Article Text

Abstract
Background: Nestin, an intermediate filament (IF) protein, is expressed in proliferating progenitor cells of developmental and regenerating tissues, and is identified as a neuroepithelial precursor cell marker. Recently, nestin was detected in some neoplasms such as glioma, ependymoma, melanoma, rhabdomyosarcoma, gastrointestinal stromal tumour (GIST), and testicular stromal tumour. Moreover, the expression intensity of nestin exhibited significant correlation with the malignant grade of glioma.
Aims: To detect the expression of nestin in different tumours and to analyse the relationship between the expression of nestin and the malignant grade of the tumours.
Methods: Formalin-fixed and paraffin-embedded surgical samples of neoplastic tissues were obtained from the Department of Pathology of Sun Yat-sen University. Histological analysis and immunohistochemical staining for nestin were performed. Histoscores were analysed by semi-quantitative evaluation.
Results: Nestin was expressed predominantly in the cytoplasm of angiosarcoma, pancreatic adenocarcinoma and GIST samples, and some tumour cells expressed in the nucleus. There was a statistically significant difference between the histoscore of nestin in high malignant GIST (2.2366 (0.6920)) and that in low malignant GIST (1.3783 (0.4268)) (p = 0.003); and also between that in high malignant angiosarcoma (1.9188 (0.2069)) and that in low malignant angiosarcoma (0.6474 (0.3273)) (p = 0.000). Cavernous angioma did not express nestin. The histoscore of nestin in high malignant pancreatic adenocarcinoma (7/14) was 1.1767 (0.4676), and that in low malignant pancreatic adenocarcinoma (3/8) was 0.6577 (0.0056) (no significant difference, p = 0.112).
Conclusions: Results suggest that the expression of nestin may play an important role in the development of some neoplasms such as GIST and angiosarcoma.
Statistics from Altmetric.com
Nestin is almost an acronym for neuroepithelial stem cell protein. It is an intermediate filament (IF) protein expressed in proliferating cells during the developmental stages in a variety of embryonic and fetal tissues. It is also expressed in some adult stem/progenitor cell populations, such as newborn vascular endothelial cell,1–3 striated muscle precursor cell,4 hair follicle precursor cell,5 islet precursor cell,6 and liver oval cell,7 and it is reactivated in response to injuries or other pathological conditions. Nestin may represent the proliferation, migration and multidifferentiated characteristics of multi-lineage progenitor cells.
Recent studies have suggested that cancer might be generated from a cancer stem cell, a tumour-initiating cell that shares many properties with those of stem cells. During tumour genesis, cells of certain tissues show protein profiles of stem/progenitor cells of those tissues. Besides being an important marker of neural stem/progenitor cells, nestin has also been detected in various tumours, such as glioma, ependymoma, melanoma, rhabdomyosarcoma, gastrointestinal stromal tumour (GIST), testicular stromal tumour and adrenocortical tumours.8–15 Nestin may also be a diagnostic and prognostic indicator of the malignant grade of tumours. For example, some studies have shown strong nestin expression in high malignant glioma. Moreover, histoscores of nestin expression in different malignant gliomas have shown statistical differences.16–18 The expression of nestin has also been observed in tumour cells of melanoma, but not in differentiated melanocytes in benign melanocytic nevi.16 Based on these observations, it has been suggested that nestin could be an indicator of tumour malignancy.
In this study, the expression of nestin in various tumours was detected with immunohistochemical staining and the correlation between the nestin expression and the malignant grade was analysed.
METHODS
Tissues
Formalin-fixed and paraffin-embedded surgical samples of neoplastic tissues were obtained from the Department of Pathology of SunYat-sen University (see table 1). The samples examined in this study were fixed in 10% neutral-buffered formalin overnight, dehydrated in gradient alcohol, and put into low melting point paraffin. Continuous 5 μm thick tissue sections were cut and fixed onto silicified slides.
Pathological grading
The histopathology of each sample was studied using H&E staining, and a report was obtained from the Department of Pathology of SunYat-sen University. There was no unified grading standard for GIST. Cases were classified according to risk and their potential for aggressive clinical behaviour based on the NIH consensus statement of 2001 for GISTs.19 Grade I (well differentiation) represents the condition when tumour is <5 cm, and pathological mitotic count is <5/50 high power fields (HPFs). Grade II (moderation differentiation) represents the condition when tumour is <5 cm, and pathological mitotic count is 5–10/50 HPFs; or when tumour is 5–10 cm, and pathological mitotic count is <5/50 HPFs. Grade III (poor differentiation) represents the condition when tumour is >5 cm, and pathological mitotic count is >5/50 HPFs; when tumour is >10 cm, and pathological mitotic count is any quantity/50 HPFs; or when tumour is of any size, and pathological mitotic count is more than 10/50 HPFs. For angiosarcoma, grade I (well differentiated) represents the stage when the pathological mitotic count is <5/10 HPFs; grade II (moderately differentiated) represents the stage when pathological mitotic count is <10/10 HPFs; and grade III (poorly differentiated) represents the stage when pathological mitotic count is >10/10 HPFs.
Nestin immunohistochemistry
Immunohistochemistry was carried out using the streptavidin–peroxidase-conjugated method. Briefly, each tissue section was deparaffinised, rehydrated and then incubated with fresh 3% hydrogen peroxide (H2O2) in methanol for 10 min. After rinsing with phosphate-buffered saline (PBS), antigen retrieval was carried out by microwave treatment in 0.01 M sodium citrate buffer (pH 6.0) at 100°C for 15 min. Next, non-specific binding was blocked with normal goat serum for 15 min at room temperature, followed by incubation with monoclonal mouse anti-human nestin antibody (MAB1259, Chemicon, Temecula, California, USA, final dilution 1:150) diluted in PBS containing 0.2% Triton X-100 and appropriate 2% normal serum (Serva, Heidelberg, Germany) overnight at 4°C. After rinsing with PBS, slides were incubated for 10 min at room temperature with biotin-conjugated secondary antibodies, followed by incubation with streptavidin-conjugated peroxidase working solution for 10 min. Subsequently, sections were stained for 10 min with 3, 3′-diaminobenzidine tetrahydrochloride (DAB), counterstained with Mayer’s haematoxylin, dehydrated, and mounted. Negative controls were prepared by substituting PBS for primary antibody.
H&E staining
The same sections were deparaffinised, and rehydrated with deionised Millipore water. Samples were stained with haematoxylin for 5 min and ablated with 1% hydrochloric acid alcohol for 30 seconds, then immersed in distilled water for 15 min. Slides were stained with 0.5% eosin for 2 min, then dehydrated, immersed in xylene for 15 min, and then mounted.
Double labelled immunofluorescent staining
Sections were deparaffinised and rehydrated with deionised Millipore water, then antigen retrieval was carried out for 25 min. Slides were penetrated in PBS containing 0.2% Triton X-100 for 30 min at room temperature. Non-specific binding was blocked with normal goat serum for 45 min at room temperature. Sections were incubated overnight at 4°C with polyclonal rabbit anti-human von Willebrand factor (VWF, A8802, DAKO, Daco, Denmark, final dilution 1:200) diluted in PBS containing 0.2% Triton X-100 and appropriate 2% normal serum. This was followed by a reaction with goat R-phycoerythrin (R-PE)-conjugated anti-rabbit IgG antibody (Southern Biotech, Birmingham, Alabama, USA, final dilution 1:150) for 45 min at room temperature. The nucleus was counterstained with Hoechst 33342 (Sigma). Next, sections were incubated overnight at 4°C with monoclonal mouse anti-human nestin antibody (MAB 1259, Chemicon, final dilution 1:150). This was followed by goat Cy3-conjugated anti-mouse IgG antibody (Jackson, West Grove, Pennsylvania, USA, final dilution 1:150) for 45 min at room temperature. Subsequently, slides were mounted with 50% buffer glycerol. The cover slips were photographed under the immunofluorescent microscope (TH4-200, Olympus, Tokyo).
Semi-quantitative evaluation of staining
The vast majority of stain was in the cytoplasm, although there was evidence for limited nuclear staining. For this study, only the cytoplasmic staining was scored. The intensity of stain and the different intensity percentages of positive tumour cells were estimated blindly by two investigators with a two-headed microscope at ×400 magnification. The intensity of stain was given a numerical score on a scale of 0–3, with 0 = negative, 1 = light, 2 = moderate, and 3 = intense. The different intensity percentages of positive tumour cells (percentage of the surface area covered) was demonstrated as the ratio of different intense positive tumour cells and total tumour cells. Areas that were negative were given a value of 0. We analysed 10–12 discrete foci in every tissue and generated average stain intensity and the percentage of the surface area covered. The final histoscore was calculated from the sum of (1 × % weakly positive tumour cells) + (2 × % moderately positive tumour cells) + (3 × % intense positive tumour cells). A tissue with intense, uniform stain would be assigned the maximum histoscore of 3, whereas a tissue with light stain intensity (a value of 1) in only 50% of tumour cells (a value of 0.5) would get a histoscore of 0.5.20 21 A tissue with intense stain intensity in 75% of tumour cells, with weak stain intensity in 10% of tumour cells would be assigned a histoscore of 2.35. Assigning a histoscore is a commonly used method for evaluating both stain uniformity and intensity in tissues in order to obtain a better relation of results among various samples from immunohistochemical studies.

Statistical analysis
Statistical analyses were performed with SPSS V.12.0 (Chicago, Illinois, USA). In total, 80 samples from 80 patients (26 women and 54 men) were stained. Mean histoscores from the different malignant tumours (i.e. the mean histoscores of high malignant angiosarcoma and those of low malignant angiosarcoma) were expressed as mean (SEM). Fifty-nine values were included in our statistical evaluation for nestin staining; an independent sample t-test was used to determine the differences in different malignant tumours (i.e. independent sample t-test was used to compare the mean histoscore of high malignant angiosarcoma with that of low malignant hemangiosarcoma). The Kruskal–Wallis test was used to compare group means and the Spearman test was used to test correlations between different variables. Patient was considered a random effect. All p values were based on two-tailed statistical analysis, and p<0.05 was considered significant.
RESULTS
Basic pathological information
In the high malignant GIST group, the average age of the 80 subjects was 52 years (see table 1). In the low malignant GIST group, the average age was 60 years. All GIST samples were CD117 positive and there was a relative lack of desmin and S-100 on immunohistochemical staining. In the high malignant angiosarcoma group, the average age was 59.6 years. In the low malignant angiosarcoma group, the average age was 58.4 years. All angiosarcoma samples were strongly CD31 or CD34 positive on immunohistochemical staining. In the cavernous angioma group, the average age was 39.2 years. In the high malignant pancreatic adenocarcinoma group, the average age was 56.1 years. In the low malignant pancreatic adenocarcinoma group, the average age was 61.1 years old.
Immunohistochemical staining of nestin expression in different malignant angiosarcomas
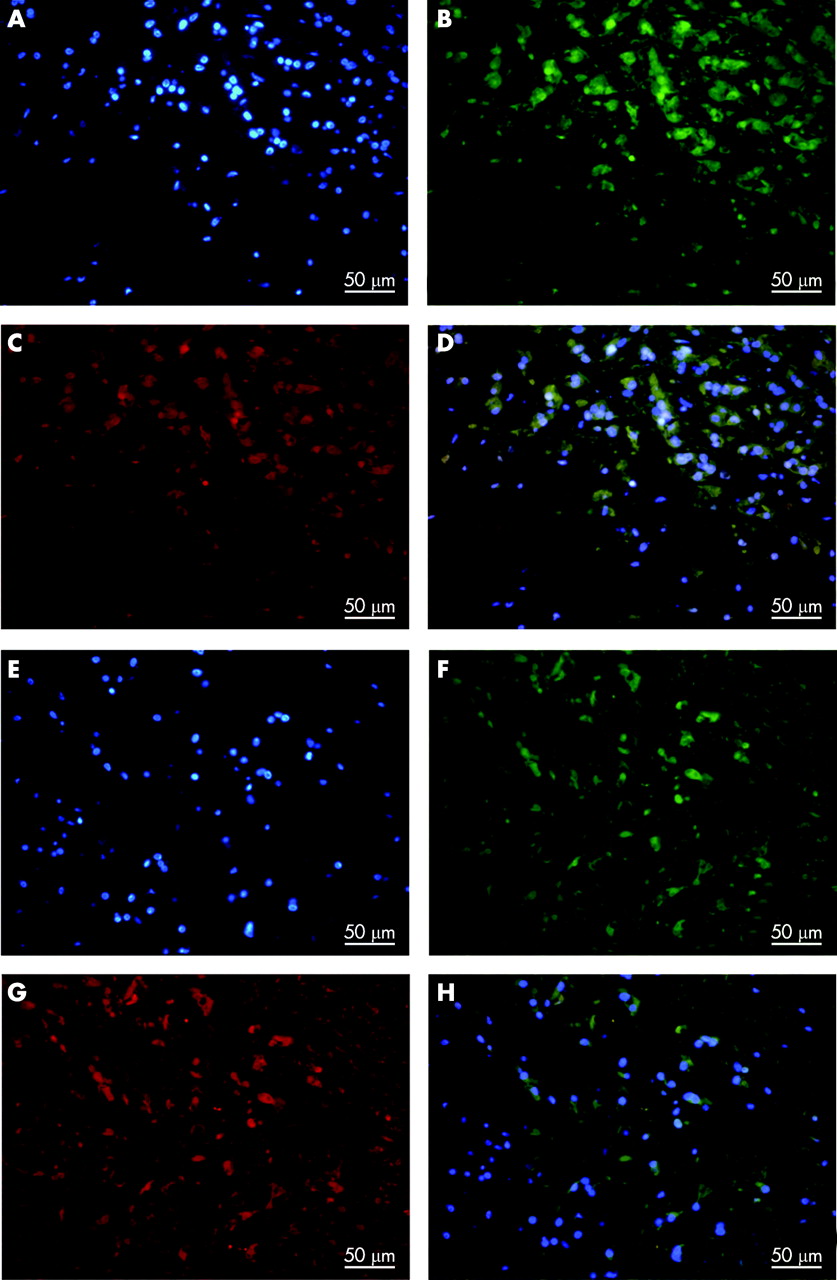
Nestin was expressed in both well and poorly differentiated angiosarcomas (fig 1A–D, fig 4). In poorly differentiated samples, nestin was expressed mostly in the cytoplasm of tumour cells; some tumour cells expressed nestin in the nucleus. Intense and concentrated expression of nestin was located in most tumour area (fig 1A,B); weak expression was located in the restricted tumour area. In well differentiated samples, moderate and diffuse expression of nestin was present in the tumour cells and located in the restricted tumour area (fig 1C,D). In cavernous angioma (fig 1E,F), nestin was only expressed in some newborn vascular endothelial cells, and tumour cells did not express nestin.

Immunohistochemical staining of nestin expression in GISTs
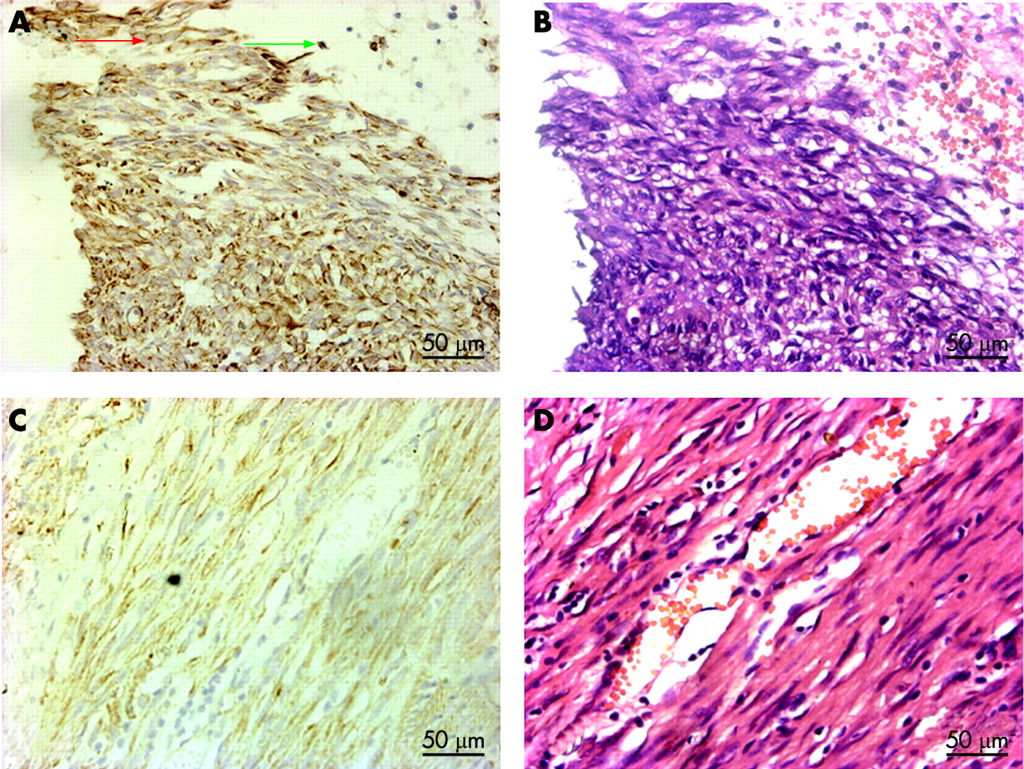
Nestin was expressed in both poorly and well differentiated GISTs (fig 2A–D). In poorly differentiated GISTs, the intense expression of nestin was present in most tumour cells (fig 2A,B). In well differentiated GISTs, the moderate and uniform expression of nestin was located in the tumour area (fig 2C,D).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemical staining of nestin expression in pancreatic adenocarcinomas
Nestin was expressed in poorly or well-differentiated pancreatic adenocarcinoma (Fig.3A, B). Part of tumour cells expressed nestin, and some samples expressed nestin. Poorly differentiated pancreatic adenocarcinoma (7/14, the numerator represents the whole-cytoplasmic staining cases and the denominator represents the total sections examined) expressed nestin and well-differentiated pancreatic adenocarcinoma (3/8) expressed nestin as well. The moderate and uniform expression of nestin was present in different malignant pancreatic adenocarcinomas.
Histoscore
Table 2 shows the expression levels of nestin in different malignant GISTs and angiosarcomas. Nestin expression in low malignant GISTs and angiosarcomas was significantly different to that of high malignant GISTs (p<0.01) and angiosarcoma (p<0.01).
We assessed the expression of nestin according to the intensity and amplitude of expression. In the high malignant angiosarcoma group, about 4000 cells were counted in every case. The expression of nestin was located in about 85% of the tumour area and moderate to intense whole-cytoplasmic immunostaining was present in the tumour cells. Nestin showed a diverse staining pattern that varied from strong homogeneous positivity in most malignant cells to very focal staining in a small subset of tumour cells. In the low malignant angiosarcoma group, about 3800 cells were counted in every case. The expression of nestin was located in about 20% of the tumour area and showed very focal staining in a small subset of tumour cells in 15 cases. There was a significant difference (p<0.01) between the histoscore of nestin in the grade III angiosarcoma group and that in the grade I angiosarcoma group. Cavernous angioma did not express nestin, but some newborn vascular endothelial cells expressed nestin. In low malignant GISTs, about 2642 cells were counted in every case; the expression of nestin was located in about 50% of tumour area. In high malignant GIST, about 3732 cells were counted in every case; nestin was expressed in more than 83% of tumour area. There was a significant difference between the histoscore of nestin in the grade III GIST group and that in the grade I GIST group (p<0.01). In high malignant pancreatic adenocarcinoma, about 2298 cells were counted in every case. The expression of nestin was located in about 40% of tumour area. In low malignant pancreatic adenocarcinoma, about 1300 cells were counted in every case; the expression of nestin was located in 23% of tumour area. Moderate to intense whole cytoplasmic immunostaining was present in the tumour cells in different malignant pancreatic adenocarcinomas. The histoscore of nestin expression in high malignant pancreatic adenocarcinoma (7/14) was 1.1767 (0.4676), and that in low malignant pancreatic adenocarcinoma (3/8) was 0.6577 (0.0056) (difference not significant).
DISCUSSION
Nestin is expressed in neuroepithelial precursor cells.22–25 Ehrmann discovered that among nervous system tumours, the expression of nestin in glioma and ependymoma was positively correlated with the malignancy of the tumours. Interestingly, in the present experiment, we found that nestin was only expressed in newborn vascular endothelial cells within the cavernous angioma tissue, not in tumour cells. In different malignant angiosarcomas, tumour cells expressed nestin. The histoscore of nestin in poorly differentiated angiosarcoma was higher than that in well-differentiated angiosarcoma. This may be because vascular endothelial cells in cavernous angioma were in the completely differentiated state, and nestin was replaced by mature IF protein. Angiosarcoma was malignant vascular endothelial cell tumour, where these vascular endothelial cells were in the incompletely differentiated state, so nestin was not replaced by mature IF protein. Based on the fact that nestin was expressed in newborn vascular endothelial cells and angiosarcoma cells,26 27 it was assumed that some angiosarcoma cells shared the same IF protein (nestin) with endothelial precursor cells. It is possible that these tumour cells were derived from normal vascular endothelial precursor cells stimulated repeatedly by tumour genesis factor, and hence they displayed some similar properties with normal vascular endothelial precursor cells: hence nestin began to re-express. Angiosarcoma cells in the poorly differentiated state were at a more primitive and immature stage than those in the well differentiated state, so there were more pathological mitoses; proliferation in the poorly differentiated state was more productive than that in the well differentiated state. IF protein, such as nestin or vimentin, played an important role in cell division, proliferation and migration through participating in cytoplasmic transport and matter partition. Klein et al showed that IF protein seemed to correlate with the high proliferative and migrational activity of primitive neuroectodermal tumours of the CNS and metastatic melanoma, suggesting that nestin might participate in proliferation and invasion of angiosarcoma cells; the expression of nestin was more intense in poorly differentiated angiosarcoma than in well differentiated angiosarcoma.16 28
GIST is a malignant mesenchymal neoplasm. There is controversy over its histogenetic origin; it has immunohistochemical and ultra-structural resemblance to the interstitial cells of Cajal. The designation of these tumours has largely been based on the immunohistochemical expression of c-KIT (CD117; stem cell factor) and CD34, with a relative lack of desmin and S-100 immunoreactivity. Nestin was expressed in both well and poorly differentiated GISTs. The expression of nestin was more intense in the poorly differentiated state than in the well differentiated state. It may be that because tumour cells in poorly differentiated GIST were further dedifferentiated, proliferation of cells was quicker. There was no significant difference of expression of nestin in the different malignant pancreatic adenocarcinomas in this study; this requires further investigation.
What roles does nestin play in different malignant grade tumours? As one type of intermediate filament, is the expression of nestin related to malignant proliferation of other tumour cells? What effect does lack of expression of nestin have on some tumour cells expressing nestin? Further investigation into the function of nestin is required.
Take-home messages
Nestin expression was found not only in neuroepithelial stem cells, but also in newly vascular endothelial cells, and some tumours, such as glioma, melanoma and gastrointestinal stromal tumour (GIST). The expression intensity of nestin exhibited significant correlation with the malignant grade of glioma.
Different malignant angiosarcomas also expressed nestin. The expression intensity of nestin exhibited significant correlation with the malignant grade of angiosarcoma. Cavernous angioma did not express nestin. The expression of nestin in GIST may be correlated with the malignancy.
Histoscore analysis as semi-quantitative evaluation of staining is an established scoring method in clinical oncology to gauge both stain intensity and uniformity for valuating nestin expression.
Acknowledgments
We thank Shao Chunkui (Pathological Department, the third affiliated hospital of SunYat-sen University,) and Wang Liantang (Pathological Department, the first affiliated hospital of SunYat-sen University) for providing samples and technical guidance.
REFERENCES
Footnotes
Funding: This work was supported by the National Basic Research Program of China (973 Program), No. 2001CB509904; the Key Scientific and Technological Projects of Guangdong Province, No. 2003A3020103, 2005A30201001; the Key Scientific and Technological Projects of Guangzhou City, No. 2002U13E0011; and the National Natural Science Foundation of China, No. 30571891, 30671023.
Competing interests: None declared.