Article Text

Abstract
Perivascular epithelioid cell tumours (PEComas) other than angiomyolipoma, clear cell “sugar” tumour of the lung, and lymphangioleiomyomatosis are very rare mesenchymal tumours. The uterus seems to be the most prevalent site of involvement, but only 13 cases of uterine PEComa have been described. Three of these cases exhibited local aggressive behaviour and only one showed metastasis. Because of the extremely small number of cases, PEComas are considered tumours of uncertain malignant potential. This report describes a 68 year old woman, who presented with multiple pulmonary lesions seven years after the initial diagnosis of well differentiated endometrial stromal sarcoma. Histological and immunohistochemical analysis of the pulmonary lesions, in addition to re-evaluation of the primary uterine tumour, led to the final diagnosis of metastatic uterine PEComa. The findings indicate that any PEComa might have malignant potential. Spreading of this tumour to other organs might become evident even several years after primary manifestation.
- perivascular epithelioid cell tumours
- myomelanocytic differentiation
- endometrial stromal sarcoma
- metastasis
Statistics from Altmetric.com
- perivascular epithelioid cell tumours
- myomelanocytic differentiation
- endometrial stromal sarcoma
- metastasis
Perivascular epithelioid cell tumours (PEComas) are mesenchymal neoplasms with a distinct perivascular epithelioid cell differentiation.1 The PEComa family comprises angiomyolipoma, clear cell “sugar” tumour of the lung, lymphangioleiomyomatosis, clear cell myomelanocytic tumour of the falciform ligament/ligamentum teres, and unusual clear cell tumours of the pancreas, rectum, serosa, uterus, vulva, thigh, and heart.1 Tumours of this family that cannot be further classified according to their morphological features are simply termed PEComas.2 This particular subgroup is very rare, with only 13 cases having been described to date, and the uterus has been the predominant site.1,2 In a recent study including eight cases with uterine PEComa, all tumours were limited to the uterus.2 However, in three other cases of uterine PEComa, the tumour showed extrauterine infiltrative growth and, in one case, additional metastases in bones and lungs were detected 18 months after the initial diagnosis.3–5 Because of the small number of cases, PEComas are considered to be tumours of uncertain malignant potential until more well documented cases fully define their potential behaviour.2
CASE REPORT
Past medical history and previous histological/immunohistological analysis
Seven years previously the patient had undergone hysterectomy because of abnormal uterine bleeding. At that time, clinical examination revealed a subserosal uterine tumour 4 cm in diameter, and the clinical diagnosis was suggestive for leiomyoma. However, on gross examination, the cut surface of the tumour was grey to red coloured and was composed of gelatinous appearing material. Histological analysis revealed a solid and tongue-like growth pattern of middle sized cells, with distinct cell borders and with clear to eosinophilic granular cytoplasm (fig 1A). There was no major cytological or nuclear pleomorphism and the mitotic rate was low. The tumour showed local infiltration into the adjacent uterine smooth muscle and serosa. Small slot-like blood vessels within the tumour were present and infiltration into lymph vessels was obvious. In the initial immunohistochemical analysis the tumour was reported to be negative for cytokeratins (KL-1), epithelial membrane antigen, and desmin and positive for the progesterone receptor. Based on these histological and immunohistological findings, the initial diagnosis of well differentiated endometrial stromal sarcoma was made. After resection, no signs of local recurrence were recognised.

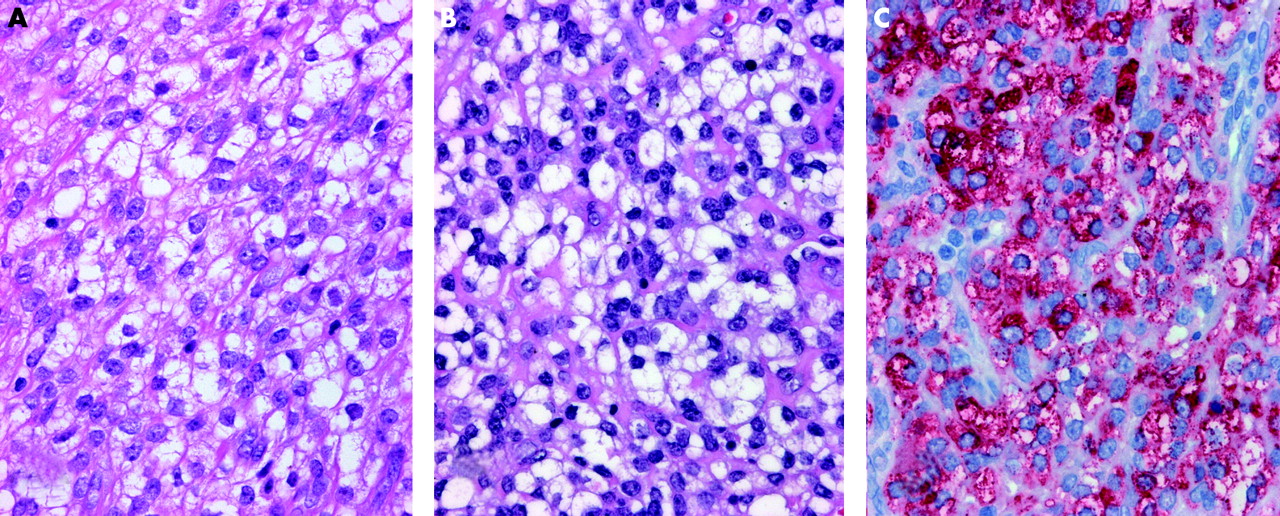
(A) Primary uterine perivascular epithelioid cell tumour and (B) pulmonary metastasis showing clear and eosinophilic tumour cells with only mild cytological and nuclear atypia. (C) Strong reaction (red) of the tumour cells with the melanocytic marker HMB-45. (A,B) Haematoxylin and eosin stain; (C) immunostaining; original magnification, ×40.
Present clinical presentation
In regular tumour follow up investigations, several nodules increasing in size were detected on the patient’s chest x ray seven years after the initial diagnosis (at the age of 68). In subsequent computerised tomography scans of the lungs, the presence of three nodules in the right and of two nodules in the left lung was confirmed (fig 2). To define the nature of the pulmonary lesions, thoracotomy was performed and nine palpable nodules from 0.3 to 2.0 cm were removed by wedge resection on both sides of the lung. Clinically, no further site of tumour recurrence or metastasis was observed.

{kind=link}
{kind=link}
Metastatic perivascular epithelioid cell tumour: computerised tomography scan of the lungs shows distinct round lesions of up to 2 cm in diameter (arrows) in both lungs.
Histology/immunohistochemistry
Gross examination of these specimens revealed grey coloured and sharply demarcated tumours. In summary, histological analysis of the pulmonary lesions exhibited the same morphological features as the uterine lesion (fig 1B). On immunohistochemical analysis, 90% of the tumour cells were positive for the melanocytic marker HMB-45 (fig 1C). Smooth muscle actin, vimentin, and CD10 were also strongly expressed, whereas staining for cytokeratins (KL-1), S100 protein, CD34, and desmin was negative. Only 5% of tumour cells proliferated and stained with the antibody MIB-1. Because no paraffin wax embedded material from the primary lesion was available, we destained some of the old haematoxylin and eosin stained sections of the uterine tumour and performed immunohistochemistry with the HMB-45 antibody, revealing a positive reaction with 20% of the tumour cells. Eventually, our final diagnosis was “multiple pulmonary metastases of uterine PEComa”.
DISCUSSION
PEComas represent a family of myomelanocytic tumours, the best known member of which is angiomyolipoma. The perivascular localised epithelioid cells were postulated as cells of origin. In four of the 13 documented cases with uterine PEComa, aggressive local behaviour with infiltration of ovary, bowel, or vagina and metastasis to pelvic and inguinal lymph nodes was described.3–5 One of these patients developed pulmonary and osseous metastasis after a follow up of 18 months.3 The primary tumour in our report showed only local infiltrative growth into the myometrium and serosa, with no extrauterine extension. At that time (1995), the PEComa concept was not established. Hence, the diagnosis of well differentiated endometrial stromal sarcoma was made.
Take home messages
-
We describe a 68 year old woman, who presented with multiple pulmonary lesions seven years after the initial diagnosis of a well differentiated endometrial stromal sarcoma, which was finally diagnosed as metastatic uterine perivascular epithelioid cell tumour (PEComa)
-
Therefore, uterine PEComas do appear to have malignant potential and all patients with this potentially malignant disease should be carefully followed up
“Any patient with this potentially malignant disease should be carefully followed up”
Applying the classification of Vang and Kempson, the uterine PEComa in our patient belongs to group A because of its large content of clear cells, its tongue like growth pattern, and the strong HMB-45 positivity. However, actin was also strongly expressed, a finding more typical for tumours of subgroup B.2 Because we found a discrepancy in the prevalence of HMB-45 positive tumour cells in the primary tumour versus the metastases, it remains unclear whether the proposed grouping can be maintained. The prognostic relevance of this subclassification also remains to be elucidated.
Although more information on the clinical, phenotypic, and genetic characteristics of uterine PEComas is needed, any patient with this potentially malignant disease should be carefully followed up.