Article Text

Abstract
This article gives guidance for the handling and examination of various types of lung tissue specimens to provide: (1) accurate diagnosis and assessment of severity of disease; (2) sufficient information for the accurate staging of tumours; and (3) an assessment of the contribution of various occupational disorders to the cause of death.J Clin Pathol(J Clin Pathol 2000;53:507–512)
- dissection
- lung
- pleura
Statistics from Altmetric.com
Examination of lung specimens
The lung can react to a wide variety of insults in many different ways: the range of conditions includes congenital, metabolic, infective, vasculitic, occupational, and neoplastic. To a large extent, the handling and examination of lung specimens should be determined by the type of pathological process affecting the lung. This can often be anticipated by close collaboration between the pathologist, radiologist, and the clinicians, the benefits of which cannot be overemphasised.
In this “Best Practice” guideline, the specimen handling and macroscopic examination of closed needle, endobronchial, transbronchial, open thoracoscopic, and resection specimens (segmental, lobectomy, pneumonectomy, and pleuropneumonectomy) are described. Cytological and postmortem examination of the thoracic cavity (excluding the handling of pneumoconiosis and mesothelioma cases) are not dealt with in this document.
Aspects of health and safety in handling lung specimens
The examination of lung specimens entails two particular hazards, namely: (1) infection risk, particularly tuberculosis; and (2) excess ambient formaldehyde concentrations. If there is clinical suspicion of tuberculosis or other infection, tissue should be sent unfixed for culture, and tissue received in fixative in the laboratory should be kept for 72 hours before processing. Such “high risk” tissue should not be submitted for frozen section examination unless absolutely necessary because this puts laboratory staff at risk and contaminates equipment.
Standard methods of lung inflation involve the use of copious quantities of formaldehyde, and unless the procedure is carried out in an appropriately ventilated area, the ambient formaldehyde concentration will rise above the permitted concentration as outlined in the UK government regulations. Appropriate protective clothing, including masks and eye shields, is essential, and lung inflation should ideally be performed in a suitable cabinet with an extraction fan.1
Types of surgical lung specimens
CLOSED NEEDLE OR DRILL BIOPSY SPECIMENS
Transthoracic biopsy is commonly performed to assist the diagnosis of localised thoracopulmonary lesions. The specimens may be of lung parenchyma or of pleura and might be obtained with a fine bore needle, a wider bore cutting needle (Trucut), or by using a high speed air drill (trephine). Their size is determined by the type of instrument used to obtain them. Usually they measure 2 or 3 mm across and vary from 2 to 10 mm in length. Macroscopic examination is usually of little value; the major decision is how to handle them. This depends on the clinical information and the size and number of pieces of tissue submitted. In every case, part of the material should be fixed in formaldehyde and processed routinely. If an infective cause is suspected some of the tissue will be required for microbiological examination. Some of the specimen might need to be deep frozen for histochemical or immunohistochemical procedures—for example, in lymphoproliferative processes. Special fixatives might be required for immunohistochemical or electron microscopical studies.
Contraindications to percutaneous lung biopsy include pulmonary hypertension, bleeding diatheses, bullous emphysema, and arteriovenous malformations.
ENDOBRONCHIAL AND TRANSBRONCHIAL BIOPSY SPECIMENS
The flexible fibreoptic bronchoscope, in addition to supplying material in the form of endobronchial and transbronchial specimens, provides material for culture from brush biopsies and bronchoalveolar lavage fluid. In particular, endobronchial resections are used in the management of “typical” bronchopulmonary carcinoid tumours. In addition to providing tissue for primary diagnosis, transthoracic biopsy and bronchoalveolar lavage fluid are increasingly used in the assessment of activity of a known disease, and in post-transplantation cases in the assessment of infection and rejection.
To obtain adequate material with minimum crush artefact, wide cupped forceps should be used and specimens “expanded” by gentle agitation in a small quantity of saline before fixation. Usually, they measure 2 to 3 mm in each dimension. Examination and handling is similar to that of closed biopsy specimens.
It is good practice routinely to cut multiple sections on these specimens and leave some unstained, so that small lesions such as granulomas are not missed, and also so that spare sections are available for special staining procedures.
OPEN AND THORASCOPIC LUNG BIOPSY SPECIMENS
These biopsies are the method of choice in the elucidation of the nature of diffuse lung disease and have a role in the diagnosis of solitary nodular lesions and in staging before lung transplantation. The size of these depends on whether the tissue is obtained by thoracoscopy, limited thoracotomy, or exploratory thoracotomy and will vary from 2 cm upwards. The pathologist should receive the tissue fresh and examine it macroscopically. The use of a hand lens helps to identify the lesions, which should be noted as solitary or multiple. In addition, their colour, demarcation, size, and, if possible, their relation to anatomical structures, such as airways, should be determined. The pathologist should select tissue for microbiological investigation or special procedures, such as electron microscopy or cytogenetic analyses, if appropriate. It might be useful at this point to carry out a frozen section to decide on adequacy of sampling, likely diagnosis, and what special procedures might be most appropriate. The tissue should always be handled very gently and instruments used should have sharp blades to reduce artefacts. Touch imprints might be useful—for example, with the appropriate special stain, pneumocystis organisms can be diagnosed rapidly. Whatever tissue remains should be carefully inflated with fixative using a small gauge needle.2 This facilitates the assessment of the distribution of lesions, which is extremely important in the diagnosis of non-neoplastic conditions of the lung.
SEGMENTAL, LOBECTOMY, AND PNEUMONECTOMY SPECIMENS
Ideally, these specimens should be inflated whole with formalin using a tube or catheter inserted into the lumen of the bronchial resection margin and connected to a container of fixative at a pressure of 25 to 30 mm of water. With lobectomy and pneumonectomy specimens, it is often necessary to replace the tube or catheter within different segmental bronchi to obtain inflation of all parts of the specimen. A tight seal around the catheter and a relatively intact pleura are necessary for proper inflation. The lung should be inflated until the pleura is smooth and then be left immersed in formaldehyde for 24 hours. It is not necessary to clamp the bronchus. The need for special procedures, however, might mean that the specimen is often partly dissected before fixation, and inflation might be difficult. After fixation, we prefer to make one large sagittal cut perpendicular to the hilum along the whole of the specimen. For tumours, we follow this by further cuts along the bronchi. Some advocate the opening of each major bronchus along its length using scissors or by cuffing down on to a probe already inserted into the lumen.3 In non-neoplastic conditions, we prefer further parallel cuts at 1 to 2 cm intervals. At necropsy, the lungs should be examined in a similar manner.
Macroscopic examination and the selection of tissue blocks (table 1)
Checklist for examination and blocking of surgical and necropsy lung specimens
The procedure applies only to segmental, lobectomy, and pneumonectomy specimens. The type of lung specimen received should be specified and the size and weight of the specimen noted before inflation. The size and weight do not give any valuable clinical information but might sometimes be useful for identification. It is useful to consider the examination and tissue block selection under neoplastic and non-neoplastic headings because the information required from the specimens is different.
Examination of specimens containing neoplasms
STAGING
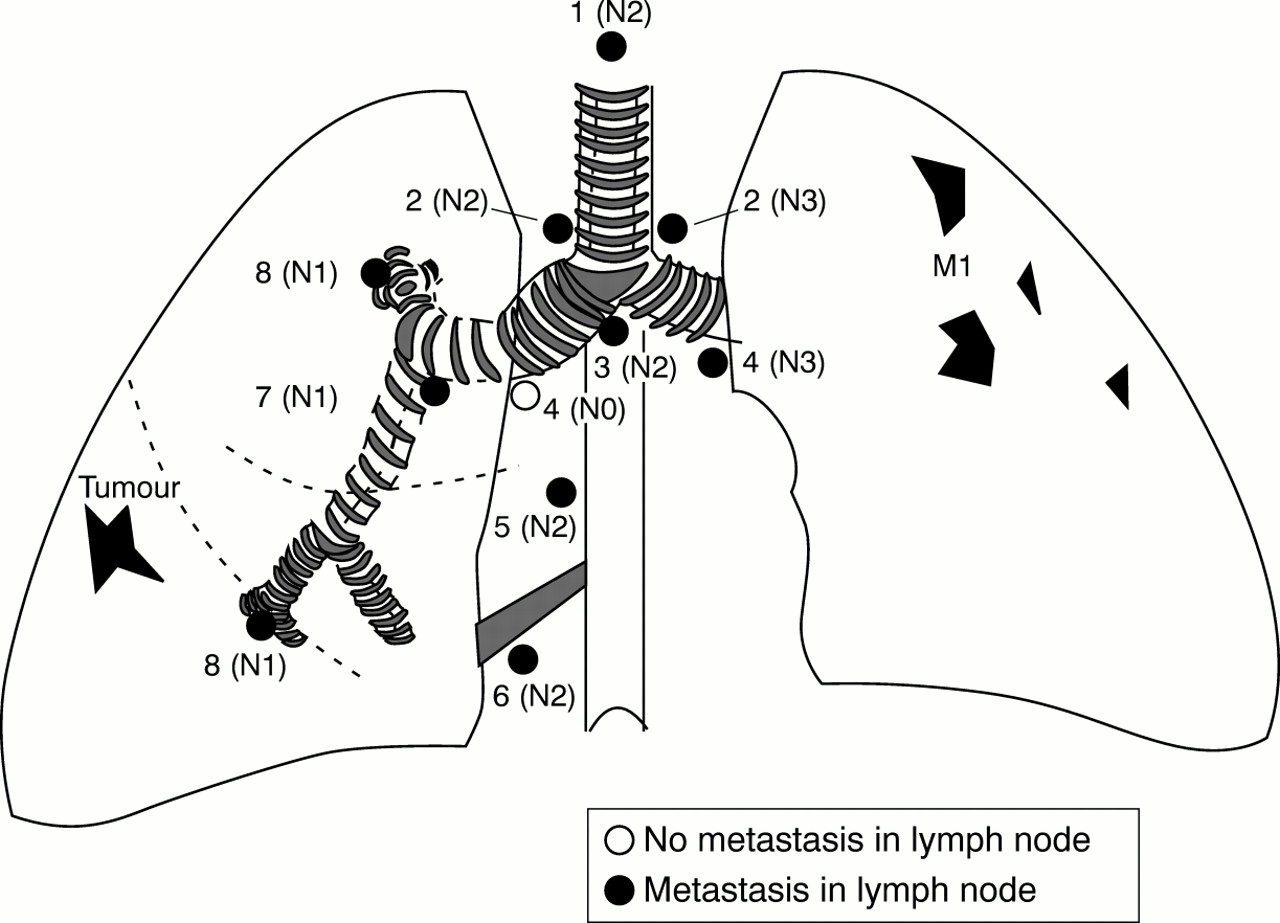
The pathologist has a central role in determining the staging of a lung tumour, and the information required for this largely determines the selection and orientation of tissue blocks. Staging is necessary to determine the prognosis of a given tumour and might modify its treatment. Staging also allows results of different treatment regimens from different centres to be compared. The most widely used staging system for lung tumours is that developed and refined by the American joint committee for cancer staging.4–6 The system is based on the size and location of the primary tumour (T), the lymph node status (N), and the presence of metastases (M), and is often referred to as the TNM system (fig 1; tables 2–4).
TNM staging for lung carcinoma
International staging system for lung cancer: stage groupings of TNM subsets (revised version, Mountain 1996)6
Macroscopic assessment of occupational lung diseases

{kind=link}
Diagrammatic representation of TNM staging for lung carcinoma. The regional lymph nodes are represented by the following numbers: 1, mediastinal; 2, paratracheal; 3, subcarinal; 4, hilar; 5, paraoesophageal; 6, pulmonary ligament; 7, interlobar; 8, segmental.
TUMOUR SIZE
The pathologist is the only person capable of providing an accurate assessment of the size of the tumour because radiological investigations usually overestimate the size of the tumour as a result of surrounding obstructive or inflammatory changes. Depending on the size of the tumour, the pathologist should take a minimum of two (but preferably more) blocks to determine the histological type.
TUMOUR DIFFERENTIATION
The classification of lung tumours depends on the presence of specific differentiation—for example, glandular or squamous; the more tissue examined, the greater the likelihood of showing differentiation. Large cell undifferentiated carcinoma can only be diagnosed in the absence of any type of differentiation. Pleomorphic carcinoma comprises spindle and/or giant cell carcinoma with any other differentiation pattern. Heterogeneity is not uncommon in lung tumours and more than one type of differentiation might be seen. Ancillary studies can be used to assist with definitive diagnosis. Mucin histochemistry (alcian blue (pH 2.5) and diastase periodic acid Schiff) is routinely advocated. Immunohistochemistry might be particularly helpful in the diagnosis of neuroendocrine neoplasms. This requires two or more markers: chromogranin A, synaptophysin, and leu-7 are preferred in our laboratory. Immunohistochemistry is also particularly useful in the diagnosis of pulmonary sarcomas, lymphomas, and mesothelial neoplasms.
TUMOUR SITE
If the tumour is situated in a major bronchus, at least one block should be taken perpendicular to the bronchial wall to assess the depth of invasion. Although not required for staging, the colour, shape, consistency, and presence of cavitation should be noted. The bronchial mucosa should also be carefully inspected for roughness or loss of the normal bronchial ridges and blocks taken; this may show in situ malignancy,7 which is important clinically if it extends close to the proximal bronchial resection edge. For central tumours, the bronchus they arise from should be specified, whereas for peripheral tumours, the segment they arise from should be noted. For polypoid tumours, the point of attachment of the stalk to the bronchus indicates the origin. The distance of central tumours from the proximal bronchial resection edge should be measured. A transverse block of the proximal bronchial resection edge should be taken to check for the presence of tumour. The distance of the tumour from the pleura should be measured, and if the tumour extends near to the pleura, a block should be taken to include both the pleura and part of the tumour. The presence of a pleural effusion should have been noted by the surgeon at thoracotomy.
Additional blocks should be taken of the background lung to include abnormal and normal looking lung. Any abnormality of the pleura should also be blocked.
Any lymph nodes in the resection specimen such as hilar, lobar, interlobar, or segmental (all N1) should be separately identified and blocked. Usually, the surgeon will submit separately identified N2 (ipsilateral mediastinal and subcarinal lymph nodes) and N3 (contralateral mediastinal and hilar lymph nodes, and ipsilateral or contralateral scalene, or supraclavicular lymph nodes), and the pathologist should examine them separately for neoplastic disease.
If a second tumour is present in the specimen it should be staged as M1 disease.
Examination of specimens containing non-neoplastic lesions
The purpose of examining these specimens, whether necropsy or surgical, is to render a diagnosis or assess the severity of the disease, or both, severity of disease being particularly important in occupational disorders. The pleura should first be examined for colour, thickness, exudate, or focal lesions such as pleural plaques. The hilar nodes can also be examined at this point and the size, colour, shape, consistency, and distribution of such lesions should be recorded. Further sagittal slices of the specimen are then taken at 1 to 2 cm intervals. Tissue blocks should be taken of abnormal and normal looking lung: in some diseases the diagnostic lesions are present in the less severely affected parts of the lung.
Occupational lung disorders
The following method is a useful way of recording dust lesions, emphysema, and interstitial fibrosis and can be applied to ordinary lung slices or Gough-Wentworth whole lung sections (appendix 1), providing there has been good inflation (table 4).8,9 It is good practice to keep intact one well inflated whole lung slice for this examination, and to take blocks from the other slices. The pneumoconiosis committee of the American College of Pathologists and the National Institute for Occupational Safety and Health have recommended that 15 tissue blocks should be taken from the lungs of patients with disease suspected to have been induced by asbestos.10 This is impractical for many non-specialist laboratories. As a minimum we recommend that four routine blocks should be taken, namely: (1) apex of upper lobe; (2) apex of lower lobe; (3) basal segments; and (4) major bronchus to include nodes. Other blocks should be taken from macroscopically visible lesions. Some of the blocks should include pleura.
DUST LESIONS
In general, non-fibrous dusts with a low free silica content—for example, coal, kaolin, and mica, have low fibrogenicity and produce widely distributed focal, impalpable stellate lesions situated at the centres of the lobules (primary foci). These usually measure up to 5 mm in diameter. The extent of these foci can be conveniently recorded by giving the average size of the primary dust lesions on a 0 to 3 scale and the percentage of lobules affected on a 0 to 3 scale (table 4).
Non-fibrous dusts with a considerable free silica content produce stellate (in mixed dust pneumoconiosis) or rounded firm, palpable nodules owing to a high collagen content, as in classic silicosis. These can be referred to as secondary dust lesions. In some cases of coal worker's pneumoconiosis, these secondary lesions might be present but are usually few in number. The number can be recorded for a range of sizes (table 4).
The definition of progressive massive fibrosis lesions is arbitrary, varies according to different authorities, and depends on size. Many authorities require a lesion of at least 2 cm in diameter but the International Labour Organisation's (ILO) radiological classification only required 1 cm. These days, we regard all dust lesions greater than 1 cm as progressive massive fibrosis, apart from rheumatoid pneumoconiotic (Caplan) lesions. The number, size, consistency, colour, and presence of cavitation should be recorded for these lesions. It should also be noted whether they look homogeneous, as in the typical coal dust progressive massive fibrosis, or seem to be formed by conglomeration or individual smaller lesions, as in silicosis.
INTERSTITIAL FIBROSIS
This might be recognised if it is severe and the distribution noted, but mild to moderate degrees are often not recognised macroscopically. The pattern and degree of pulmonary fibrosis can be enhanced by the barium sulphate impregnation technique. Barium sulphate precipitates very finely on all structures and does not become easily detached.9 This technique is also useful for showing emphysema. It is simple and inexpensive and can be performed in most laboratories. The method is given in appendix 2.
The final estimate of severity of pulmonary fibrosis is best done by grading of histological sections taken in a systematic manner, similar to that used for asbestosis,10 and the selection of tissue blocks suggested above should fulfil these requirements.
EMPHYSEMA
Several different systems have been developed for quantifying emphysema macroscopically.11 The method we use is quick and convenient and is as accurate as point counting.12 It can be used for lungs with or without pneumoconiotic lesions. The type of emphysema (panacinar, centriacinar, etc) is recorded. The average severity in affected lobules is graded on a 0 to 3 scale, as is the proportion of lobules affected, similar to assessment of dust lesions (table 4).
HANDLING OF A CASE OF SUSPECTED MALIGNANT MESOTHELIOMA AT NECROPSY
Mesotheliomas have become more common over the past 10 years and most histopatholo-gists will encounter a case from time to time; therefore, it is important that they should know how to handle such cases.13
In putative mesothelioma cases the necropsy aims to ascertain the following: (1) tumour diagnosis; (2) tumour aetiology; and (3) the extent and severity of any other disease present at necropsy that would have affected life expectancy or quality because this will be taken into account in assessing compensation, if the tumour is deemed to be asbestos related.
A careful description of the appearance and extent of the tumour is essential, with particular reference to invasion of adjacent structures, such as lung parenchyma, chest wall, mediastinum, pericardium, and lymph node or other distant metastases. These factors play an important part in mesothelioma staging (table 5).14,15 The staging system as outlined by Butchart and colleagues14 has been used generally, and is easy to apply. Recently, Rusch15 has modified this system to incorporate the TNM system, as shown in table 5.
Staging of diffuse pleural malignant mesothelioma
The background lung tissue and pleura should be assessed for neoplasia and fibrosis. A background knowledge of the occupational history is beneficial and, if possible, should go back to the commencement of work because of the long latency period of asbestos associated disease. It is also necessary, particularly in cases where direct occupational exposure to asbestos is not readily apparent (for example, in women), to know the occupations of other members of the household because occasionally asbestos related mesothelioma can be acquired from the contaminated work clothes of other members—so called paraoccupational mesothelioma.
Ideally, both lungs should be retained for future examination. Multiple samples should be taken of the tumour and processed for light microscopic examination. Adjunct histochemical and immunohistochemical procedures might be necessary to ascertain the diagnosis of mesothelioma.13
For the assessment of asbestos bodies it is important to take non-tumorous samples from each lobe of the lung. Perls staining in thick (30 μm) sections facilitates asbestos body identification. In the event that no asbestos bodies can be identified by light microscopy, consideration should be given to electron microscopic mineral analysis of digested lung tissues. This procedure allows both the quantity and quality of asbestos fibres to be determined accurately.16 This will entail referral to a specialist laboratory with experience in these techniques, which can compare the values with reference ranges. The results obtained should be considered in relation to the details of the occupational history, and particularly the latency, before concluding that the tumour was caused by exposure to asbestos.