Article Text

Abstract
Solid pseudopapillary tumours (SPT) of the pancreas are uncommon, but with widespread and increased imaging, several of these lesions are coming to light incidentally and are subject to needle biopsies. On limited material and especially the solid or clear cell, variants of SPT can morphologically mimic most notably pancreatic neuroendocrine tumours and even metastatic renal cell carcinoma or melanoma. In this context, immunohistochemistry is important and useful in helping to reach the correct diagnosis. Several antibodies have been used in the immunohistochemical evaluation of SPT. As with most tumours, no one marker is specific, but rather a core panel is advocated. Recently, both β-catenin and E-cadherin have been shown to be of value in SPT. Nuclear and cytoplasmic decoration of tumour cells by β-catenin is seen in almost 100% of cases. This protein relocalisation away from the cell membrane is underscored by mutations of the β-catenin gene. Mutations of the CDH1 gene are very uncommon in SPT, but the immunohistochemically detected changes to the protein are consistent and present in 100% of cases. Using an E-cadherin antibody to the extracellular domain of the molecule results in complete membrane loss, while the antibody directed to the cytoplasmic fragment produces distinct nuclear staining of the tumour cells. In addition, there is concordance of staining abnormalities between the two antibodies. When combined with CD10 and progesterone receptor positivity, a diagnosis of SPT can be rendered with confidence even in small biopsy samples.
Statistics from Altmetric.com
With the advent of sophisticated, high-resolution non-invasive imaging techniques, the detection of incidental small lesions throughout the body is increasing. Imaging of the pancreas has kept pace with this growing trend, resulting in smaller lesions being detected and investigated. So-called incidental pancreatic cystic lesions are being increasingly documented, and a recent publication quotes an incidence of 0.2–0.7%.1 Although techniques such as multidetector computed tomography and magnetic resonance pancreatography allow for detailed visualisation and characterisation of pancreatic cysts, pathological and/or cytological evaluation remains the gold standard when it comes to reaching a definitive diagnosis. In concert with this, more image-directed needle biopsies are being sent for pathological evaluation. Inherent in this are the pitfalls of sample size and representativity, two factors that add to diagnostic difficulty even in the best of circumstances. With limited material the pathologist tends to be more dependent on ancillary techniques to confirm a morphological opinion, and immunohistochemistry is still the bedrock, routine investigation that is resorted to. Besides pancreatic pseudocysts, other intrinsic cystic lesions of the pancreas that are important are: serous cystic neoplasms, mucinous cystic neoplasms, intraductal papillary mucinous neoplasm and solid pseudopapillary tumours (SPT).2
SPT is an uncommon primary pancreatic tumour, constituting 1–2% of all exocrine tumours of the pancreas and about 5% of cystic pancreatic tumours.3 Although its origin is still conjectural and slightly controversial, the weight of evidence points towards ductal origin.3 In general, it is a low-grade malignant tumour associated with a good prognosis after surgical excision even though widespread liver metastases and vascular invasion have been reported.4 Invasion into surrounding organs such as the spleen and duodenum is rare.3
Histologically, it is quite characteristic, if not diagnostic, in most resected cases. However, there are variants such as the predominantly solid example and even a clear cell variant that may cause mimicry of other tumours.5 The histological mimicry is heightened in needle core samples.
Recently, a few new markers that are important in the immunohistochemical work-up of SPT have emerged in the literature. The purpose of this overview is to highlight briefly the histological differential diagnosis of SPT, enumerate the various immunohistochemical markers that have been used traditionally in the work-up of SPT, discuss the more recent markers that are of diagnostic value in the identification of SPT and, finally, to provide a rational approach to the immunohistochemical work-up and diagnosis of these tumours.
HISTOLOGICAL DIFFERENTIAL DIAGNOSIS
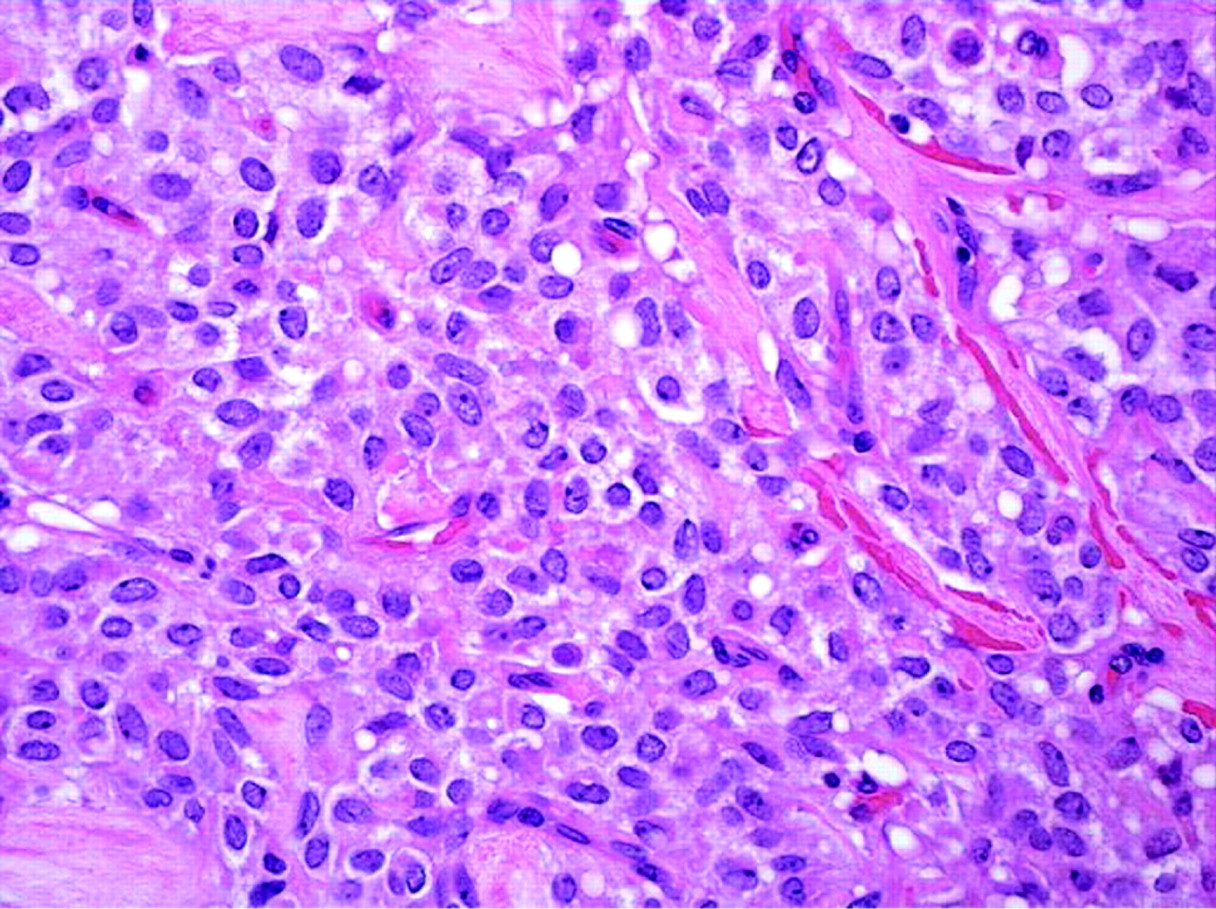
As mentioned already, in the majority of cases, SPT is readily identifiable, and immunohistochemistry serves merely as a confirmatory tool. However, in limited material, pancreatic neuroendocrine tumours (which can also show pseudopapillary areas), acinar cell carcinoma, metastatic clear cell renal carcinoma, metastatic melanoma and even pancreaticoblastoma may display histological overlap with SPT, especially the more solid examples (fig 1) and it can be difficult to separate them on morphological grounds alone.

IMMUNOHISTOCHEMICAL MARKERS USED IN SPT
A wide variety of markers have been employed in the investigation of SPT. For the sake of completeness, we will mention also that enzyme histochemistry for trypsin, α-1-anti-trypsin, chymotrypsin, amylase and lipase have also been used to stain SPT. These enzymes have given inconsistent results and may be either positive or negative in SPT. The most consistent positivity is seen with α-1-anti-trypsin. Trypsin and chymotrypsin are positive in approximately 20% of cases of SPT, exhibiting sparsely granular staining in the cytoplasm with a focal localisation.
In addition, they do not aid in separating SPT from acinar cell carcinoma, which is also positive for trypsin, α-1-anti-trypsin and chymotrypsin. These histochemical stains are often messy and difficult to interpret.
CD10
CD10 or neutral endopeptidase 24.11 or neprilysin is involved in the catabolism of biological modulators and is ubiquitously distributed in various tissues.6 In both human adult and fetal pancreas, CD10 has been reported to be positive in the luminal aspect of ducts and acini.
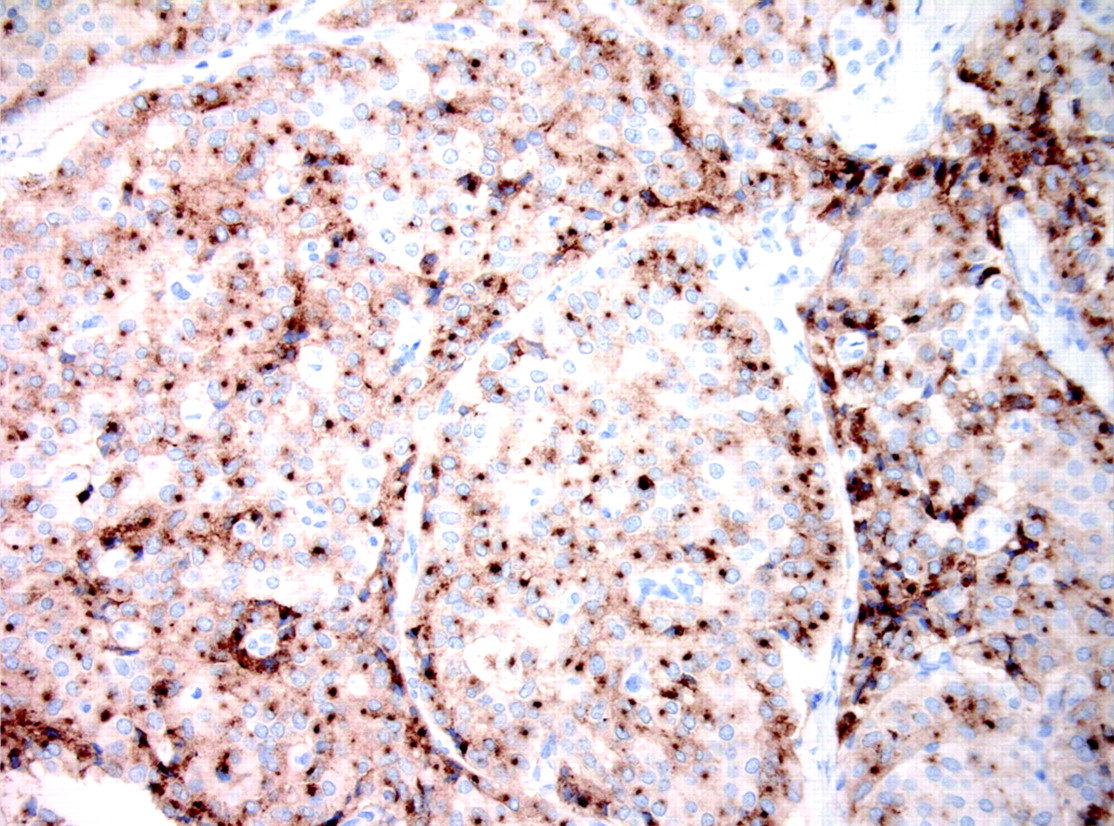
CD10 immunoexpression is a consistent feature of SPT (up to 80% of cases are positive) and is usually positive in the majority of the tumour cells, is mainly localized to the cytoplasm, occasionally showing a dot-like accentuation pattern, and occasionally highlights the cell membrane (fig 2). Dot-like staining merely reflects Golgi accentuation of cytoplasmic immunolabelling. There does not appear to be any significance associated with this pattern of staining. Acinar cell carcinoma also stains with CD10 but has a luminal surface pattern of staining. Interestingly, CD10 also stains hyaline globules present in the cytoplasm of tumour cells.6 It is thought that reduced CD10 expression may promote cell proliferation as result of an increase of biological modulators, and it has been speculated that reduced/absent CD10 expression in SPT may be a predictor of an adverse clinical. CD10 has also been reported to be focally expressed in the clear cell variant of SPT.5

However, CD10 stains approximately 25% of pancreatic neuroendocrine tumours, a variety of carcinomas, including acinar cell and renal cell carcinomas, and sarcomas. Thus, CD10 is of limited value in small biopsies.
Progesterone and oestrogen receptors
Although there is a distinct female preponderance for SPT, oestrogen receptor-α positivity is very uncommon, and most series report absence of immunoreactivity.8 On the other hand, progesterone receptor positivity is seen in almost all cases of SPT, irrespective of gender (fig 3). Progesterone receptor immunopositivity is seen in the normal pancreatic islets, and approximately 60% of pancreatic neuroendocrine tumours show positivity for this receptor.9 The rationale for progesterone rather than oestrogen receptor activation is not clear but perhaps is linked to wnt pathway abnormalities in particular, nuclear β-catenin. This, in turn leads to target gene abnormalities, especially a cluster of chromosome 11q molecules that are upregulated. These include progesterone receptor, cyclin D1, FLI-1 and CD56.

Neuroendocrine markers
Synaptophysin
Synaptophysin is positive in 70% of cases: more frequently staining individual isolated cells or small clusters of cells rather than showing a diffuse staining pattern which is expected in neuroendocrine tumours (fig 4). If diffuse staining is encountered, then the positive staining is sparsely distributed throughout the tumour.6 Focal synaptophysin immunoexpression is the rule with SPT.

Chromogranin A
Chromogranin A is negative in all cases of SPT.
CD56
CD56 is a neural cell adhesion molecule and member of the immunoglobulin superfamily and is implicated in cell–cell or cell–matrix adhesion during development. It is expressed in both normal and neoplastic cells.
In the human pancreas, CD56 is usually expressed diffusely but weakly in adult islets of Langerhans. With regards to CD56 staining in SPT, it has been reported to be positive in 55.5–100% of cases with variable intensity.6 7 Not only are the predominant epithelioid cells of SPT positive, but multinucleated, foamy tumour cells as well as clear cells also stain for CD56.5 Foamy macrophages (not foamy tumour cells) are negative for CD56 but positive for CD68. CD56 is also positive in malignant SPT, both in the primary tumour and in the metastasis.6 Although CD56 immunoexpression has been reported to be significantly higher in metastatic cases compared with those localised to the pancreas, suggesting that it may serve as a marker for SPT with metastatic potential, a larger number of cases need to be examined to validate this hypothesis.7
CD56 also displays intense immunoreactivity in many neuroendocrine tumours and thus cannot be relied on to separate SPT from neuroendocrine tumours.
Neuron-specific enolase
Neuron-specific enolase is diffusely positive for most cases of SPT. However, it also stains 90% of melanomas, 100% of renal cell carcinomas and pancreatic neuroendocrine tumours, and 50–60% of acinar cell carcinomas.6 10 11 In view of this low specificity, NSE has very little use in the work-up of SPT.
Protein gene product 9.5
SPT shows only scattered positive cells in approximately 40% of cases.
Cytokeratins
AE1/AE3 is positive in up to 75% of the cases, but staining is of a weaker intensity in SPT compared with normal pancreatic epithelium. Sometimes there is an accentuation of staining in the basal portion of the tumour cells. However, results vary with different series, and it is best to regard cytokeratin expression in SPT as inconsistent and unreliable for diagnostic purposes.
CK7 and CK19 are uniformly negative in SPT, and occasional cases are CK8, CK18 and CK20 positive.6
It is worth remembering that AE1/3 may also be expressed in occasional metastatic melanomas.12
Miscellaneous markers
Ca19-9 is a marker specific for ductal epithelia but is only focally expressed in a few examples of SPT.
p53 immunoexpression has been encountered in 16% of cases in a diffuse or patchy distribution.9
Vimentin has been reported to be diffusely expressed in SPT with up to 60% of the tumour population showing positivity.5–7 Fifty to 90% of cases of both melanoma and renal cell carcinomas are also positive for vimentin.10 13
Wnt pathway dysfunction
E-Cadherin and β-catenin are important molecules in the wnt signalling pathway, and both have been shown recently to be of diagnostic value in SPT. Figure 5 illustrates normal β-catenin catabolism (A) and interaction with E-cadherin, while (B) is an illustration of the process with wnt pathway activation. The reason these two proteins warrant separation from all the other markers is that they yield consistent results in 100% of cases of SPT. It is for this reason that they are now regarded as two of the pre-eminent antibodies in the routine panel used to investigate SPT.

β-Catenin
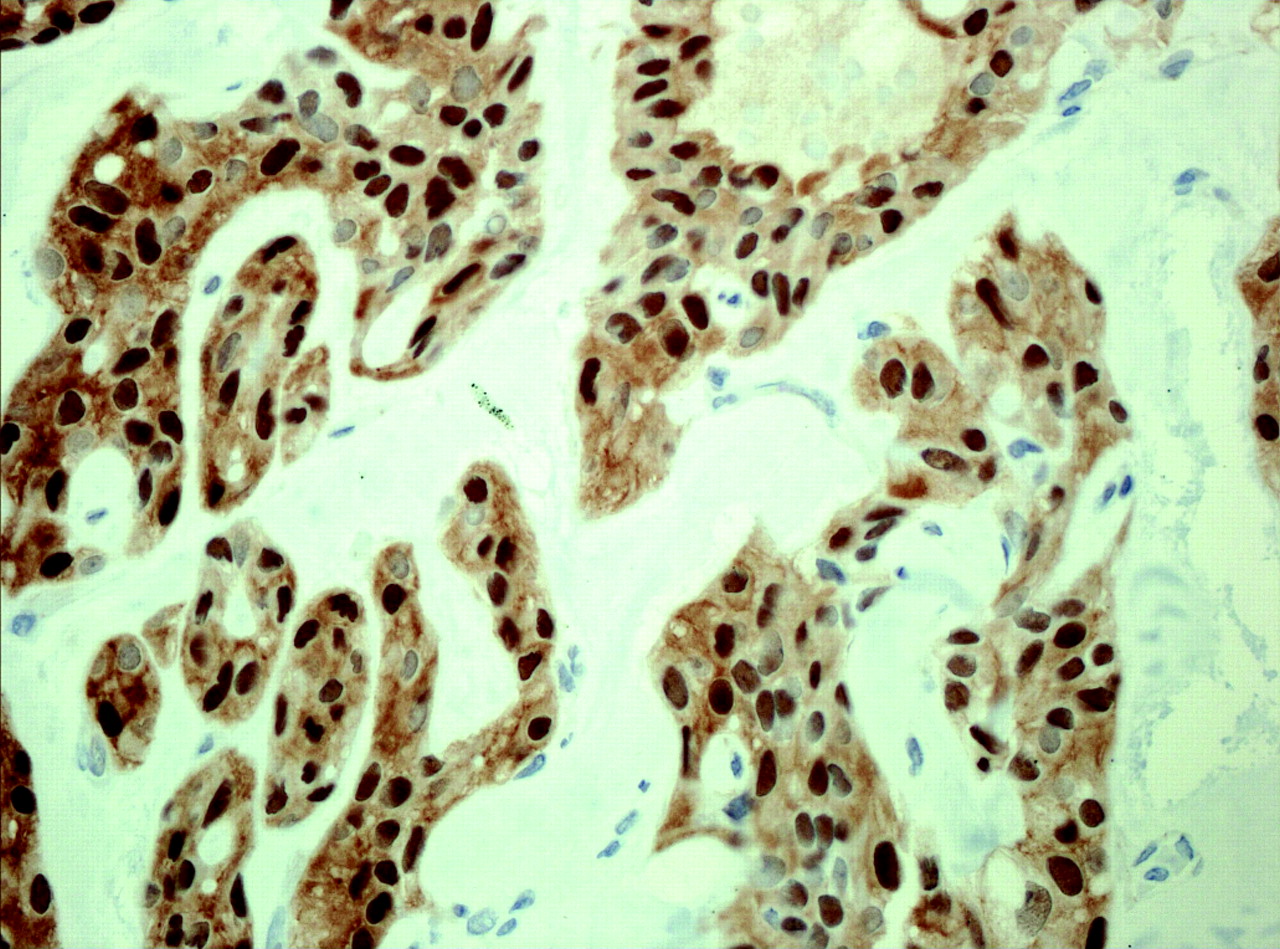
β-Catenin is a component of adherens junction that links E-cadherin to α-catenin. In the Wnt signalling pathway, β-catenin plays a key role as a transcriptional activator in conjunction with lymphoid enhancer factor/T cell factor DNA-binding protein to induce target gene expression resulting in cell proliferation and differentiation.14 Mutations of the components of the Wnt/β-catenin pathway are found in many gastrointestinal cancers. SPT are usually associated with activating mutations in exon 3 of the CTNNB1 gene encoding for β-catenin in 83% of cases, resulting in dysregulation and redistribution of β-catenin protein leading to characteristic strong nuclear and cytoplasmic immunoreactivity in 100% of the cases (fig 6).14–16 This staining pattern contrasts with the normal pancreas, where β-catenin protein shows distinct membrane decoration of the ducts and the acini. The rationale for this aberrant location is because the mutations involve GSK-3β phosphorylation sites and abrogate subsequent ubiquitin-mediated degradation of β-catenin protein, allowing for cytosolic accumulation and pooling of β-catenin with consequent nuclear shift leading to nuclear accumulation (see fig 7, area A)


While activation of the Wnt pathway results in relocation of β-catenin protein, it also results in overexpression of Cyclin D1 and glutamine synthetase.16 Cyclin D1 is variably overexpressed in SPTs from 74% to 100% of the cases and variably from 15% to 100% of the tumour cells.14 16 These antibodies are negative in the surrounding normal pancreas. Glutamine synthetase shows strong cytoplasmic immunostaining in SPT, in contrast to the weak cytoplasmic staining observed in the surrounding normal exocrine and endocrine pancreas.16
Thus, there is a strong correlation between mutations in the β-catenin gene and the resultant aberrant protein expression in SPT. While the vast majority (85–90%) of SPT show exon 3 mutations, 100% of cases show nuclear and cytoplasmic immunoreactivity. In those cases not showing exon 3 mutations, it is likely that mutations are present in other exons that would account for the remaining 10–15% of cases.
Nuclear expression of β-catenin is extremely uncommon in pancreatic neuroendocrine tumours.17
E-Cadherin
E-Cadherin is a calcium-dependent transmembrane glycoprotein, localised to zonula adherens junctions at the basolateral surface in epithelial cells and is involved in cell–cell interaction. Normal E-cadherin expression plays a key role in the maintenance of epithelial integrity and polarity function. The E-cadherin molecule is composed of a cytoplasmic domain, a single-pass transmembrane domain and an extracellular domain that consists of five tandemly repeated cadherin-motifs subdomains with putative calcium-binding sites. The cytoplasmic domain of E-cadherin interacts with the catenin molecules that mediate its binding to the actin cytoskeleton (see fig 8).

E-cadherin binds to either β-catenin or γ-catenin. E-cadherin immunostaining is localised to and highlights the cell membrane of normal cells of pancreatic ducts and acini as well as endocrine cells.
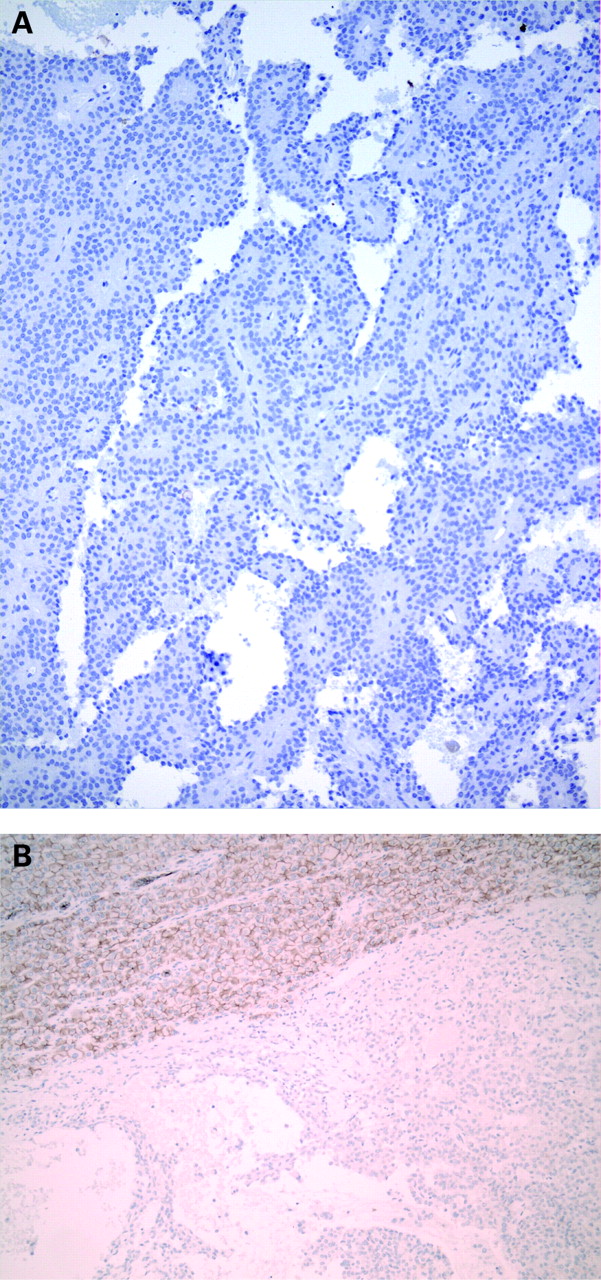
There has been a recent flurry of publications on E-cadherin expression in SPT.7 16 18–21 In addition to some observing loss of membrane expression, others have also noticed very characteristic nuclear positivity for E-cadherin.7 21 Nuclear E-cadherin expression was explored further in another set of tumours (oesophageal squamous carcinomas), and in fractionation studies, a fragment of the E-cadherin molecule was confirmed to be intranuclear in location.22 Further to this, our group showed that the staining pattern for E-cadherin in SPT is dependent on the type of E-cadherin antibody used.19 Use of the antibody that recognises the extracellular domain of the E-cadherin molecule results in an absence of staining in SPT (complete loss membrane staining in all cases) (fig 9A,B), while use of the antibody that recognises the cytoplasmic domain results in nuclear positivity (fig 10).19


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Nuclear immunoreactivity of E-cadherin with loss of membranous staining was found in all cases studied, using an antibody that recognises the intracytoplasmic domain of E-cadherin.19 21 Cytoplasmic immunoreactivity with variable dot-like pattern7 16 or a complete loss of membrane staining and absence of cytoplasmic immunoreactivity was seen using an antibody against the extracellular domain of E-cadherin.19 20 The significance of dot-like E-cadherin cytoplasmic positivity in SPT is not known; however, cases of gastric cancer with some types of CDH1 gene mutations have led to Golgi accentuation of E-cadherin immunohistochemistry.
Approximately 30% of pancreatic neuroendocrine tumours have also been documented as showing nuclear immunoreactivity for E-cadherin using the antibody to the intracytoplasmic domain and loss of membrane staining with the antibody to the extracellular domain.16 Thus, nuclear E-cadherin positivity is not the exclusive preserve of SPT and can be seen in pancreatic neuroendocrine tumours, Merkel cell carcinomas and approximately 50% of clear cell renal cell carcinomas.23 24
Thus, it is important to be aware of the E-cadherin antibody that is employed in the work-up of SPT, as different immunohistochemical results will be obtained.
The rationale for the consistent E-cadherin aberrations is not clear cut. It has been suggested that p120, an E-cadherin regulator, rather than mutations of the CDH1 gene, may be responsible for dysregulation of E-cadherin protein in SPT.25
E-cadherin immunohistochemistry is of diagnostic value in all cases of SPT as all cases will show either nuclear positivity or absence of membrane staining depending on the antibody that is employed.
CONCLUSION
Table 1 summarises the immunohistochemical findings of SPT and its lookalikes.
As can be seen from the discussion, there have been several markers that have been employed in the immunohistochemical work-up of SPT. This brief overview is not intended to be all encompassing but rather to highlight the important antibodies and their immunoreactivity with SPT. It is worth reiterating that most SPT are readily recognised morphologically, but predominantly solid variants, those with a significant clear cell component and needle biopsy material, can all be quite challenging. In the case of metastatic renal cell carcinoma or malignant melanoma, an appropriate clinical history is ideal; however, there are times when this information is not forthcoming. With regards to morphologically diagnostic cases, it is a moot point whether any immunohistochemistry needs to be performed at all. It is perhaps advisable to perform confirmatory immunohistochemistry if these tumours are not encountered frequently, even though the diagnosis of SPT may be obvious. As with most tumours, a panel of markers is advocated, and the results thereof need to be correlated with morphology and clinicoradiological information. It is important to remember that one antibody or marker alone cannot identify SPT; hence a prudent panel of markers is advocated. Although further analysis of the expression of different members of the wnt pathway in renal cell carcinoma is still required, a tumour that is CD10 positive, displays cytoplasmic and nuclear β-catenin immunolabelling, and shows nuclear E-cadherin expression with the antibody to the cytoplasmic domain and loss of membrane staining with the antibody to the extracellular domain is likely to be a SPT.
Take-home points
Solid pseudopapillary tumours (SPT) may show histological overlap with other tumours such as endocrine tumours.
The key immunohistochemical markers in the evaluation of SPT are: CD10, progesterone receptor, synaptophysin, β-catenin and E-cadherin.
β-Catenin staining of 100% of SPT is cytoplasmic and nuclear, and is reflective of mutations in the gene.
E-Cadherin immunostaining is dependent on the type of antibody used: nuclear staining is seen with the antibody to cytoplasmic domain, while complete loss of membrane localisation is encountered with the antibody to the extracellular domain.
The immunoprofile of CD10 +ve, PR +ve, β-catenin cytoplasmic and nuclear +ve, E-cadherin nuclear +ve/membrane loss is virtually diagnostic of SPT.
REFERENCES
Footnotes
Competing interests: None.