Robots in operating theatres
BMJ 1995; 311 doi: https://doi.org/10.1136/bmj.311.7018.1479 (Published 02 December 1995) Cite this as: BMJ 1995;311:1479
- aSouthmead Hospital, Bristol BS10 5NB
- bAdvanced Manufacturing and Automation Research Centre, Faculty of Engineering, University of Bristol, Bristol BS8 1TR
- Correspondence to: Dr R O Buckingham
- Accepted 30 August 1995
Robots designed for surgery have three main advantages over humans. They have greater three dimensional spatial accuracy, are more reliable, and can achieve much greater precision. Although few surgical robots are yet in clinical trials one or two have advanced to the stage of seeking approval from the UK's Medical Devices Agency and the US Federal Drug Administration. Safety is a key concern. A robotic device can be designed in an intrinsically safe way by restricting its range of movement to an area where it can do no damage. Furthermore, safety can be increased by making it passive, guided at all times by a surgeon. Nevertheless, some of the most promising developments may come from robots that are active (monitored rather than controlled by the surgeon) and not limited to intrinsically safe motion.
Research into the use of robotic technology in operating theatres has reached a critical stage in the United Kingdom and around the world. Many systems that can be described as “robotic” are now working in laboratories, and some are undergoing trials in operating theatres. Although the United States leads in this work, Europe is well placed since the litigious nature of American society makes full clinical use a risky venture.
Robots designed for surgery have three main advantages over humans. Firstly, they have greater three dimensional spatial accuracy, especially when linked to scanning technology. Secondly, systems can be designed to be more reliable and produce more repeatable outcomes, and, finally, robots can achieve a precision at least an order of magnitude greater than that achievable by humans. This article explains some of the background to the development of surgical robotics and illustrates the current state of the technology by describing some of the leading developments from around the world.
Possibilities and problems
The most exciting reason for pursuing robotic technology is the new possibilities it opens up. For instance, consider a computer controlled endoscope that can “follow its nose” to a predefined site. The advantages of being able to avoid damage to normal tissue, whether in the brain or bowels, while reaching the most restricted operating sites would be enormous. In addition, if the skin of the device is coated with sensors that could not only measure force but also the concentration of a chemical or fluid flow the surgeon would know the position of the device and the nature of the surrounding tissue. Imagine a device which, having been told to go to the site of a tumour, could track along the safest path and find the required site even though it may have moved because of the action of the device. Such technology may seem to belong to the world of Star Trek or cruise missiles but the technology will certainly be available in the next decade (Buckingham RO, Sandeman D, Graham A. Medimec ‘95—2nd international workshop: mechatronics in medicine and surgery, Bristol, September 1995).
It also does not take a huge leap to consider robots that can be controlled remotely. Telerobotics could be used in situations that are inaccessible to a particular skilled surgeon—for example, on a battlefield, in space, or under the sea.1
The whole subject of micromachines, although not the topic of this article, is another which will undoubtedly affect invasive surgical procedures. The machines, smaller than a pin head, could be the manmade white cell of the future, instructed to seek out and destroy specific molecules or tissue.
These are dreams that may become reality but for the present one of the key issues is safety. Safety is a primary concern of all the research teams around the world, and the fate of devices currently seeking approval from the British Medical Devices Agency and the US Federal Drugs Administration is being closely watched. Convincing people of the safety of a surgical robot might prove to be the biggest challenge to their implementation.
What is a robot?
According to the Robot Institute of USA, a robot is “a programmable multifunctional manipulator designed to move materials, parts, tools, or specialised devices through variable programmed motions for the performance of a variety of tasks.” A slightly simpler definition is, “Robotics is the intelligent connection of perception to action.”2 Engelberger, one of the robot patriarchs, said, “You know one when you see one!” and this may yet prove to be the most appropriate definition for surgical robotics. Within the context of surgical devices, however, it is more appropriate to define a “robotic device.” This is a machine with some but possibly not all the features of a robot. In fact, because they need to work in an operating theatre these devices will probably be quite unrecognisable as the stereotyped industrial robot. This is certainly true of the devices described below.
Rehabilitation robotics
The history of surgical robotics lies partly in rehabilitation robots, and there are lessons there for surgical robotics. Rehabilitation robotics is concerned with aids to help people who have manipulative disabilities and raises the important issue of robots interacting directly with people. A typical application would involve a robot arm attached to a wheelchair or to furniture within the working area, which would enable the person to eat and drink, to work or study, or to exercise.
Much research has been conducted into these devices and has resulted in many demonstrator systems,3 4 5 6 7 8 9 although few are commercially available. One that is now in long term trials with disabled users is RAID (robot for assisting the integration of the disabled; see fig 1.10 This uses a low powered robot arm driven by software and controlled using an extremely simple input device. Low powered here means that the arm has less power than that of a small child and is slower too. This is a useful approach to safety when humans have to interact with robots. The system, designed by Oxford Intelligent Machines Ltd, costs about pounds sterling50000 and has been designed to allow computer based work in an office.

computer controlled RAID (robot for assisting integration of the disabled) in operation in an office environment
{kind=link}
Rehabilitation robotics is perhaps five years ahead of surgical robotics, and the main lesson learnt from these projects is the need for the user to define the system. The needs of the surgeon must be considered at all times to design systems that are appropriate for current operating theatres.
Surgical robotics
Within the Advanced Manufacturing and Automation Research Centre (AMARC) in Bristol two classifications are used to describe the complexity of robotic technology in the operating theatre. The first is a distinction between active and passive mechanisms and the second is whether or not the device is intrinsically safe. This simple categorisation has the advantage of focusing attention on two overriding features: who or what is controlling the device—surgeon or computer? and if things go wrong what damage might occur?
A passive mechanism is one where the surgeon provides the physical energy to drive the surgical tool; an active mechanism is one where motion is achieved using non-human powered devices and probably involves a computer. Active mechanisms, by definition, have a degree of autonomy, although the surgeon must at least be able to monitor the complete process and intervene if the procedure is not going according to plan. Some devices will move from being passive to active within a single procedure.
An intrinsically safe design is a mechanism that has physically restricted motion so that all possible movement is safe. Errors in software or incorrect use of the device may still override an intrinsically safe mechanism, but an intrinsically safe design should be viewed as a target in the design process.
The first surgical systems have tended to be both passive and intrinsically safe. Typically the next step has been to introduce some form of active motion to these devices, and the most advanced systems now have some active motion that is not intrinsically safe. The examples given below are shown on a simple graph that indicates this trend 2. This does not imply that the passive systems are less important or out of date, merely that the field is expanding to include active systems.

Grid showing where current robotic developments lie on the scales for instrinsic safety and active/passive
{kind=link}
Neurosurgery
Neurosurgery is an important test case for robotic technology, because the cranium contains the brain in a fairly rigid manner and provides fixed landmarks which can be used as datums. In comparison abdominal surgery has the disadvantage that everything moves around, making perception extremely important, and this is just where robots fall down.
NEURONAVIGATORS
In neurosurgery devices fall into three broad types: neuronavigators, stereotactic devices, and robotic devices used as stereotactic frames. The wand is an example of a neuronavigator 3 which is both passive and intrinsically safe. It was developed by ISG Technologies and has been used mainly in head surgery (Sandeman D, Marshall C, Brett P. Medimec ‘92, Malaga, 1992). It uses fiducial markers to register the patient's head at the time of surgery with respect to previously acquired maps of the tissue acquired through computer aided tomography or magnetic resonance imaging. Once registered, wherever the surgeon places the tip of the wand, either on or within the head, the “wand's eye view” is shown on the monitor. The image is displayed as a three dimensional solid model or as user defined sections through the head.

The wand, a neuronavigator, being used in neurosurgery
{kind=link}
The basic technology is a robotic arm which is moved by the surgeon. The computer interrogates the position of each joint to determine the position and orientation of the tip and then calculates which view of the data to show on the screen. The wand is a completely passive device, but the data could be misleading for several reasons: inexact registration, a joint-position-sensor malfunction, movement at the base of the wand relative to the patient, or movement of flexible tissues during the operation. So it is essential that the surgeon controls the wand and not the other way round.
When the wand is used correctly the enhanced three dimensional spatial awareness reduces the time needed in the operating theatre. This goes some way to providing a financial case for what is not a cheap piece of hardware.
STEREOTACTIC FRAMES
Also there are now several motorised stereotactic frames on trial.11 These frames are reconfigurable orientation devices that act as a stable base for the incursion into the patient. The spherical configuration favoured in most designs is used because it has many intrinsically safe features (Buckingham R O, Buckingham R A, Wood-Collins P, Brett P, Khodabandehloo K. Medimec ‘92, Malaga, Oct 1992) and is close to the design of manual frames. The frame can be designed so that no driven link can come into contact with the patient unless the patient is wrongly positioned. The surgeon can also verify the position and orientation of the tool axis, and once in position the frame can be locked in place.
From this stable base tools can move in a straight line to the biopsy site. This motion could be physically limited while under the control of a surgeon using a joy stick or push buttons. These devices are particularly powerful when used in conjunction with the computer graphics that can be produced from computer aided tomography, magnetic resonance imaging, and other scanning techniques. These can be used to plan safe paths, the data being passed directly to the motorised frame.12 The drawback with single axis tool motion is that, while such a system is ideal for removing pips from an orange, the direct line to a deep seated biopsy site may be obstructed by blood vessels or vital brain structure, making only surface brain operations feasible.
ROBOTIC FRAMES
A number of robots have been used to achieve the same result as motorised stereotactic frames. Drake used a PUMA 200 robot to help in the resection of thalamic astrocytomas in six children.13 In this case a surgical retractor was held and manipulated by the robot, the position and orientation of the retractor being displayed on a three dimensional display using computer aided tomography and digitised cerebral angiograms.
Another stereotactic robot has been designed by the large research team at Grenoble which positions a probe holder to allow access to a given target.14 This device has already been used for 140 procedures over 14 months.
Perhaps the future of robotics in operating theatres is best illustrated by the work of the Lausanne Research Group, which has built the new robot Minerva.15 16 Minerva was designed to meet an exacting specification which considered safety, geometry, rigidity (and hence accuracy and repeatability) for the task of one dimensional incursions into the brain while the patient is within a computer aided tomography scanner. The advantage of operating within the scanner is to use real time scan data to reprogram the robot during the procedure. Costing in the region of pounds sterling1m, excluding the scanner, these systems are not likely to be available in every general hospital, but rather in specialised hospitals where the skill is on hand to use the systems efficiently.
Although not an aid to neurosurgery, AESOP (automated endoscope system for optimal positioning) is in many ways a similar type of device to those used in neurosurgery, which acts as an extra pair of hands.17 It assists in laparoscopies by holding and moving the laparoscope to any chosen position with any orientation. The device can be repositioned using a simple hand control or foot pedal, and its speed of movement is determined by pressure on the control. Two useful features are, firstly, that the surgeon can take manual control at any time and, secondly, that the robot can return to a memorised position on command.
Orthopaedics
Robotics also has a special place in orthopaedics, because bones are rigid and can be fixed in known positions. The main use of orthopaedic robots is to cut and ream bones with great precision for the fitting of joint prostheses or for replacing ligaments.
Paul et al developed a robot which prepares the proximal femur to accept the femoral component of an uncemented total hip replacement.18 The aim is to produce total contact of the prosthetic stem with the femoral medullary canal to increase stability of the implant. Current methods of femur preparation allow the prosthesis to make contact with the bone over only 18-20% of its surface. The robot can create a cavity to house any make of prosthesis, accurate to within 0.4 mm—10 times more accurate than conventional reaming with 90% surface contact. To orientate the robot with respect to the bone, markers are fixed to the bone which show up on computed tomography. These markers are then used for preoperative registration. A similar system has been proposed for total knee replacement19 and is currently undergoing trials in cadavers.
Work by Lavallee at Grenoble has shown the feasibility of creating a computer model of a knee from measurements of the real knee to identify the insertion sites for replacing the anterior cruciate ligament (Lavallee S, Dessenne V, Juillard R, Orti R, Martelli S, Cinquin P. 1st International Symposium on Medical Robotics and Computer Assisted Surgery, Pittsburgh, 1994). These data can then be used to direct a robot to drill holes in the femur and tibia to accept the new ligament and maximise the movement of the repaired knee.
Urology: prostatectomy
The robotics group based at Imperial College, London, has designed and implemented a new robotic device based on the concept of the stereotactic frame for transurethral resection of the prostate. There were a number of stages in the development of the device, which is now a test case within the UK as it has reached the stage of seeking approval from the Medical Devices Agency. The first stage was for a robot to hold a hot loop diathermy tool and make conical cuts in a potato (the next best thing to a prostate). The industrial robot was then replaced by a manually driven frame, similar to a stereotactic frame, designed specifically for the task. Typically industrial robots are designed for a range of tasks that require different capabilities—for example, high speeds while carrying heavy loads, which make them inappropriate for operating theatres.
The important concept in the design was that the tool could cut only within a physically restricted volume, making the device intrinsically safe. The final stage was to redesign the system to be motorised and controlled via the computer.20 21 The system stands every chance of being approved since, although it is an active device, it has been designed to be intrinsically safe. The key questions will probably revolve around software reliability, the ability for the surgeon to take over in an emergency, and how to ensure that the equipment is used correctly. Training is obviously important for the last point, but so is a set up sequence that must be followed precisely before the system becomes active.
ENT: stapedotomy
Stapedotomy involves replacing the stapes with a prosthesis to regain mobility of the ossicles in osteosclerosis. Most of the stapes is removed, leaving just the footplate, through which a hole 0.6 mm in diameter is drilled. This houses the prosthesis, which is then attached to the incus. The footplate measures 1.5x2 mm and has a thickness of 0.2 to 2.5 mm. The challenge is to avoid penetrating the oval window during the drilling.
Brett at Bristol's Advanced Manufacturing and Automation Research Centre has developed a robotic technique to drill the hole with minimum protrusion by monitoring the drill cutting force and the motor torque in real time.22 The profile of these two curves is used to identify the onset of breakthrough. The device is currently hand held, but the drill feed is controlled by the computer 4. The computer control system decides when to stop the drill feed. This is just before breakthrough since on breakthrough the footplate will inevitably spring back, with the danger of puncturing the membrane. The tool then backs off to release the spring tension in the footplate and calculates where the bone has relaxed to before finishing off the hole.
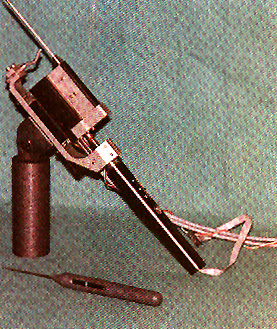
Robotically controlled device for drilling the footplate of the stapes. Computer control ensures that it stops drilling just before it breaks through the stapes
{kind=link}
Since the thickness of the bone is unknown it is impossible to restrict the forward motion of the drill to a known safe level; hence this mechanism is both active and not intrinsically safe. A malfunction could cause irreparable damage to the inner ear. Nevertheless, from realistic cadaveric trials the surgeons are convinced of the substantial improvement in hole quality compared with current techniques.22
This device is fully based on robotic technology but looks nothing like a typical robot. Like Minerva, it has been designed for a specific task, although at a cost of thousands its use could eventually be widespread.
Conclusions
s
Robots designed for surgery have been shown to have three main areas where they perform better than humans. Their accurate spatial awareness is used in neurosurgery with the wand and motorised stereotaxy. Reliability and repeatability are the important qualities of the Imperial prostatectomy device and the automated endoscope. And the delicate precision is over-whelmingly the important feature of the stapedotomy device. The motorised endoscope then takes the technology beyond the capabilities of people. The task of controlling a large number of motors, taking into account sensory feedback from a number of different sources, can be achieved only by using computer technology. It is at this stage that the surgeon does become more of an observer than a controller. This level of technology will then necessitate a clear understanding of all the safety issues.
Current health and safety guidelines for industrial robots state that robots must be confined within an area from which all staff are excluded, yet we are proposing to allow devices that are akin to robots next to and even inside patients. Highly sophisticated safety systems must be an intrinsic feature of such systems.