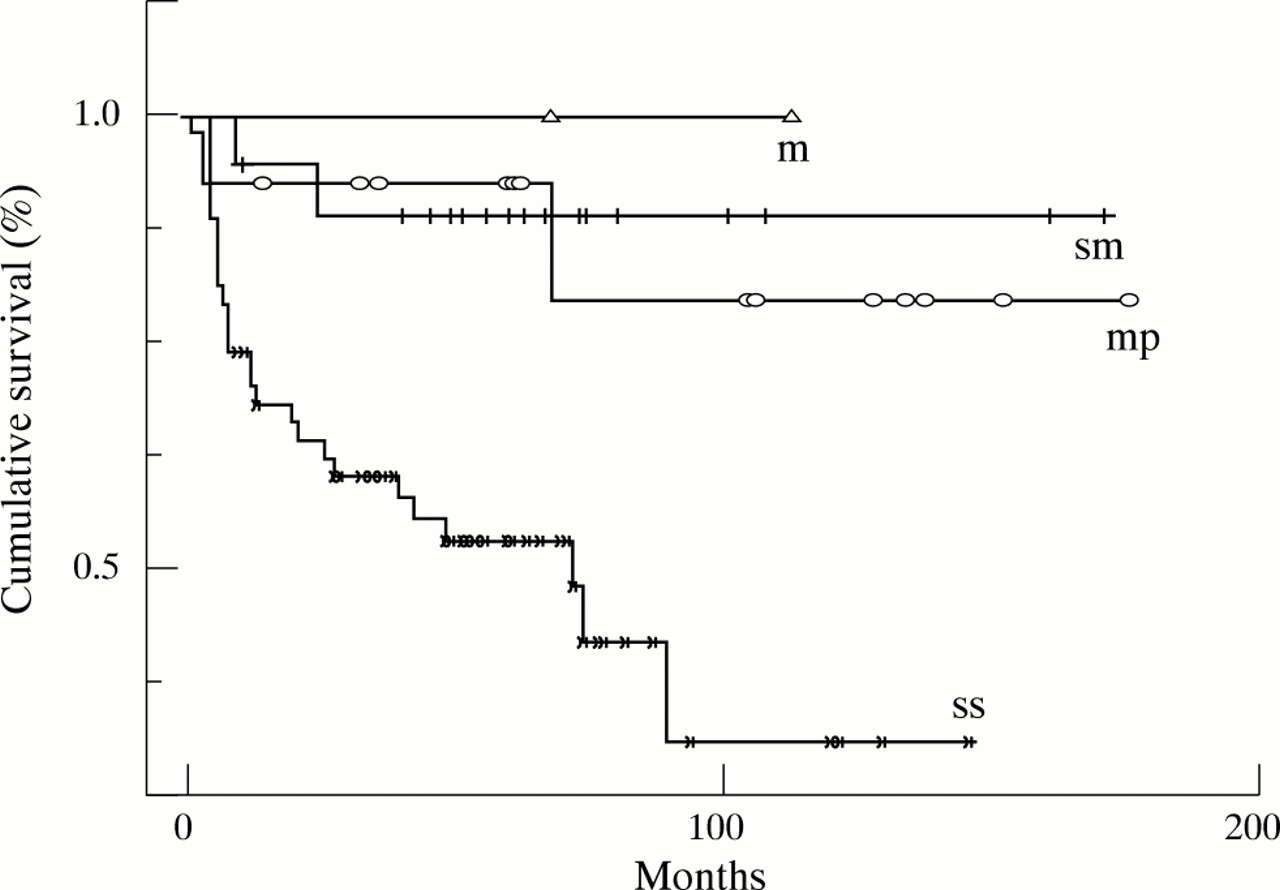
Kaplan-Meier survival analysis with depth of infiltration as selecting variable. The four groups correspond to neoplastic infiltration limited to the mucosa (m), submucosa (sm), muscolaris propria (mp), or extended to the serosa (ss). The difference between the curves is significant (log rank test, p = 0.005).
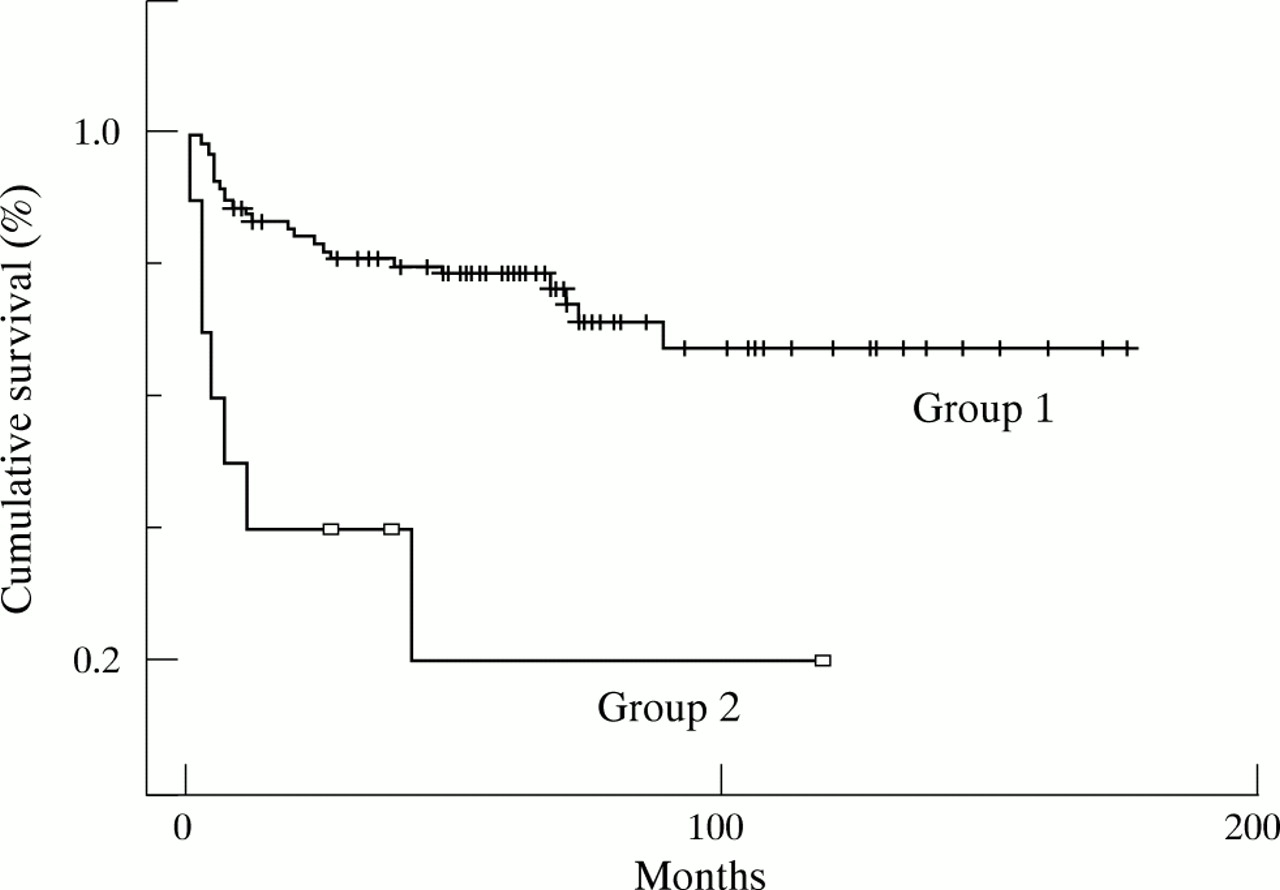
Kaplan-Meier survival analysis of patients without infiltration of adjacent organs (group 1) and with lymphoma invading adjacent organs (group 2). The difference between the curves is highly significant (log rank test, p = 0.0005).
With regard to depth of infiltration, no significant differences in survival were found among lymphomas infiltrating the mucosa, the submucosa, or the muscolaris propria. They were thus placed in a single group and compared with cases showing infiltration of the serosa (fig 6). Comparable results were obtained performing separate survival analysis for both LG + HG and DLCL.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival analysis of patients stratified by level of infiltration in the gastric wall: cases with invasion of mucosal (m), submucosal (sm), and muscularis propria (mp) layers were compared with patients with invasion of the serosa (ss). The difference between the curves is highly significant (log rank test, p = 0.00001).
With reference to tumour stage, patients with stages IIE2, IIIES, and IV showed overlapping survival curves and were grouped together. Moreover, there was no significant difference in survival between stages IE1 and IE2, or between stages IE2 and IIE1; but the corresponding survival curves did not overlap and there was a trend of increasing hazard of mortality going from stage IE1 to IIE1. Therefore, they were not grouped together. The resulting four group classification resulted in a highly significant overall difference in survival (log rank test, p = 0.001) and it was used in the Cox analysis. Repeating the analysis separately for LG + HG and DLCL did not yield reliable results because of the small number of cases in each class.
As already stated, there was no significant difference in survival in patients receiving or not receiving postsurgical adjuvant treatment. However, when the patients were stratified by depth of tumour infiltration, an important finding became apparent: adjuvant treatment had little effect in patients with the lymphoma limited to the gastric wall (log rank test, p = 0.92), but dramatically improved survival when the tumour extended to the subserosal fat tissue (p = 0.00001). Repeating the analysis separately for LG + HG and DLCL yielded similar results in both groups. The importance of postsurgical treatment was also checked in the patients stratified by pathological stage. Treatment was more effective in improving survival in advanced stages (IIE1 and the group IIE2 + IIIES + IVE) than in early stages. However, the significance of the test was affected by the small number of cases in each class and by the fact that no patients in stage IE1 were treated.
The variables that were found to affect prognosis were paired in each possible combination and analysed by the χ2 test to detect a correlation between them. Depth of infiltration correlated with tumour stage (p = 0.0005), with infiltration of adjacent organs (p = 0.0058), and with tumour size (p = 0.05). Tumour size also correlated with tumour stage (p = 0.0056).
Cox multivariate analysis provided a very accurate prediction of survival (χ2 test, p < 0.00001) and selected age and depth of neoplastic infiltration as the most significant parameters.
DISCUSSION
In our study we compared the clinicopathological features of primary gastric lymphomas, which were surgically treated, divided into three groups based on the histological grading.
Patients with LG lymphomas differed from the other two groups, being younger in age, having longer survival, and having tumours that were smaller in size, more frequently flat, with a lower proliferative activity, and at an earlier stage. In contrast, there were only minor differences between LG + HG and DLCL, mainly concerning the infiltration of the serosa, which was more frequent in DLCL. We saw no significant differences in survival between the two groups. These findings suggest a distinction between LG lymphomas, which nowadays are treated conservatively as first choice, and LG + HG or DLCL tumours, which show features of disease progression and require more aggressive treatment.10, 11, 14 Therefore, the recognition of a high grade component in preoperative small biopsies has become crucial for the further management of patients with gastric lymphomas.9, 13 We think that the analysis of proliferative activity can aid the definition of histological grade in small biopsies, where the blastic aspect of the cells can be obscured by artifacts. In our series, MIB-1 immunostaining provided a sharp distinction between LG and the other two groups: values greater than 15–20% were invariably associated with the presence of a high grade component. In contrast, there were no differences in MIB-1 positivity between LG + HG and DLCL tumours because measurements were done in areas with the highest positivity.
In most cases we found that the histopathological features of recurrences were similar to those seen in the primary lymphoma (table 2). In the single case of an LG lymphoma recurring as DLCL after a long time period we cannot exclude the possibility of a second malignancy. Moreover, it should be pointed out that stage I tumours showed local recurrence in the gastric stump, whereas distant relapses were seen in patients with higher stage tumours (II and IV). The histopathological examination of the resection margins failed to show lymphomatous involvement in two of the three patients with gastric stump relapse. This finding suggests that undetectable neoplastic foci may exist at a distance from the main tumour, as recently reported.37
“The recognition of a high grade component in preoperative small biopsies has become crucial for the further management of patients with gastric lymphomas”
In our present study, we excluded all LG cases from the survival analysis, because nowadays H pylori eradication and chemotherapy are the first treatment choice for such cases. In LG + HG and DLCL, which are still treated by surgery, we found that age, stage, depth of infiltration, and invasion of adjacent organs all affected outcome. In agreement with other studies,3, 15, 19, 23, 25, 26 age appeared to be an independent prognostic factor: it was not related to other parameters with prognostic significance, or to differences in the treatment choices that could have been based on patient age. It should be noted that age was found to be most important factor in predicting the outcome of patients with DLCL.
As already claimed by others,4, 5, 7, 8, 12, 17, 18, 20, 22, 23, 25, 26 we believe that stage is of crucial importance for prognostic evaluation. It should be estimated as carefully as possible, including the level of nodal involvement, tumour size, depth of infiltration, and invasion of other organs. All these factors correlated with survival in our present study. The prognosis was unfavourable when regional lymph nodes were involved by lymphoma and it was even worse when the disease extended to more distant lymph nodes and other organs. Depth of infiltration was one of the most important prognostic indicators, particularly in LG + HG lymphomas, which showed a much lower survival rate when the serosa was infiltrated.
Take home messages
-
High grade gastric lymphomas (both pure and with a residual low grade component) were more frequently large, ulcerated, at an advanced stage, and highly proliferating than were low grade lymphomas, and patients were usually older with a worse outcome
-
These differences appear to justify the different treatment approaches used
-
Adjuvant postsurgical treatment prolonged survival only in patients with advanced stage and deep neoplastic infiltration, so that postsurgical management of high grade lymphomas should be based on accurate evaluation of the neoplastic extension
In our study, patients with unfavourable prognostic factors, such as serosal involvement and advanced stage, seemed to benefit from adjuvant postsurgical therapy. This did not occur in the overall series. A similar correlation has been reported in recent papers.6, 16, 19, 24, 26, 28, 30 We believe that these findings should be taken into account in the postsurgical management of primary gastric lymphomas.