Article Text

Abstract
Aims: To evaluate the practicality of use and the effectiveness of a standard protocol for examining nephrectomy specimens for renal cell carcinoma (RCC), with emphasis on the identification of vascular invasion.
Methods: A standard protocol, devised to identify the major prognostic determinants, was used to examine 79 consecutive tumours submitted to four histopathology departments. The incidence of vascular invasion found was compared with the incidence in a historical series of tumours.
Results: The protocol proved easy to follow, and appeared to increase the incidence of observed vascular invasion (40 of 69 cases compared with 69 of 176 cases in the historical series; p = 0.059, Fishers exact test, one sided)
Conclusions: If pathological prognostic determinants are to be used for clinical management, then it is important that they are identified and recorded consistently. The protocol described provides a method of examining nephrectomy specimens that can be used in routine practice and would probably reliably identify recognised prognostic variables.
- renal cell cancer
- pathology
- technical methods
- prognostic indices
- nephrectomy
- IVC, inferior vena cava
- IVCI, inferior vena cava invasion
- MVI, microvascular invasion
- RCC, renal cell carcinoma
- RVI, renal vein invasion
Statistics from Altmetric.com
- IVC, inferior vena cava
- IVCI, inferior vena cava invasion
- MVI, microvascular invasion
- RCC, renal cell carcinoma
- RVI, renal vein invasion
Renal cell carcinoma (RCC) has an incidence of about 5/100 000 and accounts for between 1% and 2% of all cancer related deaths. About two thirds are localised at presentation and these patients will usually undergo nephrectomy. Despite apparent complete tumour excision, 40% will subsequently develop metastases and die from these. Predicting those patients who will relapse is notoriously difficult and relies upon pathological assessment of the surgically resected specimen. There is no generally accepted or validated method of pathological examination of a nephrectomy specimen for renal cell carcinoma. This probably reflects the relative lack of influence that pathological findings have had on subsequent clinical management: until recently the information was used only for prognostication, there being no treatment available to prevent metastasis. This situation may be changing because recent successes with treatment for metastatic disease1 have encouraged a trial of adjuvant treatment (EORTC protocol number 30955) in patients at high risk of subsequent metastasis. Although entry into this trial is by histopathological criteria it is nevertheless recognised that conventional grading and staging has relatively poor predictive value in many cases and there is a need for better ways to assess risk.2
“Predicting those patients who will relapse is notoriously difficult and relies upon pathological assessment of the surgically resected specimen”
Several recent analyses of microvascular invasion—vascular invasion identified histologically in vessels smaller than the main renal veins—as a prognostic indicator3–6 should allow better assessment of the metastatic risk in individual patients. One potential source of inaccuracy is that the identification of microvascular invasion may be dependent on histological sampling because Bonsib and colleagues7 have shown that complete histological examination of the tumour–renal sinus interface appears to increase the yield of microvascular invasion. The renal sinus is the fatty connective tissue that surrounds the pelvicaleceal system within the kidney; it is in this structure that all the veins draining the parenchyma are gathered together into the renal vein. It is therefore a reasonable prediction that early vascular invasion should be found at the junction between the tumour and the renal sinus. However, there are no clear recommendations on how full histological examination of this junction can be achieved. We have devised a simple protocol for the dissection of nephrectomy specimens that allows complete examination of the tumour–renal sinus interface, in addition to ensuring that all other prognostic variables can be assessed. Here, we report our experience of this method in 79 consecutive cases of renal cell carcinoma.
MATERIALS AND METHODS
The protocol was based on the objectives of the examination of a nephrectomy specimen for tumour; namely, the accurate recording of the accepted prognostic determinants. These are: tumour size, type, and grade, tumour invasion outside the kidney, and vascular invasion.2,6
The method (fig 1; appendix 1) is based on that of Eble,8 and is similar to that described by Govender9 for nephroblastoma. However, it differs from Eble’s method because the perinephric fat is not disturbed before the kidney is sliced, so that the relation between the invading outer margin of the tumour and the normal surrounding tissues is preserved. Our protocol also insists that the renal sinus–tumour interface is sampled in a standard way for histology because this is the site at which vascular invasion is most likely to be detected. The description of the protocol has gone through three revisions after being used in four histology departments to ensure that the instructions are clear and unambiguous. It has been used in these departments to examine a total of 79 consecutive nephrectomies from patients with clinically localised renal cell carcinoma. None of the patients had evidence of lymph node or distant metastasis at the time of surgery, although lymph node dissection or formal lymph node sampling were not usually carried out. In each case, the following data items were recorded: maximum tumour diameter, tumour type according to the Heidelberg classification,10 Furhman nuclear grade,11 and whether or not there was invasion of perinephric fat. Vascular invasion was identified by conventional histological criteria (that is, the presence of tumour within an identifiable vascular space) and was classified according to the level reached6 into three groups: inferior vena cava (IVC) invasion (IVCI), renal vein invasion (RVI), and vascular invasion seen histologically in smaller vessels, designated as microvascular invasion (MVI).

{kind=link}
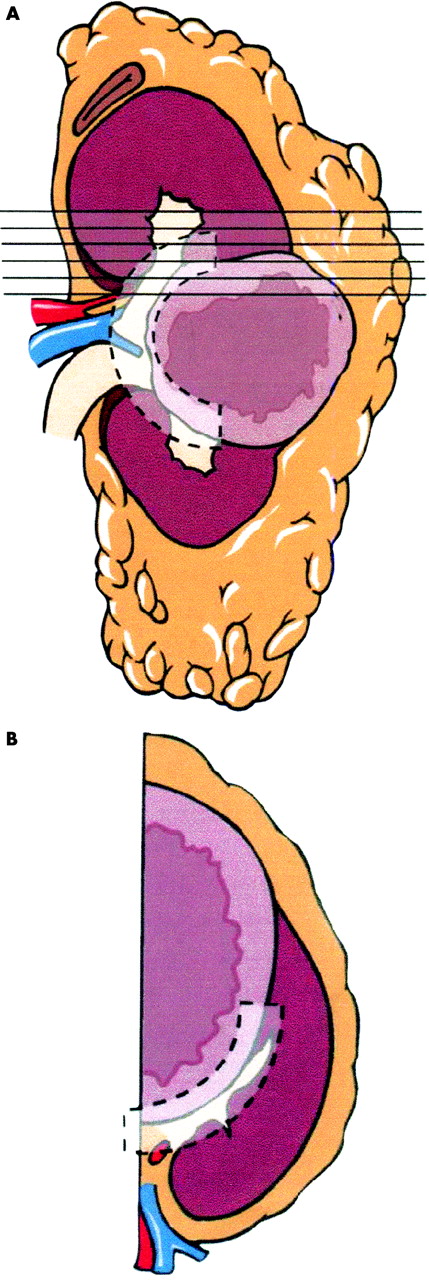
(A) Sagittal cut surface of specimen: the opaque overlay indicates the site of the tumour–renal sinus interface. The lines indicate the orientation of the slices to be taken. (B) An individual slice including tumour; the opaque overlay indicates the tumour–renal sinus interface. This may be present in multiple slices and should be systematically sampled.
PROTOCOL FOR DISSECTION
-
Cut sagitally and divide into anterior and posterior halves, disturbing the perinephritic fat as little as possible. Measure the maximum diameter of the tumour, photograph if required, and then fix.
-
Orientate the specimen: look for and dissect off any perirenal and perihilar lymph nodes (these are rare).
-
Identify the ureter, renal vein, and artery—take and embed transverse sections of each at the resection margin.
-
Cut each half into 4 mm slices in the horizontal plane without removing the perinephritic fat. Separate and lay out the slices so that the relation between the tumour and both the renal sinus and the perinephritic fat can clearly be seen.
-
Assess margins at capsule and renal sinus. For upper pole tumours note the relation with the adrenal.
-
Blocks to take—ensure that there is a block key (fig 1).
-
Lymph nodes, if any (see 2 above).
-
Ureter, vein, and artery (see 3 above).
-
Tumour: external margin. Capsular/peripheral margin, two to three blocks at the site of greatest extension in the perinephritic fat.
-
Tumour: sinus margin. Embed the whole junction of the tumour and the renal sinus, including tumour margins within 2 mm of the sinus (fig 1B).
-
Tumour: other areas. Take blocks of any macroscopically distinctive areas not sampled in (c) or (d) to ensure that foci of sarcomatoid tumour are not missed.
-
Total tumour sampling—at least one block/cm of tumour maximum diameter, the total including (c), (d), and (e) above.
-
Take a block of the adrenal.
-
Background kidney—one or two blocks.
-
Other points of interest—for example, unusual scars/second tumours.
To determine whether this protocol was effective at improving the overall identification of vascular invasion the findings were compared with those of a historical series of 176 consecutive nephrectomies with clinically localised RCC that were resected in two hospitals between 1991 and 1996. An analysis of the findings in this retrospective series has been reported previously.6 Nephrectomy specimens in these cases had originally been dissected using a variety of protocols and the histological slides recently re-examined for the same data items. We also carried out a literature search for series of RCCs in which the incidence of vascular invasion had been investigated. Six papers were identified: the incidence of vascular invasion reported in these series was extracted in a comparable format and compared with the present series.
RESULTS
Seventy nine tumours were examined using the new protocol. Although in most cases the protocol was easy to follow, there were a few circumstances that presented some difficulty. Large or centrally sited tumours may appear to obliterate the renal sinus. In these cases, we found that it was essential to lay out the slices so that they could be examined in good light. After smeared blood had been rinsed off with running water, careful examination usually revealed some residual renal sinus. This could be identified by flecks of fat and prominent blood vessels at the edge of the tumour or compressed between the tumour and the adjacent parenchyma. Some tumours had an extensive tumour–renal sinus interface that would have taken up to 30 or 40 blocks to embed completely. Many of these cases had vascular invasion and it was found that a policy of taking 10 blocks in the first instance, with subsequent additional blocks if vascular invasion was not identified, would probably reduce the overall number of blocks taken without compromising the sensitivity of the method. This was devised as a rule of thumb; the optimum number of blocks required at initial cut up has yet to be determined. In this series, a mean of 12.4 tissue blocks of tumour were taken for each case compared with a mean of 5.6 in the historical series.
Of the seventy nine tumours examined, the mean size was 7.2 cm; 58 were of conventional type, 12 papillary carcinomas, two chromophobe carcinomas, one collecting duct, and six of uncertain histological type. Table 1 shows a cross tabulation of grade, vascular invasion, and size.
Cross tabulation of vascular invasion, size, and grade
Using the new protocol, we identified 40 cases with some form of vascular invasion. In seven, the vascular invasion extended into the IVC and in five tumour was present in the block taken near the cut end of the renal vein. In an additional 28 cases, vascular invasion was found in smaller blood vessels—designated as microvascular invasion—usually in the renal sinus. Vascular invasion in the IVC and the renal vein were easy to identify; microvascular invasion was usually seen in the renal sinus, sometimes in relatively large vessels with a partial muscular wall, and in others it was seen in smaller vessels that did not have a muscular wall. The extreme vascularity of many renal cell carcinomas made it impractical to identify vascular invasion within the boundaries of the tumour mass with any degree of confidence.
Take home messages
-
Recently, there has been some success in the treatment of metastatic disease following nephrectomy for renal cell carcinoma, so better ways to assess the risk of developing metastatic disease are needed
-
We have developed a method of examining the nephrectomy specimen that can be used in routine practice and would probably reliably identify recognised prognostic variables
-
This technique appeared to increase the yield of histologically confirmed vascular invasion, although whether this will improve the selection of high risk cases remains to be determined
In the historical series of 179 cases IVCI, RVI, and MVI were identified in 24, 31, and 14 cases, respectively. Table 2 compares the overall incidence of vascular invasion in the current 79 cases with our historical series, and shows an increased yield of vascular invasion, although the difference does not quite reach significance (p = 0.056; Fishers exact test, one sided). Table 2 also shows data extracted from other published series in which the incidence of vascular invasion has been investigated. These are not strictly comparable with our series because case selection and the data items collected differ. However, the comparison does show that our protocol appears to increase the overall yield of vascular invasion.
Our results compared with other published series that have examined the incidence of vascular invasion
DISCUSSION
We have described a standard protocol for histological examination of nephrectomy specimens with RCC and shown in a consecutive series of cases that it increases the yield of vascular invasion when compared with historical series of our own and with published series. This is hardly surprising because our method concentrates much effort into thorough sampling of the renal sinus, the site of vascular drainage from the renal parenchyma.
We also noted previously that vascular invasion,6 if present, was usually only found in a limited number of blocks; thus, although complete sampling of the tumour sinus interface would be expected to identify any vascular invasion that was present, less thorough sampling would frequently miss such vascular invasion
We have found that the method is easy to use and explain—it has been successfully taught to trainees and to other pathologists. It is presented in an algorithmic form: individuals who follow the protocol should get similar results. This is in contrast to other previously published methods in which much of the dissection and sampling is left to the discretion of the pathologist. When the results of a histological examination are to be used to guide treatment it is important that the results do not depend on variation in operator technique.
“The method is easy to use and explain—it has been successfully taught to trainees and to other pathologists”
The method has been found to be adaptable and has been used successfully on kidneys resected for transitional cell carcinomas; the blocks taken give good orientation of the interfaces of the tumour, the renal pelvis, and the renal parenchyma, facilitating the assessment of staging.
In summary, the protocol described provides a practical and relatively simple method of examining the tumour–renal sinus interface. It appears to increase the yield of histologically confirmed vascular invasion, but at a cost of increasing the number of blocks taken. Whether increasing the yield of vascular invasion by the new protocol improves the selection of high risk cases remains to be determined.
Acknowledgments
Thanks to J Sharpe of Media Resources, University of Wales College of Medicine who contributed the artwork.