Article Text

Abstract
The introduction of global gene expression analysis in breast cancer research has focused attention onto a repeatedly described subgroup of invasive breast cancer, the basal-like carcinomas. This subgroup is characterised by the expression of high-molecular weight cytokeratins 5, 14 and 17; using immunohistochemical diagnosis, it represents approximately 7–20% of invasive breast cancers. Some of these tumours fulfil the criteria of grade 3 invasive ductal carcinoma, the so-called triple negative carcinomas. However, other rare subgroups of metaplastic, medullary and myoepithelial carcinomas also belong to this entity. Even though the initial clinical prognostic relevance of basal-like breast cancers may have been overestimated, its distinctive biology generates many questions regarding the pathogenesis, chemosensitivity and optimal clinical management of this subgroup. Physiological progenitor cells within the normal female breast share essential immunohistochemical features with basal-like breast cancers. Although the exact relationship between subgroups of normal breast cells and their respective malignant counterparts is still under investigation, the major hallmarks of physiological progenitor cells are either maintained or reactivated by distinct genetic changes in basal breast cancer cells. This review will discuss the impact of these findings on our global understanding of breast cancer pathogenesis, especially from the perspective of its potential histogenesis. Clinical consequences and potential future research directions driven by the definition of basal breast cancers will also be discussed.
Statistics from Altmetric.com
CLASSIFICATION OF BREAST CANCER ACCORDING TO GENOTYPE AND IMMUNOPHENOTYPE
The classification of invasive breast cancer for surgical, prognostic and predictive purposes is part of the basic workup of every breast cancer specimen, and usually involves molecular and immunohistochemical assays.1 These conventional, mainly morphology-based approaches have been clinically validated and serve as the gold-standard for prognosticating patient outcome. Other molecular markers, such as the oestrogen receptor (ER), progesterone receptor (PR), and expression of the growth factor receptor HER2, provide therapeutic predictive value, and are of central importance for the clinical management of breast cancer. However, many other genes have limited clinical value, and the subclassification of breast cancers based on the expression of these single genes offers incomplete prognostic and predictive information. Thus, investigators are continually searching for new breast cancer biomarkers, especially those that predict therapeutic efficacy of conventional and molecular-based chemotherapeutic treatments.
Novel classification systems based on the definition of cytogenetic alteration patterns have given rise to the postulation of multiple, parallel pathogenetic pathways in breast cancer.2 3 For example, the distribution of 16q-losses in different grades of breast cancers shows that invasive breast cancer is comprised of multiple distinct subgroups that do not necessarily arise from sequential genetic and morphological dedifferentiation steps.4 Global gene expression profiling using microarray analysis extended our current knowledge and promises to further improve predictive and prognostic power in breast cancer pathology. Gene expression studies have used different microarray platforms to address slightly different questions. One research approach used supervised classification techniques to define gene sets for prognostic purposes, identifying genes that were differentially expressed in patients who, within a finite period of time, did and did not develop metastatic disease (e.g. “prognostic 70-gene set”5 6). Others used different methods to determine gene signatures that would classify breast cancers into distinct molecular subtypes (the Stanford/Norway “intrinsic” gene set7–9). The first approach was further refined by associating the “prognostic 70-gene set” with a “core serum response” gene set—considered representative of wound healing processes—to generate a better predictor of clinical outcome in patients with earlier stage breast cancer.10 Classification of breast cancer using the “intrinsic” gene set defined by Perou and colleagues has stimulated recent intense interest in the pathophysiology and best treatments for diverse tumour subtypes. However, it has also generated confusion regarding appropriate subtype nomenclature.
Two decades ago, Dairkee et al described a small subgroup of breast cancers that, similar to cells from normal basal epithelium, exclusively expressed a high molecular weight basal cytokeratin, and that had poor prognostic characteristics, postulating that these cancers may originate in “basally located precursor cells often referred to as ‘stem cells’ and may represent tumours of the undifferentiated stem cell”.11 A more recent study12 analysed a group of 295 breast cancers using five diverse gene expression signature sets, including classification gene sets and prognostic gene sets; despite each signature set containing different genes, there was good concordance of patient-specific outcome predictions for the majority of the breast cancer patients. In other words, individual tumours appear to have a good or bad prognostic phenotype, regardless of the gene set used to define that phenotype. This means that multiple feature patterns can define and distinguish specific tumour subtypes, but no one pattern can adequately explain the causal development of the different phenotypes.
BASAL BREAST CANCER
Basal cytokeratins (Ck) represent a large number of high-molecular weight (HMW) cytokeratins which, according to the catalogue of human cytokeratin expression, are mainly seen in the basal cell layers of stratified epithelium.13 In the human breast, these cytokeratins are also expressed in the basally-located myoepithelial cell layer and in a small proportion of luminal, glandular cells.14 The dual meaning of the term “basal” in the breast induced confusion, as “basalness” was often interpreted as a sign of a myoepithelial origin.15 However, as shown below and discussed previously, this explanation might not be sufficient.16
A subgroup of invasive breast cancers expressing basal cytokeratins was first described in 1987 and 1996.17 18 More recent studies have shown that the incidence among Caucasian women ranges around 16%, with significant differences among different ethnic subgroups.19 Further studies gave additional insights into the characteristics of this tumour subgroup, such as expression of hyperproliferation-associated cytokeratins and the coexpression of basement membrane material in these tumours.20 21 Prior to the description of basal carcinomas by microarray technology, studies pointed to clinical and morphological characteristics,22 including the presence of brain metastasis.23 However, this tumour group, defined by the expression of Ck 5, 14 or 17 is rather heterogeneous.24 Recent work studying Ck 5 expression showed that this group is comprised of not only grade 3 invasive ductal carcinomas (NOS), but also other histological breast cancer subgroups, such as metaplastic25 and medullary carcinomas,26 with or without associated BRCA1 mutations.27 It is noteworthy that the vast majority of these tumours always coexpress a multitude of other cytokeratins.28
These tumours also show specific genetic features. In contrast to all other breast cancer subgroups, these tumours, especially the metaplastic subgroup, harbour EGFR-amplifications,29 otherwise rarely seen in breast cancer.30 31 A more recent study characterised an increased expression of genes located on 6p21 and 12p13 as hallmarks of medullary carcinomas.32 A significant proportion of basal carcinomas are associated with a BRCA1 germ line mutation27 33 or sporadic p53-mutations and/or p53-protein overexpression. Compared with Ck 5/14 negative breast cancers, a significantly lower rate of 16q-losses has been described.34–37 However, this significance vanished if the same comparison was made with invasive ductal grade 3 carcinomas only.38
In general, the initially described prognostic relevance has now been challenged by various other reports. Although some initial studies evaluated prognosis without consideration of tumour grade, it has since been shown that the prognostic significance of the basal subtype disappears when evaluated alongside other high risk variables in a representative series of breast cancer patients,39 in ER-negative,40 and in grade 3 breast cancers.41 Moreover, a subgroup of basal carcinomas has been associated with an improved prognosis.42 More recent gene expression analysis also revealed that a prognostic difference could not be elaborated between the basal and the ER negative/HER2-overexpressing breast cancer subgroups.12 However, the criteria used to define basal breast cancer, as shown below, differ significantly and many accumulated results have this potential bias when compared. Another significant source of bias is that most studies grouped patients together who were undergoing different treatment protocols, again cautioning us not to over-interpret these results. To answer future questions about prognosis and appropriate therapies, controlled prospective clinical trials with uniformly treated patients are mandatory.
MORPHOLOGICAL AND IMMUNOHISTOCHEMICAL CHARACTERISATION OF BASAL BREAST CANCER
Morphologically, basal carcinomas are mainly grade 3 invasive ductal carcinomas and share a multitude of features definable by simple H&E staining. Tsuda et al were among the first to describe the presence of large, central acellular necrosis as a major hallmark of basal breast cancer.23 This was later verified by other groups, who further outlined the presence of central scars and a large degree of peritumoural lymphocytosis, as well as high proliferation rate, presence of spindle cells, and squamous metaplasia.43 44
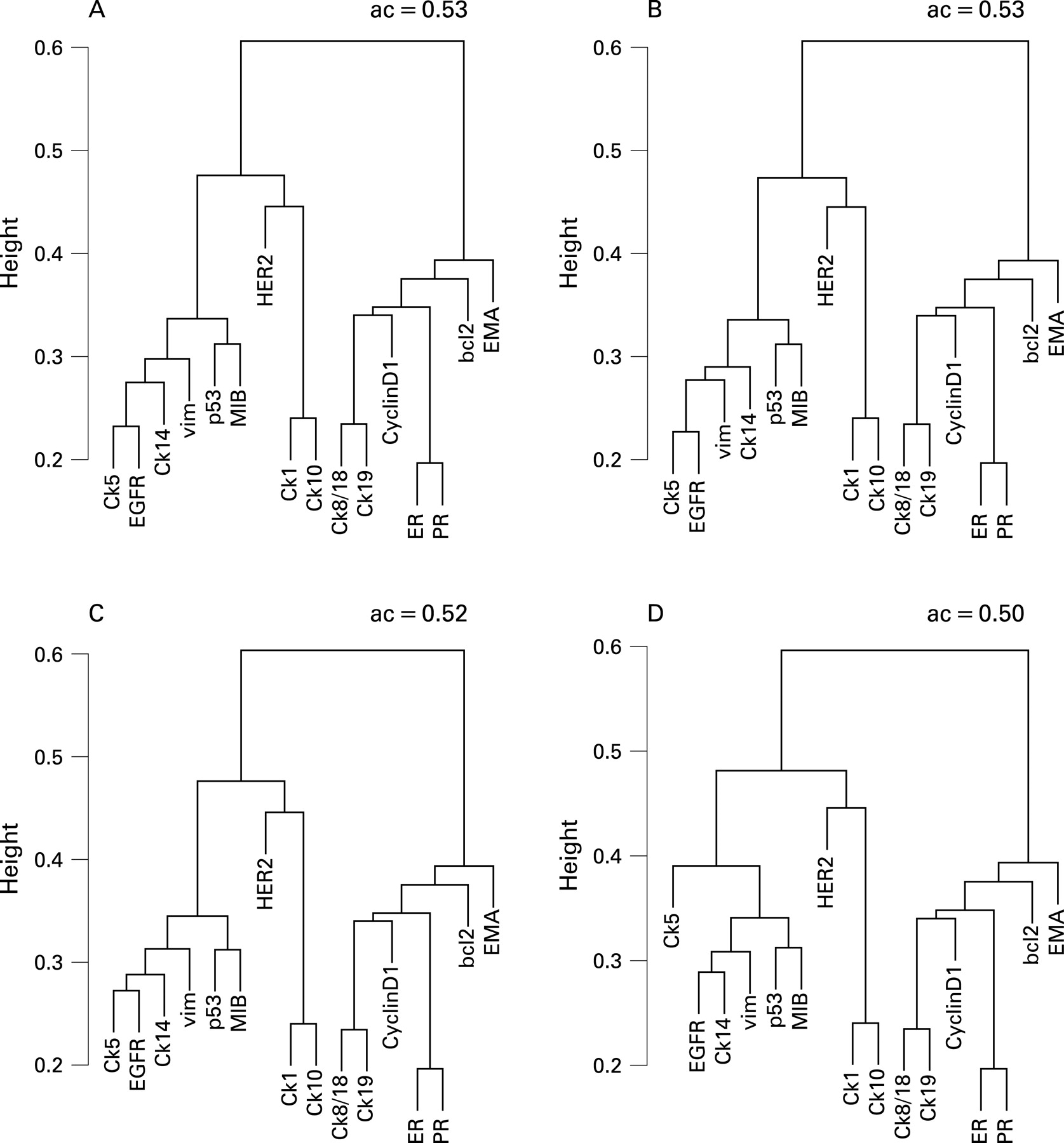
However, there are no currently accepted definitions of “basalness” that use thresholds for distinct HMW-cytokeratins (Ck 5, 14 or 17). This might be partially due to the use of tissue microarrays in many studies, rather than whole tumour tissue sections for immunohistochemical evaluation. Thus, breast carcinomas have been deemed basal when they express HMW-cytokeratin in a single, malignant cell, or in 1%, 5% or 10% of malignant cells (table 1). In addition, one study defined a 50% threshold for the distinction between basal and basoluminal carcinomas, with the former characterised by the general lack of c-erbB2 (HER2/neu) amplifications.39 Despite this general lack of agreement on what defines histological and immunostain “basalness”, further immunohistochemical characterisation displayed very similar results in multiple studies. Basal carcinomas have been consistently associated with expression of epidermal growth factor receptor (EGFR),34 35 44 45 c-kit, p53, p63, negativity of ER and PR, and, in the initial reports, with lack of HER2-expression.46 However, recently the so-called basoluminal carcinomas have been characterised by the expression of Ck 5 and HER2.39 Further investigations revealed the coexpression of smooth muscle actin (SMA), CD10 and vimentin in some tumours,47 as well as the expression of P-cadherin.48 Therefore, even the expression of high molecular cytokeratin in single breast cancer cell might be interpreted as a hint for the presence of a global immunohistochemical expression pattern in the whole tumour. One might therefore argue that “basalness” from an immunohistochemical perspective may be considered an overall tumour cell expression programme, not necessarily defined by the expression of high molecular cytokeratins in the majority of tumour cells. Our own data presented in fig 1 support this assumption: identical gene expression clusters on the protein level could be reproduced irrespective of the set threshold. However, to compare immunohistochemical results with global gene expression profiles requires a direct comparison of both methods within the same tumours.44 49
Basal breast cancer requires a set of diagnostic markers, and has been defined differently in different studies. Whereas Nielsen et al defined basal breast cancer as negative for ER and HER2 as well as positive for basal cytokeratins, EGFR and/or c-kit,45 other groups used the combination of negativity for ER and HER2 with positivity for Ck 5, P-cadherin and p63,50 or positivity for vimentin, EGFR and Ck 5/6.44 It may be that, table 1 shows, these different technical approaches in combination with widely differing patient cohorts might explain aspects of the widely differing experimental results for the mentioned markers. Rakha et al showed, in a multivariate analysis, a relationship between the expression of basal cytokeratins and poor prognosis. Interestingly, the addition of other markers as described above did not increase the detection rate of cases with differing outcome compared with the use of basal cytokeratins alone.51
BASAL CYTOKERATINS, PHYSIOLOGICAL BREAST PROGENITOR CELLS AND GENETIC ALTERATIONS
In recent years, basal cytokeratins have been the focus of breast cancer research from another perspective. In 1988, Jarrasch et al discussed the possible existence of Ck 5 positive cells as potential progenitor cells in the female breast that could give rise to the glandular and myoepithelial cell lineage.52 However, the data from that time were indirect and derived from simple immunohistochemical experiments. Almost a decade later, studies showed that cells with the potential to differentiate into luminal and myoepithelial cells—one requirement for the definition of progenitor or stem cells—express basal cytokeratins.53 Most of these studies were based on mouse or immortalised human mammary cell models.54 Recently, it has also been shown that putative mammary stem cells in the mouse typically show the expression of high molecular cytokeratins and weak or almost absent expression of Ck 18 as well as lack of expression for ER. Furthermore, these cells were EGFR-positive and HER2-negative.55 Interestingly, identical results concerning cytokeratin expression patterns were obtained by Dontu et al, who also noted a high proliferation potential of Ck 5+, Ck 8/18−, ER− cells within primary mammospheres.56 The differentiation of these cells into differentiated glandular cells was paralleled by a complete phenotypic change of these cells into Ck 5−, Ck 8/18+, ER+ cells, again in almost complete concordance to the mouse model.57 Moreover, in most of these experiments these cells seemed to depend on an intact EGF/EGFR system.54 Further characterisations also showed positivity for vimentin and P-cadherin and reduced expression of p21 and p27 in these progenitor/stem cells.58
The similarities of these protein expression patterns in physiological progenitor cells of the breast and the basal breast cancer subgroup are striking. As fig 2 shows, the present state of knowledge defines a spectrum of physiological cellular compartments within the female breast. The extreme ends of this spectrum (progenitor/stem cells and luminal cells) can easily be defined by a variety of proteins. In parallel, the distribution of these protein expression patterns is similar in the spectrum of invasive breast cancer.

This spectrum is not only defined by different protein expression patterns but also by the presence of distinct (cyto)genetic alteration patterns. Whereas basal carcinomas have been defined by the presence of EGFR-amplifications,29 loss of BRCA159 and/or p53-mutations,9 chromosomal 16q-losses were rare in these tumours.36 This was in contrast to ER-positive tumours, with 16q-losses60 as a hallmark.
These associations suggest at least two explanations. Against the background of the above mentioned subsets of progenitor cells, it may be that distinct cytogenetic alterations can show their effect only in distinct precursor cells. 16q-losses in this regard may predominantly occur in more mature progenitor cells, whereas “basal” changes may arise in early, more stem cell-like, progenitor cells. In other words, the tumour would reflect or maintain cellular properties of its progenitor or more differentiated cell of origin (fig 3A). An alternative explanation, taking into account the ongoing discussion about organ-specific stem cells as target cells,61 would instead point towards direct changes in the stem cell itself and, as a result, protein expression patterns in the tumour that reflect specific genetic alterations in the progression from stem cell to tumour cell. This would then suggest that, for example, EGFR-amplifications or the loss of BRCA162 would start a “basal” expression programme, whereas in contrast 16q-losses would lead to the expression of luminal markers as shown in fig 3B and recently shown by microarray analysis.37

{kind=link}
{kind=link}
{kind=link}
Alternative theories speculate about a myoepithelial origin of these tumours, as many “basal” markers are also expressed by myoepithelial cells in vitro or in vivo.47 63 Another proposed origin of basal tumours has been deduced from morphological and immunohistochemical dedifferentiation, defined as “epithelial-mesenchymal transition” (EMT), with the expression of vimentin as a major morphological hallmark of EMT.64 Even though all above listed theories have their shortcomings, the EMT and myoepithelial theories are flawed by some pure histopathological observations. Ductal carcinoma in situ (DCIS) is accepted as the ultimate precursor of invasive breast cancer; it is seen in the majority of basal breast cancer cases.43 As long as no evidence exists that myoepithelial cells are the cells of origin of DCIS, the presence of DCIS, associated with the immunohistochemical staining pattern, including the expression of vimentin,35 suggests a glandular, non-myoepithelial origin of these tumours (excluding the myoepithelial carcinomas). Moreover, an association of benign, myoepithelial tumours with the most common basal breast cancers has not been described to date. More recently a subgroup of DCIS with expression of HMW-cytokeratins has been described, pointing to the existence of a real precursor lesion for basal breast cancer.65 66 EMT as a general mechanism is also disputable, based on the fact that vimentin, considered the most reliable marker of EMT, is expressed in similar degrees in DCIS and the adjacent invasive carcinomas—pointing to a general characteristic of the respective, individual tumour.
However, most of these results are associative and a definite proof would require experiments targeting different subgroups of physiological progenitor cells as has been previously done.67 68 A mouse model of the basal breast cancer subgroup has been recently described.69 However, most studies focus on the basal, progenitor compartment as cellular targets in oncogenesis. Experiments targeting Ck 18+/Ck 5/14− cells have yet to be performed.
CLINICAL CONSEQUENCES
What are the current clinical consequences of our knowledge about basal breast cancers? As mentioned above, the initial overall prognostic significance of basal carcinoma is now discussed intensively.70 However, from a practical point of view it seems that the existing guidelines for the workup of a breast cancer specimen with the determination of the ER, PR and HER2-expression status provides a suboptimal definition of basal tumours. The recently introduced term “triple-negative breast cancer” (ER negative, PR negative, HER2 negative) roughly describes the majority of basal breast cancers; however, the overlap between basal and triple negative breast cancer is imperfect, with basal cancers comprising perhaps 60–90% of triple negative breast cancers, depending on whether they are defined immunohistochemically or by expression profiling; also, basal tumours may themselves be molecularly heterogeneous.49 71 The terms, although occasionally used interchangeably, should be considered distinct for research and clinical purposes as not all basal cancers are triple negative. Therefore, results from future studies focused on triple negative breast cancers will not provide a clear characterisation for all basal breast cancers. However, keeping these discrepancies in mind, preliminary studies on triple negative breast cancers showed that their locoregional relapse rate is identical to that of other molecular subgroups, suggesting that conservative surgical treatment options are still available to patients with basal tumours.72 However, one has to be aware that the basal subgroup is more frequently detected in interval breast cancers compared to screening-detected breast cancers.73 In vitro studies suggested different mechanisms of chemoresistance in basal and luminal breast carcinomas,74 even though the relation between an increased sensitivity and a poorer outcome cannot yet be explained.75 It has also been hypothesised that platinum salts based therapy regimens might be of advantage in the treatment of basal breast cancer as they seem to interfere with the BRCA-1 pathway.76 However, currently no specific systemic therapy is recommended for the treatment of triple negative/basal breast cancers and only limited data is available to support the selection of appropriate treatment.77 Data about chemosensitivity in p53-mutated breast cancers is controversial. In a prospective study, a complete pathological response to primary chemotherapy was reported in 45% of basal breast cancers and 45% of HER2-positive breast cancers, but only 6% of luminal breast cancers.78 Current recommendations regarding adjuvant chemotherapy for this tumour type are in flux and an interdisciplinary approach for individualisation of patient care remains the best approach.
In conclusion, from lessons learned from hereditary breast cancer, an improved understanding of less common tumour types is mandatory to advance our general understanding of breast carcinogenesis and clinical treatment and to finally solve the breast cancer puzzle.
Take-home messages
Basal breast carcinomas are characterised by specific morphological, immunohistochemical and genetic features. However, there is no accepted consensus about the definition of basal breast cancers based on immunohistochemistry.
Basal breast cancers are usually ER, PR and HER2 negative. However they are not identical to the so-called triple negative breast cancers, since the overlap between both terms is not complete. Therefore ongoing clinical studies should incorporate these discrepancies in the interpretation of their results.
Basal breast cancers share a similar protein expression pattern compared to physiological stem/progenitor cells in the breast. Further investigation of basal tumours should enable penetrating insights into the relationship between breast cancer cells and their putative progenitor cells or cell of origin, respectively.
REFERENCES
Footnotes
Competing interests: None declared.