Article Text

Statistics from Altmetric.com
Helicobacter pylori causes chronic gastritis with variable activity and topographic distribution. Patient age at acquisition, expression of gastritis, strain virulence, host factors, and environmental factors determine the outcome of the infection. Well established consequences are peptic ulcer disease (PUD) and gastric neoplasia.1-4
As duodenal ulcer is often associated with gastro-oesophageal reflux disease (GORD),5 and antral gastritis is a frequent finding in patients with reflux disease,6 H pyloriinfection may be a common cause of both conditions. Our aim was to explore the strength of the postulate that H pyloriis a causal factor in GORD by reviewing publications on epidemiological studies, clinical observations or treatment trials, and identifying possible pathogenic mechanisms.
Association of H pylori and GORD
Currently, we have no clear data to show that patients with GORD are more frequently infected by H pylori than controls, neither in adults nor in children.7 Indeed, a recent well designed case control study from Japan showed a significantly lower incidence of H pylori infection in patients with reflux oesophagitis than in age and sex matched controls.8 This finding is supported by one of our own studies.9 The prevalence of both H pylori infection and GORD increases with age.10 ,11 Male sex is a risk factor for GORD,12 but the prevalence of H pylori is equally distributed between men and women.10 ,12
H pylori is able to colonise Barrett’s epithelium. Many uncontrolled studies showed H pylori prevalence rates similar to those in the background population.7 Also, in a controlled study the prevalence of H pylori infection was similar in patients with Barrett’s oesophagus and controls.13 However, patients with Barrett’s oesophagus and an ulcer within the columnar metaplasia were more frequently infected by H pylori than those without ulcers.14
The prevalence of H pylori infection is decreasing steadily in white adults in developed countries.15 This is paralleled by an increasing incidence of primary adenocarcinoma of the oesophagus as a consequence of reflux disease.16 Moreover, adenocarcinomas in the oesophagus are uncommon among black patients16 who have a high prevalence of H pyloriinfection,17 and a recent study suggests thatH pylori induced gastritis may protect against cancer of the cardia.18 These epidemiological data do not primarily support a role for H pylori in GORD, but this finding does not rule out the pathogenic importance of the infection in H pylori positive reflux disease. Moreover, the infection might be involved in the pathogenesis of Barrett’s ulcer. In contrast, the epidemiological data tend to support the hypothesis that H pylori infection may protect to some extent against reflux disease and, most importantly, against adenocarcinoma of the gastro-oesophageal junction. Cancers at this site are now recognised as a possible complication of GORD.
Current concepts of the pathogenesis of GORD
Gastro-oesophageal reflux disease is a common disorder characterised by abnormal exposure of the oesophageal mucosa to acidic gastric contents. This may cause symptoms or mucosal damage, or both, of variable severity. Primarily, GORD is a motility disorder associated with incompetence of the lower oesophageal sphincter (LOS) and crural diaphragm. The spectrum of disturbances of the LOS extends from inappropriate transient relaxations to a persistently low basal pressure.19 ,20 Although acidity in the oesophagus is a key factor in the pathogenesis, gastric acid secretion is similar in patients with reflux oesophagitis and appropriate controls.21 However, patients with very high acid secretion are at risk of developing reflux oesophagitis,22and gastric acid hypersecretion has been found in refractory GORD.23 A substantial proportion of patients with GORD have delayed gastric emptying24 which might adversely affect the response to medical treatment.25 Furthermore, a high gastro-oesophageal pressure gradient—for example, as a result of disturbed gastric accommodation to a meal,26 motility disorders of the oesophagus with delayed clearance of refluxed gastric contents,27 impaired mucosal defence mechanisms,28 ,29 diminished production of saliva,30 and environmental factors such as a high fat diet, smoking and alcohol consumption, may contribute to this multifactorial disease.31-33
Mechanisms by which H pylori might contribute to the pathogenesis of GORD
H pylori frequently colonises the gastric cardia and may, in turn, exert direct and indirect effects on the LOS.34 In patients without reflux oesophagitis, density ofH pylori and severity of gastritis in the cardia and antrum are similar,34 probably because the type of gastric epithelium and the local pH that determines the growth behaviour ofH pylori are quite similar in these regions of the stomach.35 In patients with reflux oesophagitis, however, we observed lower cardial gastritis activity and lower bacterial density.36 We assume that this phenomenon is secondary to increased exposure of the cardia to acid in reflux disease.
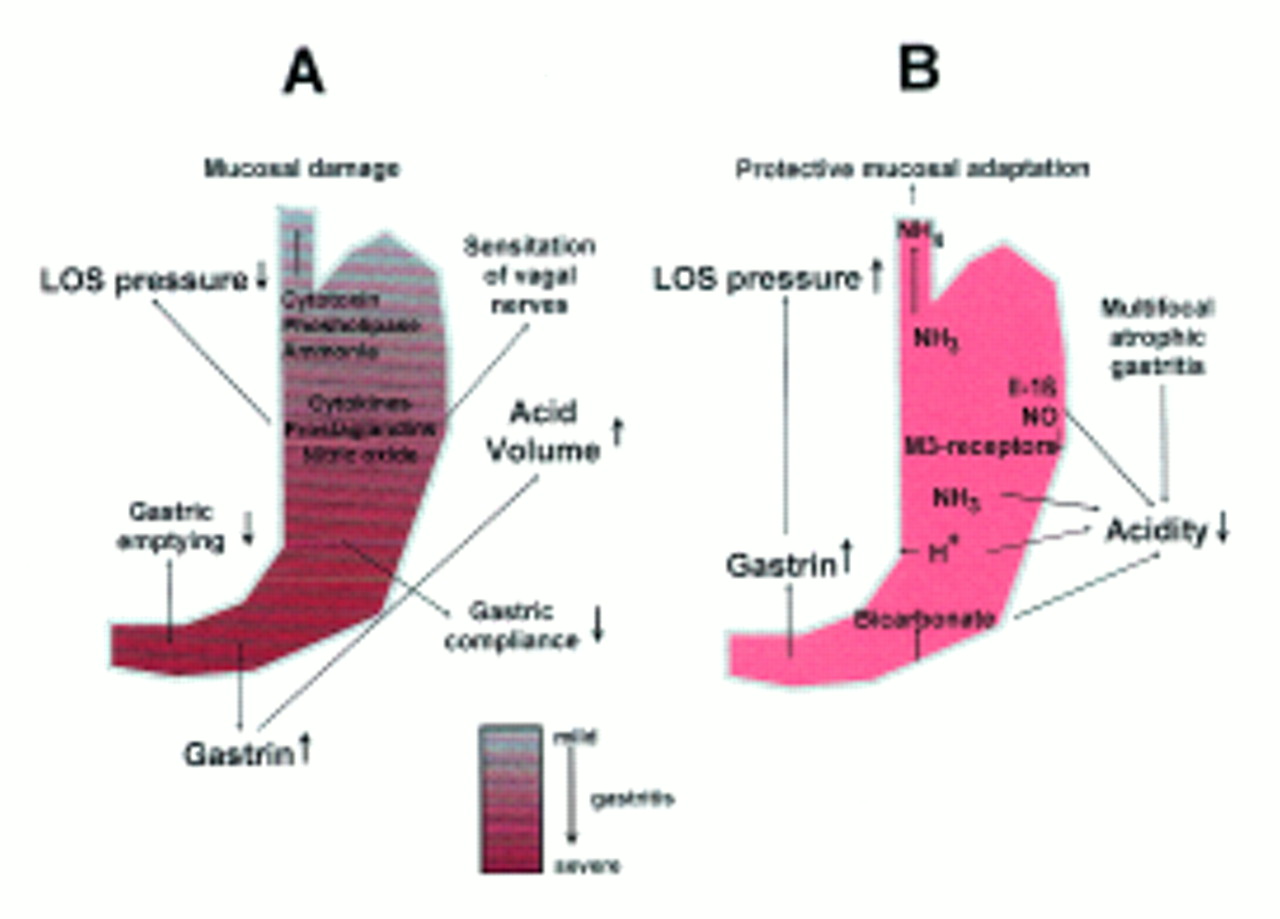
H pylori gastritis is accompanied by the release of numerous mediators, cytokines and nitric oxide37 ,38 which may adversely affect the LOS39 ,40 and possibly promote an inflammatory response in, and mucosal damage to, the adjacent oesophageal mucosa. Also, H pylori infection leads to increased production of prostaglandins41 which, in addition to inflammatory mediators, can sensitise afferent nerves and reduce LOS pressure.42 There is good evidence to indicate that the excessive production of prostaglandins in reflux oesophagitis drives a vicious cycle of LOS dysfunction, reflux, mucosal inflammation, aggravated LOS dysfunction, and further reflux.43 Hypothetically, inflammation in the upper part of the stomach may lower the threshold for triggering transient relaxation of the LOS—for example, by altering the sensitivity of vagal sensory receptors.44
It has been shown convincingly that H pylori infection with antrum predominant gastritis is associated with an augmented gastrin release, both in the fasting state and after infusion of gastrin-releasing peptide.45 This also holds true for healthy subjects and patients with duodenal ulcer. It is conceivable that, at least in some patients with GORD, increased acidity along with a higher volume of gastric juice may aggravate reflux disease.
About half of the patients with GORD show some degree of delayed gastric emptying. Antral gastritis may interfere with gastric emptying, and some studies suggest abnormalities of gastric motor function inH pylori infected dyspeptic subjects,46 but data on this are controversial.47-51
H pylori may theoretically affect the compliance of the gastric wall, and in this way favour gastro-oesophageal reflux by increasing the gastro-oesophageal pressure gradient after a meal. However, a recent study investigating the mechanical properties of the gastric wall failed to find any differences between healthy subjects and patients with functional dyspepsia either with or without H pylori infection.52 Studies in patients with reflux are still lacking.
Direct injurious effects on the oesophageal mucosa could also be caused by bacterial factors such as cytotoxin, phospholipase and ammonia derivates, which might well be strain dependent.
Mechanisms by which H pylori might protect against GORD
H pylori infection may lower intragastric acidity. In vitro, H pylori has been shown to release substances that inhibit gastric acid secretion.53 ,54 Moreover, H pylori generates large amounts of ammonia.55Ammonia has a high pKa of 9.1 and acts as a powerful neutralising substance at elevated gastric pH while having no effect on the physiological pH in the spontaneously secreting stomach. Ammonia could, therefore, decrease the corrosive potential of the gastric juice refluxing into the oesophagus where the pH is high.
The amount of acid secreted in the infected stomach largely depends on the severity of corpus gastritis. More severe corpus gastritis is associated with lower acid output that returns to normal when the infection has been cured.56 ,57 This effect is probably mediated by cytokines such as interleukin-1β, nitric oxide and a loss of M3 receptors in moderate, but not in mild, corpus gastritis.58-61 Bicarbonate leakage from the inflamed mucosa and intramural back-diffusion of acid may also lower the acidity in the infected stomach.62 Finally, H pylorigastritis may progress to multifocal atrophic gastritis with destruction of gastric glands and, in turn, hypochlorhydria.63 That corpus gastritis plays a critical role is supported by a study showing that patients with reflux symptoms without oesophagitis more often had active corpus gastritis than did patients with GORD with erosive oesophagitis.64 Also, the severity of corpus gastritis before cure of H pyloriinfection in patients with duodenal ulcer was a risk factor for the development of reflux oesophagitis after the cure.65
It has been shown repeatedly that H pylori infection is associated with raised serum gastrin concentrations that decrease after cure of the infection.45 ,66 Although controversial, gastrin, even at physiological concentrations, may increase the LOS pressure.67 ,68 This effect might even be more pronounced in patients with reduced acid output as a consequence of moderate to severe corpus gastritis.
Ammonia leads to protective mucosal adaptation in the rat stomach.69 As ammonia appears in the gastric juice refluxing into the oesophagus, it is conceivable that ammonia, like other mucosal irritants,20 may also lead to protective adaptation of the oesophageal mucosa.
Clinical observations and H pylori treatment trials
Anecdotal reports indicate that some patients with GORD experience relief from reflux symptoms following the cure of H pyloriinfection. Controlled studies on this issue are, however, still lacking. In a prospective clinical study in patients with functional dyspepsia, we found H pylori infection to be more frequently associated with reflux symptoms.70 It has also been reported that patients with reflux-like functional dyspepsia may benefit from cure of the infection,71 and this holds true for some patients with peptic ulcer disease and reflux symptoms.72-74 However, these studies were uncontrolled, and reflux symptoms such as heartburn or regurgitation, which were considered in all these studies, are not specific.75
Conversely, it has been reported that reflux oesophagitis may develop in healthy subjects and in patients with duodenal ulcer after successful treatment of H pyloriinfection.76 ,77 As GORD is a common disorder, this finding in small scale studies may be coincidental. However, in a large, controlled study we found that about one quarter of patients with duodenal ulcer cured of their H pylori infection developed endoscopically diagnosed reflux oesophagitis within three years of cure. This was double the rate we observed in patients with duodenal ulcer with ongoing infection.65
Impact of H pylori on the efficacy of antisecretory drugs
Proton pump inhibitors (PPIs) are without doubt the most effective drugs in the control of GORD.78 Pharmacological studies showed that omeprazole is less effective, with respect to acid control, in healthy subjects than in patients with duodenal ulcer79 ,80 despite the known acid hypersecretion in the majority of the latter. In healthy subjects, omeprazole was less effective in the absence of H pyloriinfection,81 and curing the infection noticeably decreased the pH increasing effect of omeprazole over the short and long term,82 with neutralising ammonia generated by H pylori being the most likely explanation.83 Similar experiments in patients with duodenal ulcer confirmed these observations.84 The loss of efficacy of ranitidine on nocturnal intragastric acidity after cure of the infection was less pronounced.85 As intragastric pH is linearly related to the healing rate of reflux oesophagitis78 and as, within a 24 hour period in patients with duodenal ulcer, the total time during which the pH was ⩾4 was twice as long before the cure of H pylori infection as after,86 studies in reflux patients with special emphasis on the dosage of a PPI needed after the cure are urgently required to determine the clinical relevance of this observation.
Does H pylori increase the risk of maintenance treatment with antisecretory drugs?
Several studies have shown that treatment with PPIs is associated with worsening of corpus gastritis in H pylori infected patients.87 ,88 There is also circumstantial evidence that lower gastric acidity is associated with a higher than usual incidence of atrophic gastritis.89 The first (and only) controlled study suggested that PPI maintenance treatment in H pyloripositive patients with GORD may accelerate the development of atrophic corpus gastritis.90 However, this study is scientifically flawed by incorporation of an inappropriate control group. An FDA Advisory Committee, therefore, concluded that there is no evidence whatsoever that long term treatment with antisecretory drugs increases the risk of gastric atrophy, intestinal metaplasia, or gastric cancer. Although we agree with the experts final conclusion, we are not convinced that increased severity of corpus gastritis is completely without relevance, as a recent case control study has suggested that corpus predominant gastritis in terms of mono- and polymorphonuclear cell infiltration increases the risk of gastric cancer.91
Conclusions
The inter-relation between H pylori infection and GORD is complex and not fully understood. Epidemiological data have not shown that patients with GORD are more likely to be infected withH pylori, but there are plenty of possible mechanisms by which the infection could theoretically contribute to this multifactorial disease (fig 1). Clinical observations and the results of H pylori treatment trials are not conclusive, and appropriately controlled eradication studies in patients with reflux disease are urgently needed. Epidemiological data, pathogenic considerations and the observation that curing the infection increases the risk of reflux oesophagitis in patients with duodenal ulcer are consistent with the hypothesis that H pylori infection may, at least in some patients, protect against reflux disease (fig 1). The topography of H pylori gastritis could be the crucial point, with an antrum predominant gastritis aggravating reflux disease and pangastritis or corpus predominant gastritis protecting the oesophagus against damage by gastric juice. Curing the infection in GORD may have the disadvantage of reducing the efficacy of antisecretory treatment; conversely, it may prevent worsening of corpus gastritis. Further studies are urgently needed to identify those patients in whom H pylori is a friend/foe of the oesophagus, and to permit the development of clinical guidelines on a sound scientific basis.

{kind=link}
: Proposed mechanisms by which H pylori infection could aggravate (A), or protect against (B), GORD. In condition A the gastritis is antrum predominant (antrum > corpus). In condition B the gastritis involves all regions of the stomach to the same degree (corpus ⩾ antrum). It is of note that the cardia is always inflamed.