Article Text

Abstract
Aims To review the incidence of multiple tumour marker (TM) requesting in the primary care setting and determine whether the rationale for requesting a TM panel is in agreement with evidence-based guidelines.
Methods Data-mining software was used to retrospectively identify multiple TM requests and requesting practices of GP surgeries over a 34-month period for α-fetoprotein, CA125, CA15-3, CA19-9, carcinoembryonic antigen and prostate-specific antigen. The appropriateness of each test was reviewed by a clinical biochemist in accordance with National Association of Clinical Biochemistry best-practice guidelines.
Results 505 multiple TM requests were identified which corresponded to 1304 TM tests. Comparison with best-practice guidelines suggested that 68% of request cards contained no appropriate TM request, and 84% of the tests requested were inappropriate.
Conclusion A review of requesting practices in primary care for TMs highlights the need for laboratories to be more proactive in educating their users on their clinical utility and limitations.
- Tumour marker
- education
Statistics from Altmetric.com
Introduction
Inappropriate testing is an ongoing problem in the clinical biochemistry laboratory. Most notably the Carter Report (phase 2) highlighted that inappropriate requesting of tests is endemic with a reported incidence of 25–40%.1 2 With year-on-year increases in workload of 8–10%, there is an increasing need to manage the demand of these tests.3
There has been much debate on tumour marker (TM) requesting in both primary and secondary care. When used in the appropriate clinical context, TMs can be a useful aid for the clinician in the diagnosis, prognosis and management of patients with cancer. In the majority of cases, their low diagnostic sensitivity and specificity limit their use as a first-line rule in/rule out test for cancer and are only indicated in patients known to have cancer.
In order to resolve some of the common misconceptions surrounding the use of TMs, Sturgeon reviewed their clinical utility using the National Association of Clinical Biochemistry (NACB) guidelines on use of TMs.4 This review highlighted the fact that in most situations, requesting of multiple TMs offered no clinical benefit for the patient and could be highly misleading in patients with non-specific symptoms.4 5 The pitfalls of this practice were emphasised in an accompanying case report, which showed the association of TMs with non-malignant pathology.6
In light of this publication, the Department of Clinical Biochemistry at University Hospital Lewisham reviewed the requesting patterns of TMs in primary care and particularly the incidence of multiple TM requests to determine whether the rationale for requesting a TM panel was in accordance with best-practice guidelines.
Methods
Using data-mining software (Telepath 2000, iSOFT) multiple TMs requested on a single request card for individual patients were identified from GP surgeries within a 34 month period from 1 January 2007 to 31 October 2009. Owing to the volume of requests received, it was not feasible to review retrospectively all single TM tests. Data on α-fetoprotein, cancer antigen 125 (CA125), CA15-3, CA19-9, carcinoembryonic antigen (CEA) and prostate-specific antigen (PSA) were identified, and the patients' hospital number, sex, date of birth and test result recorded. The requesting location was also noted to determine whether there was any disparity in requesting practices between individual surgeries. Furthermore, as each test result was electronically linked to the original request form, the clinical details stated by the requesting doctor were also recorded. Data were handled in keeping with the Caldicott principles, and this study was registered with the hospital audit office.
Each identified request was reviewed retrospectively by a clinical biochemist and chemical pathologist within the department. Disagreements were resolved through discussion. For instance, PSA testing has been widely adopted by many clinicians as a result of the NHS introducing the informed choice Prostate Cancer Risk Management programme as a first-line investigation in males suspected of prostate cancer. As a result, in this study it was agreed that all PSA requests in male patients were assumed to be appropriate unless clinical details stated otherwise.7 For request cards that contained no clinical details, previous records were reviewed, and if no evidence was identified to justify their measurement, these tests were deemed inappropriate.
With the exception of PSA, the justification for performing each test was reviewed against guidelines from the NACB (table 1), and based on these recommendations the test was defined as either appropriate or inappropriate.5
Current National Association of Clinical Biochemistry recommendations for the appropriate use of tumour markers
Results
A total of 17 879 separate GP requests were received for TMs and consisted of 18 678 tests (table 2). During the 34-month period, requests for TMs increased on average by 3.1% per month (figure 1). Ninety-one per cent of all requests received were for a single PSA measurement. Five hundred and five request cards were identified as containing multiple requests with two or more TM tests and accounted for 2.8% of the total number requests received.
Summary of tumour marker requests received by GPs

Number of tumour marker (TM) tests analysed per month from January 2007 to October 2009.
Requests for multiple TMs comprised a total of 1304 separate tests. Less than 1% of request cards contained no clinical details. The justification for performing the test when compared against recommendations from NACB suggested that 84% of these tests seemed to be inappropriate (table 3). Review of individual request cards that contained a TM panel suggested that 68% of these request cards had no appropriate TM request (figure 2). Of these requests, over half (57%) were for two TMs, while 14% of these requests contained four or more different TMs. The most common reason for requesting a multiple TM panel according to the clinical details stated on the request card was for screening patients with non-specific symptoms such as weight loss, being tired all the time and abdominal pain.
Number of appropriate and inappropriate tests suggested by National Association of Clinical Biochemistry best-practice guidelines that were requested as part of a tumour marker panel

Overview of multiple tumour marker requesting by GPs within a 34-month period compared with National Association of Clinical Biochemistry best-practice guidelines.
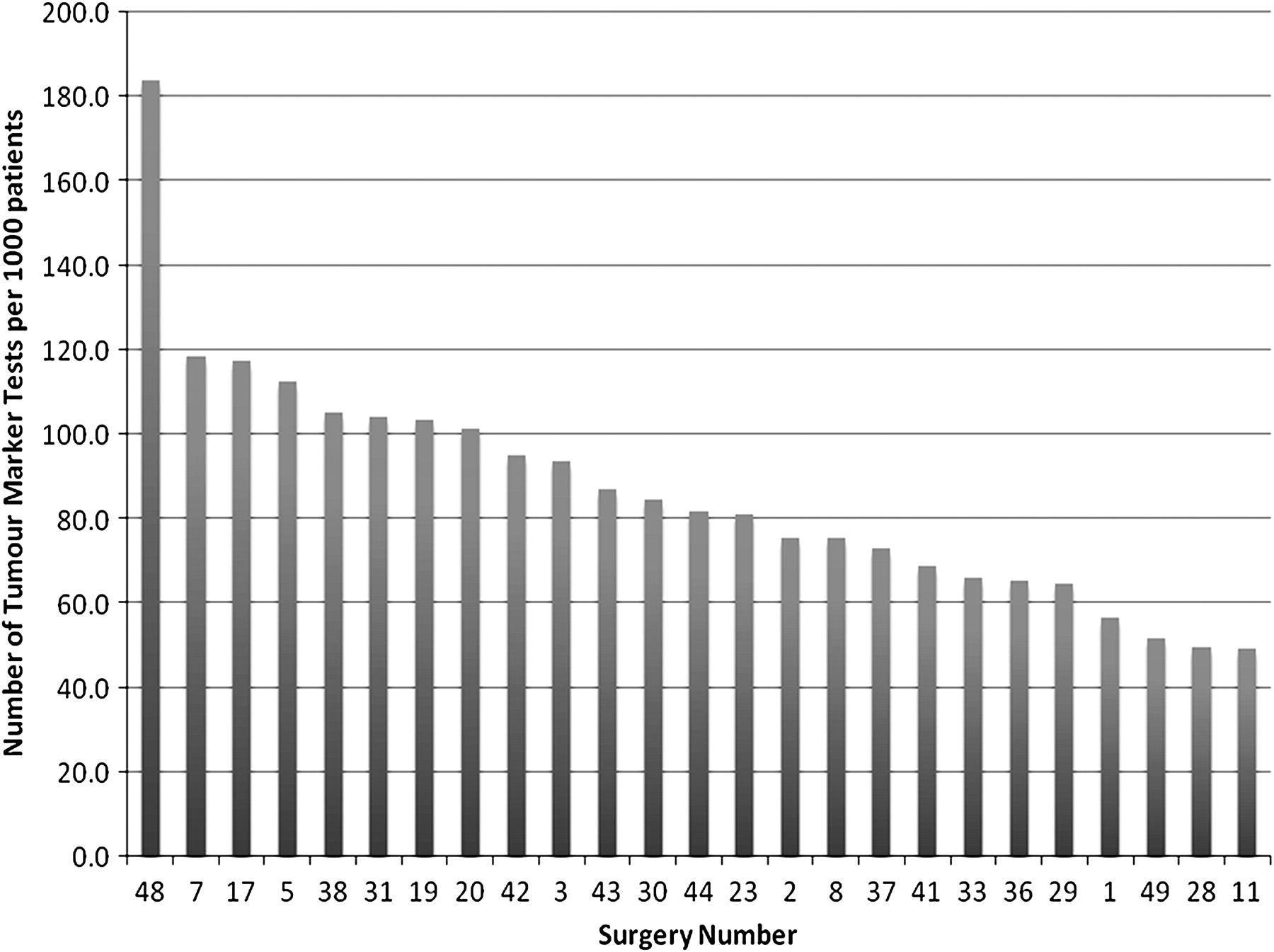
A review of the number of tests requested per surgery and accounting for the number of registered patients showed that the number of TM tests requested ranged from 49 to 184 tests per 1000 patients with a median of 82 tests per 1000 patients per surgery (figure 3).

{kind=link}
{kind=link}
{kind=link}
Number of tumour marker tests analysed per 1000 registered patients for the top 25 requesting surgeries.
Conclusion
When used in the correct clinical context TMs can be of significant value to the treatment and management of a patient with cancer. However, their indiscriminate use in asymptomatic individuals is not recommended and may lead to further unnecessary and costly investigations. With month-on-month rises in TM requests, the finding in this study that 84% of multiple TM requests seemed to be inappropriate highlights the need of laboratory professionals to educate its primary care users on the utility and pitfalls of these specialist investigations.
Traditionally, laboratories acted as gatekeepers to performing TM requests by vetting every individual request received. Although this can reduce the volume of work, the cost of vetting each request is far greater than the cost saving achieved and does not endear us to our colleagues in primary care. Alternatively tailoring request cards has been of some success, with a reported 25% reduction in tests received.8 With the developments seen in information technology, the resources are now available to allow labs to be more proactive in managing tests that are received, and some recent publications have reviewed this topic extensively.3 9 By using rule-based criteria, order communications systems and, in some instances, limiting the testing repertoire to senior clinicians, this intelligent software has allowed laboratories to intervene at the point of test request, thereby directly reducing the number of inappropriate requests received.
In spite of publications highlighting the role of TMs in clinical practice, inappropriate requesting of TMs is still encountered, as this study shows. An audit reviewing TM requests in Northern Ireland reported that despite publication of local TM guidelines, clinicians still chose to use certain TMs inappropriately for screening asymptomatic individuals.10 Similarly, a survey of 28 laboratories showed that there was little difference in the requesting practices of clinicians between hospitals where local guidelines relating to the appropriate use of TMs were available.11
Although intelligent software design can be an effective method for managing demand of hospital requests, a more forward-facing approach to engage with primary care users is required. Publication of regular laboratory updates, holding user group meetings, education seminars and anonymously feeding back request data to individual GP surgeries are just some of the ways this may be achieved. Only through direct engagement with our colleagues in primary care can the utility of TMs as well as their limitations be highlighted to the ultimate benefit of the patient.
Take-home messages
There are notable heterogenous requesting patterns from general practitioners for certain tumour markers from the hospital laboratory; some of which may be inappropriate.
For certain tumour markers such as carcinoembryonic antigen, CA19-9 and CA15-3, their use is best for monitoring tumour activity and therapeutic response rather than for screening for initial disease.
Communication between clinicians and the laboratory may reduce the likelihood of inappropriate test requesting as part of demand management.
Interactive multiple choice questions
This JCP best practice article has an accompanying set of multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://jcp.bmj.com/education Please note: the MCQs are hosted on BMJ Learning the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into JCP with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Acknowledgments
The authors would like to thank M Nelson and D Nelson for the tremendous help in collating the data.
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.