Article Text

Abstract
Aims: To investigate the smooth muscle nature of the spindle stromal cells in the capsule of thyroid tumours and tumour-like lesions.
Methods: Immunostaining for high molecular weight caldesmon (HCD), a highly specific marker for smooth muscle differentiation, was performed in 70 primary thyroid tumours and tumour-like lesions (21 hyperplastic nodules, 29 follicular adenomas, five minimally invasive follicular carcinomas, six widely invasive follicular carcinomas, and nine encapsulated papillary carcinomas).
Results: HCD positive stromal cells (HCD+ cells) were detected in the capsule of 20 of the 21 hyperplastic nodules, and all of the 29 follicular adenomas and five minimally invasive follicular carcinomas, whereas HCD+ cells were seen in the capsule of only four of the six widely invasive follicular carcinomas and no HCD+ cells were seen in the capsule of the nine encapsulated papillary carcinomas examined.
Conclusions: The presence of HCD+ cells in the capsule is characteristic of thyroid follicular tumours and tumour-like lesions. The stromal cells in the capsule of thyroid follicular tumours and tumour-like lesions are different from those of encapsulated papillary carcinoma.
- thyroid
- capsule
- high molecular weight caldesmon
- smooth muscle cell
- follicular tumour and tumour-like lesion
- ASMA, α smooth muscle actin
- HCD, high molecular weight caldesmon
Statistics from Altmetric.com
- thyroid
- capsule
- high molecular weight caldesmon
- smooth muscle cell
- follicular tumour and tumour-like lesion
In diagnostic histopathology of the thyroid gland, evaluation of the capsule is most important for distinguishing between benign nodular follicular lesions (hyperplastic nodules and follicular adenomas) and follicular carcinomas.1 Follicular adenomas are completely encapsulated,1 and the tumour capsules are made of fibrous tissue and vessels of various sizes.1 It is relatively common for the capsules of follicular adenomas to contain almond shaped or ovoid masses of smooth muscle bundles, probably representing the thick walls of blood vessels.1 Hyperplastic nodules, follicular adenomas, and carcinomas (both follicular carcinomas and papillary carcinomas) also have sphincteric structures, as revealed by their smooth muscle component (so called muscle cushions) at the inner side of the capsule.2 Recent immunohistochemical analysis using an antibody to α smooth muscle actin (ASMA) confirmed that the muscular cushions connected with vessel walls were present at the periphery of 80% of follicular adenomas and 50% of hyperplastic nodules, whereas they were seen in only 10% of carcinomas (both follicular carcinomas and papillary carcinomas)2; all of these carcinomas with muscle cushions at the tumour periphery developed in thyroid glands affected by long standing hyperplastic nodules.2 Fibrous tissues in the capsule contain spindle stromal cells (fibroblastic cells) between collagen fibres. However, spindle stromal cells in the capsule of thyroid tumours and tumour-like lesions have not been studied extensively.
“In human tissues, high molecular weight caldesmon is more specific for smooth muscle cells than α smooth muscle actin, which is also found in myofibroblasts”
Caldesmon was originally purified from gizzard smooth muscle as a major calmodulin binding protein that also interacts with actin filaments by Sobue et al.3 Two molecular weight forms of caldesmon, high molecular weight caldesmon (HCD) and low molecular weight caldesmon, were purified.4 In particular, HCD, molecular weight 120–150 kDa, is associated with smooth muscle contraction and localised exclusively in smooth muscle cells.4 In human tissues, HCD is more specific for smooth muscle cells than ASMA, which is also found in myofibroblasts.5 Hence, HCD is used as a highly specific marker for smooth muscle tumours.6–11 Recently, we elucidated that colorectal pericryptal fibroblasts are also positive for HCD, suggesting that pericryptal fibroblasts are smooth muscle cells.12
To elucidate the smooth muscle differentiation of spindle stromal cells in the capsule of primary thyroid tumours and tumour-like lesions, we examined the expression of HCD in the capsule of primary thyroid tumours (follicular adenoma, minimally invasive follicular carcinoma, widely invasive follicular carcinoma, and papillary carcinoma) and tumour-like lesions (hyperplastic nodules).
MATERIALS AND METHODS
We examined 70 surgically resected thyroid tumours and tumour-like lesions (21 hyperplastic nodules, 29 follicular adenomas, five minimally and six widely invasive follicular carcinomas, and nine encapsulated papillary carcinomas) from the surgical pathology files of the first department of pathology, Kochi Medical School and its affiliated hospitals from 1979 to 2001. We examined nine encapsulated papillary carcinomas from a total of 25 cases in our surgical pathology case file. The follicular variant of encapsulated papillary carcinoma is very rare, so none of these lesions was examined. We diagnosed all of the thyroid tumours and tumour-like lesions according to the World Health Organisation histological typing of thyroid tumours,13 and also referred to the paper by Rosai et al.1 All minimally invasive follicular carcinomas and widely invasive follicular carcinomas were diagnosed by two attending pathologists (T Moriki and H Kiyoku), who specialise in diagnostic histopathology of thyroid tumours and tumour-like lesions.
Immunohistochemical studies were performed using a Histofine SAM-PO (multi) kit (Nichirei, Tokyo, Japan). A monoclonal antibody against HCD (clone h-CD; Dakopatts, Glostrup, Denmark; 1/50 dilution; microwave treatment) was used.12 In our present study, we defined a rim of peritumoral compressed fibrous tissue containing stromal cells, collagen fibres, and vessels as the capsule of thyroid tumours and tumour-like lesions. We regarded HCD positive cells in the capsule of thyroid tumours and tumour-like lesions to be HCD positive stromal cells (HCD+ cells). We examined HCD+ cells between collagen fibres in the capsule. Vascular media, almond shaped masses,1 ovoid masses,1 and muscle cushions2 were also positive for HCD, and were excluded in our present study.
Figures 1B, 2B, and 3B show the results of HCD immunostaining. Statistical analysis was carried out using Fisher's exact probability test. A p value < 0.05 was considered to be significant.

Immunostaining for high molecular weight caldesmon (HCD) of follicular adenoma ((A) haematoxylin and eosin stain; (B) HCD immunohistochemistry). In the capsule, the spindle stromal cells between the collagen fibres are positive for HCD; HCD positive stromal cells are present.
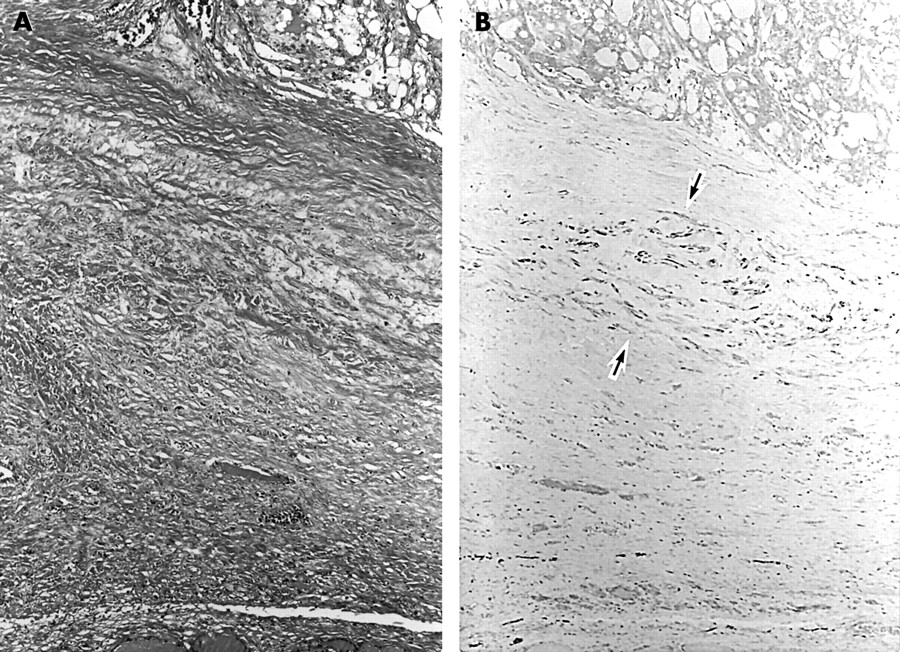
Immunostaining for high molecular weight caldesmon (HCD) of widely invasive follicular carcinoma ((A) haematoxylin and eosin stain; (B) HCD immunohistochemistry). The thick fibrous capsule is composed of spindle stromal cells and hyalinised collagen fibres. HCD positive cells are seen (between the arrows).

{kind=link}
{kind=link}
{kind=link}
Immunostaining for high molecular weight caldesmon (HCD) of encapsulated papillary carcinoma ((A) haematoxylin and eosin stain; (B) HCD immunohistochemistry). The tumour is partially surrounded by the capsule. No HCD positive cells are seen; all of the spindle stromal cells are negative for HCD; vessel walls (vascular smooth muscle cells) are the positive control for HCD.
RESULTS
Normal thyroid tissue
No HCD+ cells were detected. HCD was positive only in vessel walls (vascular smooth muscle cells).
Hyperplastic nodules, follicular adenomas, and minimally invasive follicular carcinomas
HCD+ cells were detected between collagen fibres in 20 of the 21 hyperplastic nodules, all of the 29 follicular adenomas (fig 1A,B), and all of the five minimally invasive follicular carcinomas.
Widely invasive follicular carcinomas
The tumour capsules of the widely invasive follicular carcinomas were generally thick (fig 2A). HCD+ cells were detected between collagen fibres in the tumour capsule of four of the six widely invasive follicular carcinomas (fig 2B).
Encapsulated papillary carcinomas
No HCD+ cells were seen in the nine encapsulated papillary carcinomas examined (fig 3A,B).
Summary of results
HCD+ cells were detected in the capsule of the benign tumours and tumour-like lesions and minimally invasive follicular tumours, whereas they were seen in the capsule of only about two thirds of the widely invasive follicular carcinomas (p = 0.023) and no HCD+ cells were detected in the capsule of the encapsulated papillary carcinomas examined (p = 0) (table 1).
Summary of the presence of high molecular weight caldesmon positive stromal cells in the capsule of benign follicular tumour-like lesions, benign and minimally invasive follicular tumours, widely invasive follicular lesions, and encapsulated papillary carcinomas
DISCUSSION
The examination of the capsule is most important in the diagnostic histopathology of thyroid tumours and tumour-like lesions. The detection of complete capsular invasion is only one criterion that is diagnostic of follicular carcinoma. Although the importance of the thyroid tumour capsule is well known, the components of the thyroid tumour capsule have not been studied extensively, and there are few descriptions in the literature.1,2 In follicular adenomas, almond shaped or ovoid masses of smooth muscle fibres were described in the tumour capsule,1 and recently, longitudinally oriented small muscular cushions composed of smooth muscle fibres were pointed out on the inner side of the capsule of hyperplastic nodules and follicular adenomas.2 However, spindle stromal cells in the capsule of thyroid follicular lesions and papillary carcinomas have not been studied yet.
In our present study, HCD+ cells were easily detected between collagen fibres in the capsule of thyroid follicular tumours and tumour-like lesions. This is the first report to confirm the existence of HCD+ cells in the capsule of human tumours and tumour-like lesions by immunohistochemical analysis with a monoclonal antibody to HCD. The thyroid gland has an extremely rich blood supply.1 The regular vessel array of the thyroid is severely disrupted by the formation of nodules, either by neoplastic or hyperplastic processes.1 Accordingly, tumours and tumour-like lesions cause mechanical stress to vessels surrounding them, resulting in the displacement of the vascular smooth muscle cells. It is possible that the HCD+ cells between collagen fibres in the capsule may be displaced and isolated vascular smooth muscle cells, and that the detection of HCD+ cells is helpful in making a diagnosis of thyroid follicular tumours and tumour-like lesions.
We found no HCD+ cells in the capsule of the encapsulated papillary carcinomas examined. Therefore, the capsule of encapsulated papillary carcinoma is different from that of follicular tumours and tumour-like lesions.
“This is the first report to confirm the existence of high molecular weight caldesmon (HCD) positive cells in the capsule of human tumours and tumour-like lesions by immunohistochemical analysis with a monoclonal antibody to HCD”
Tumour capsular structure varies from one organ to another. No HCD+ cells were detected in the capsule of salivary gland pleomorphic adenomas.14 (The tumour periphery of Warthin tumours, polymorphous low grade tumours, adenoid cystic carcinomas, acinic carcinomas, and mucoepidermoid carcinomas was studied extensively, but HCD+ cells were not examined.15) The cellular components of the fibrous capsule of hepatocellular carcinomas are myofibroblasts,16 which are transformed from hepatic perisinusoidal cells, namely Ito cells.17,18 Kojima et al reported that smooth muscle cells were also detected in the capsule of hepatocellular carcinoma, by immunohistochemical analysis with various smooth muscle markers (desmin, smooth muscle actin (clone 1A4, HHF35, CGA7), and smooth muscle myosin heavy chain (SM1, SM2)) and electron microscopic study.19 Unfortunately, they did not perform immunostaining for HCD. The immunohistochemical markers that they used were not specific for smooth muscle cells, but were also positive in myofibroblasts.5 The results should be confirmed by immunostaining for HCD. As mentioned above, there is a possibility that the cellular components of tumour capsules are organ-specific. To elucidate the organ specificity regarding the tumour capsular components, tumour capsules in various organs should be examined.
Take home messages
-
High molecular weight caldesmon (HCD) is a highly specific marker for smooth muscle differentiation
-
The presence of HCD positive cells in the capsule is characteristic of thyroid follicular tumours and tumour-like lesions but not encapsulated papillary carcinomas
-
The stromal cells in the capsule of thyroid follicular tumours and tumour-like lesions are different from those of encapsulated papillary carcinoma
-
Further morphological and molecular pathological studies are needed to elucidate the origin and the roles of HCD positive cells
In conclusions, HCD+ cells were detected in the capsule of the thyroid follicular tumours and tumour-like lesions examined, but not in that of encapsulated papillary carcinomas. The capsule of thyroid follicular tumours and tumour-like lesions is different from that of encapsulated papillary carcinomas. There is a possibility that the presence of HCD+ cells is associated with the growth regulation of follicular tumours and tumour-like lesions. To elucidate the origin (whether HCD+ cells are displaced and isolated vascular smooth muscle cells or not) and the roles of HCD+ cells, further comprehensive morphological and molecular pathological studies are needed.
Acknowledgments
Thanks to Ms H Yamasaki, Ms M Yamamoto, Mr T Tokaji, and Mr Y Hayashi, First Department of Pathology, Mr M Shirota, Medical Research Center, Kochi Medical School, and Ms M Mitani, Mr S Ueda, and Ms M Ichien Pathology Section, Department of Laboratory Medicine, Kochi Medical School Hospital for their excellent technical assistance.