Article Text

Abstract
Women with hereditary non-polyposis colorectal cancer (HNPCC)/Lynch syndrome have a high risk for endometrial cancer (EC) and frequently present with a gynaecological cancer as their first or sentinel malignancy. Identification of these patients is important given their personal and family risk for synchronous and metachronous tumours. Modalities to detect ECs for the possibility of HNPCC include microsatellite instability assay, immunohistochemistry for DNA mismatch repair proteins, MLH1 promoter hypermethylation assay and mutational analysis of DNA mismatch repair genes. The revised Bethesda guidelines provide screening criteria for HNPCC in colorectal cancers (CRCs). However, there are currently no such screening recommendations for women with endometrial carcinoma. While age and family history are useful screening criteria, their sensitivity has been shown to be low for detection of HNPCC in EC. Expansion of these criteria to include tumour morphology (presence of tumour infiltrating lymphocytes and tumour heterogeneity including dedifferentiated/undifferentiated ECs) and topography (lower uterine segment localisation) as well as presence of synchronous ovarian clear cell carcinomas may significantly enhance the detection of patients with EC at risk for HNPCC. Consideration should be given to incorporating these screening criteria into a revision of the Bethesda guidelines for detecting EC patients at highest risk for HNPCC.
Statistics from Altmetric.com
Take-home messages
The association between endometrial carcinoma and hereditary non-polyposis colorectal cancer (HNPCC)/Lynch syndrome is important and should be recognised.
Immunohistochemistry for DNA mismatch repair proteins is an effective method to detect microsatellite instability.
Screening endometrial carcinomas for the possibility of HNPCC using age and personal/family history, while useful, may lead to under-detection of these patients.
Tumour morphology and topography may be helpful additional features to enhance detection of microsatellite instability in endometrial cancer.
Lynch syndrome, or hereditary non-polyposis colorectal cancer (HNPCC), is an autosomal dominant syndrome that predisposes its carriers to multiple malignancies including colorectal cancer (CRC), endometrial cancer (EC), ovarian cancer (OC), and cancer of the renal pelvis and ureter, stomach, pancreas, small bowel and brain.1 Traditionally Lynch syndrome has been perceived as a CRC dominated syndrome. However, in women with Lynch syndrome, the incidence of EC equals or exceeds that of CRC2 and in more than 50% of cases, these women present with a gynaecological cancer as their first or “sentinel” malignancy.3 The frequency of germline DNA mismatch repair gene mutations among unselected patients with EC has been found to be 1.8%4 to 2.1%,5 which is similar to the frequency of Lynch syndrome in colorectal carcinoma.6 In patients younger than 50 years, the incidence is increased up to 9%.7 8
The identification of these patients is important for several reasons. Affected patients are at risk for multiple synchronous and metachronous tumours.2 The risk for developing a metachronous cancer is approximately 25% at 10 years and 50% at 15 years following the initial diagnosis of malignancy.9 These individuals would therefore benefit from surveillance measures to detect other HNPCC associated tumours; their family members may benefit from genetic testing to determine carrier status. Moreover, there may be significance regarding the therapy and prognosis of HNPCC-associated EC as has been observed for CRC.
The revised Bethesda guidelines for identification of individuals at risk for HNPCC and recommended criteria for mismatch repair defect (MMR) testing focus almost exclusively on CRC10 (box 1).
Box 1 The revised Bethesda guidelines for testing colorectal tumours for microsatellite instability (MSI)
Tumours from individuals should be tested for MSI in the following situations:
Colorectal cancer diagnosed in a patient who is less than 50 years of age.
Presence of synchronous, metachronous colorectal or other hereditary non-polyposis colorectal cancer (HNPCC) associated tumours, regardless of age.
Colorectal cancer with the MSI-H histology diagnosed in a patient who is less than 60 years of age.
Colorectal cancer diagnosed in one or more first-degree relatives with an HNPCC-related tumour, with one of the cancers being diagnosed under age 50 years.
Colorectal cancer diagnosed in two or more first- or second-degree relatives with HNPCC-related tumours, regardless of age.
Better surveillance measures have resulted in significantly decreased mortality rates from Lynch syndrome-associated CRC.11 Although several authors have suggested that endometrial cancer be treated equivalently to colorectal cancer in the Bethesda guidelines,12 13 there are currently no published recommendations. Screening measures for the detection of EC and HNPCC include endometrial biopsy and transvaginal ultrasound, but the efficacy is currently uncertain14 and the target populations are poorly defined.
Effective screening is therefore required for the detection of HNPCC in EC, similar to CRC. The importance of screening based on patient age (ie, younger than 50 years) and family history of HNPCC-related malignancies has been proposed,8 but it has been shown that women with HNPCC, particularly those with MSH6 mutations, frequently present with EC at an age greater than 50 years.4 15 In the series by Hampel et al,4 age-based screening would have failed to detect 6 of 10 patients with HNPCC-defining germline mutations and family history-based screening would have missed 7 of 10 patients with HNPCC.
Since it is neither practical nor feasible to analyse all ECs for the possibility of MMR defects, it has become important to identify additional screens or combinations thereof that effectively narrow the pool of patients who need further testing; screening ECs for morphological features associated with MSI is one such modality. Candidate cases can then undergo further testing with one or more assays, with mutational analysis of the DNA-MMR genes being the test that provides genetic confirmation of an HNPCC diagnosis.
This review will detail the contributions of DNA mismatch repair protein expression (DNA-MMR), microsatellite instability assays (MSI), methylation assays to detect hypermethylation of the MLH1 promoter, and mutational analysis of the DNA-MMR genes as they relate to identifying which EC patients are at highest risk of having HNPCC. The ways in which one test complements the others will be explained. We will then propose an algorithm, incorporating clinical history, patient age, tumour morphology and topography, and DNA-MMR immunohistochemistry, which can be used in practice to identify EC patients at risk for HNPCC.
DNA-MMR GENE MUTATION ANALYSIS
Analysis for germline mutation in the DNA-MMR genes (MLH1, MSH2, MSH6 and PMS2) is the confirmatory test for diagnosis of HNPCC/Lynch syndrome. Affected persons carry one mutated gene and acquire an additional abnormality in the second allele within the tumour. Usual mechanisms for the acquired abnormality include a somatic mutation or hypermethylation of the second allele’s promoter. Unlike Lynch syndrome associated CRC, which appears to frequently have mutations in MLH1 and MSH2, ECs have a greater probability of mutations in MSH2 and MSH6. MSH6 mutations appear to confer a particular risk for EC, and these patients tend to present with EC at an older age.15–18 Mutational analysis, however, is expensive, cumbersome and time consuming given the heterogeneity of these mutations.19 Moreover, the requirement for specific patient consent is another drawback as a screening test, especially given the low frequency of anticipated positive results. Therefore pre-selection of high risk patients for mutation analysis is important. This can be achieved by methylation assays to detect hypermethylation of the MLH1 promoter, MSI analysis of tumour DNA by PCR and immunohistochemistry (IHC) for the four DNA-MMR proteins (MLH1, PMS2, MSH2 and MSH6). While the latter two methods do not distinguish between genetic (heritable) and epigenetic (acquired) mechanisms that result in loss of DNA-MMR gene function, each method has its own merits and shortcomings.
MICROSATELLITE INSTABILITY ANALYSIS
The human genome has short tandem DNA repeats, or microsatellites, that are prone to replication errors due to their repetitive nature. Normally, these defects are corrected by the DNA mismatch repair system (DNA-MMR).20 Microsatellite instability results from defects in the DNA-MMR, and occurs in two settings. MSI in most ECs (75%) is sporadic in nature, resulting from methylation (epigenetic inactivation) of MLH1 promoter.21 22 The hereditary form, associated with HNPCC, is a consequence of germline mutations in one, or occasionally more than one, of the DNA-MMR genes (MLH1, PMS2, MSH2 and MSH6). Therefore, MSI is not synonymous with HNPCC, and in fact, HNPCC accounts for only a minority of MSI-high ECs.
MSI analysis is accomplished by PCR using five primers as defined by the international workshop on HNPCC in Bethesda23—two mononucleotide (BAT25 and BAT 26) and three dinucleotide repeats (D2S123, D5S346 and D17S250)—although some authors have suggested that mononucleotide markers may be better for MSI identification.24 Tumours are classified as MSI-high (MSI-H) when two or more of the five markers show MSI, MSI-low (MSI-L) when one of the markers shows MSI, and MS-stable (MSS) if none of the markers show MSI. MSI analysis has some shortcomings when it is used in an effort to detect HNPCC-associated ECs. Many, but not all ECs that arise in the setting of HNPCC are MSI-H, while most, but not all MSI-H ECs arise in a sporadic setting. In other words, MSI analysis may fail to detect a number of HNPCC-associated ECs, while it detects a large percentage of ECs that arise in a sporadic setting.
IMMUNOHISTOCHEMISTRY
DNA-MMR proteins MLH1, MSH2, MSH6 and PMS2 are found to be lacking in tumour cell nuclei by immunohistochemistry in up to one-third of endometrioid adenocarcinomas25–28; this results from MLH1 promoter hypermethylation in most cases while mutations in MLH1, MSH2, MSH6 or PMS2 account for the rest. DNA-MMR protein immunohistochemistry serves as a screen for HNPCC; it is not a diagnostic test.
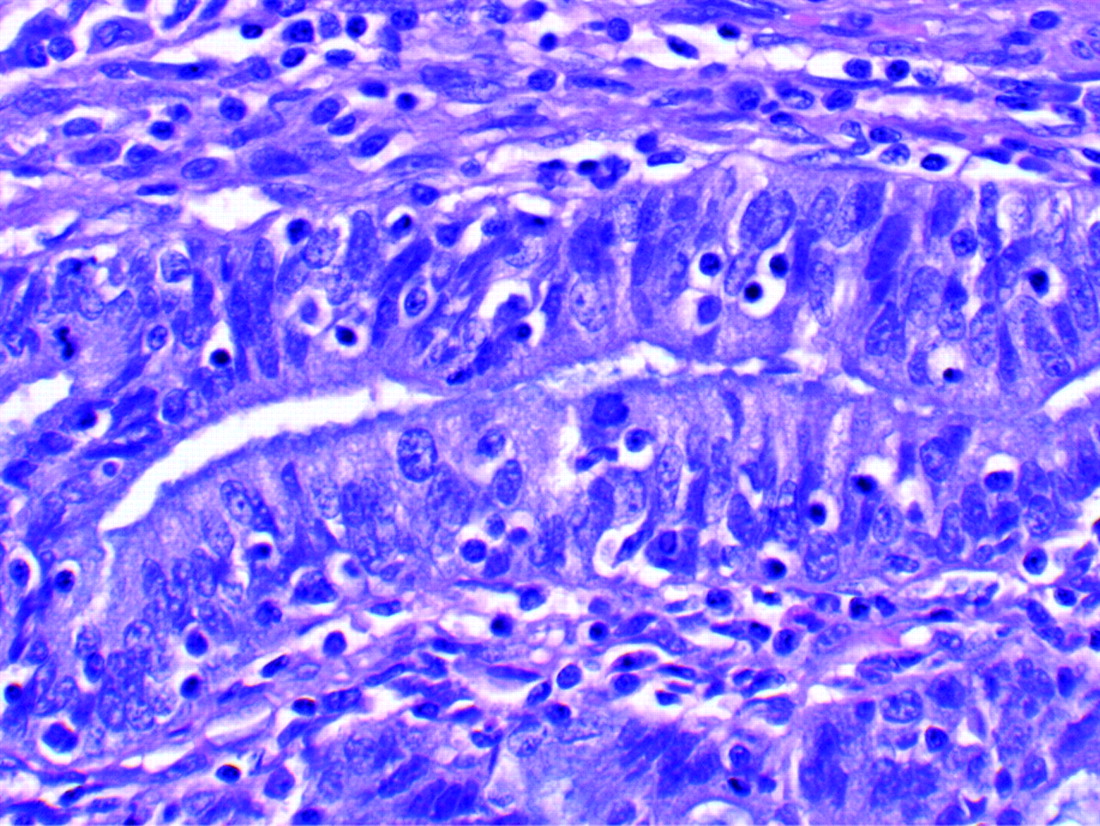
Due to dimerisation of proteins, loss of MLH1 is almost always coupled with concurrent loss of PMS2, and loss of MSH2 is accompanied by MSH6 loss. Isolated loss of MSH6 or PMS2 can occur, however. The interpretation of DNA-MMR IHC can be problematic, particularly with MLH1.19 In general, only complete loss of expression in the setting of a valid positive internal control is considered interpretable (fig 1). Valid internal controls include non-neoplastic endometrial stroma, lymphocytes and glands with reproducibly stained nuclei. Care should be taken to ensure that the lesion being assessed is adenocarcinoma, not hyperplasia.28 Common pitfalls in interpreting these stains are discussed in a review by Shia et al.19 When such problematic cases are encountered, they should be reviewed by at least two pathologists with experience in the interpretation of IHC for DNA-MMR. If no consensus is reached, the stain should be repeated. There are rare cases that remain uninterpretable and are deemed inconclusive. In such cases, an alternative testing mechanism should be performed, if there is clinical suspicion for HNPCC.

This endometrial carcinoma shows loss of nuclear expression of MSH2. The lymphocytes and stromal cells should stain positive and represent an internal positive control.
ASSAYS TO DETECT METHYLATION OF THE MLH1 PROMOTER
Because assays that detect methylation of the MLH1 promoter can recognise epigenetic mechanisms that lead to MSI-H, one can derive information regarding DNA-MMR gene mutation if a methylation assay is performed along with immunohistochemistry for DNA-MMR or an MSI assay.29–31 A patient whose tumour is MSI-H or shows loss of MLH1/PMS2 on IHC, but lacks MLH1 promoter methylation likely has HNPCC, whereas one whose tumour was MSI-H with MLH1 promoter methylation probably does not.29–31
CORRELATIONS BETWEEN IMMUNOHISTOCHEMISTRY, MSI AND MUTATIONAL ANALYSIS
IHC has been shown to be a sensitive and specific method to detect MSI and is a powerful, albeit indirect, modality for detecting germline mutation.4 28 In the series by Modica et al,28 IHC with MLH1 and MSH2 antibodies had a sensitivity of 69% and a specificity of 100% in detecting MSI-H. When the panel was expanded to include PMS2 and MSH6 antibodies, the sensitivity for detection of MSI-H improved to 91%, but the specificity decreased to 83%. The decreased specificity was primarily due to a lack of correlation between loss of MSH6 expression and MSI-H. Loss of MSH6 expression has important implications regarding HNPCC diagnosis, irrespective of the lack of correlation with MSI-H. Endometrial carcinoma associated with HNPCC is more frequently associated with MSH6 mutations (fivefold higher) compared to colorectal cancers4 and mutations in MSH6 do not necessarily result in high levels of MSI.4 16 25 In Hampel et al’s study, there was one MSS case and two MSI-low cases in patients with Lynch syndrome associated MSH6 mutations.4
The positive predictive value of IHC for detecting a germline mutation, particularly with absent MSH2 or MSH6, has also been shown to be very high.4 17 In fact, it has been suggested that the current testing for MSH2 and MSH6 mutations is not 100% sensitive and that loss of these proteins by IHC even in the absence of detectable germline mutations may be sufficient evidence of Lynch syndrome.8 Compared to MSI analysis, IHC is a convenient test and is readily performed in most pathology laboratories. IHC is also advantageous as it can pinpoint the affected gene or genes, leading to an ability to target specific genes for sequencing.4 There are, however, reports of mutations in DNA-MMR genes that are not detected by IHC, therefore some experts still recommend using both IHC and MSI testing in combination to maximise the ability to detect every patient at risk for HNPCC.27
SCREENING ENDOMETRIAL CARCINOMAS FOR HNPCC
None of these detection methods can be applied routinely to every endometrial carcinoma. Given the shortcomings of using the restrictive criteria of age and personal/family history, other methods are required to narrow the pool of patients with EC to enrich for patients at high risk. Evaluation of tumour morphology is one such method.
The relationship between tumour morphology and the presence of MSI-H is well recognised in CRC and has been incorporated in the revised Bethesda guidelines.10 We and others have reported a similar relationship in EC,32–35 although this remains debatable and controversial.36 37
The morphological features in endometrial carcinomas that have been shown to correlate most with MSI-H include the presence of dense peritumoural lymphocytes apparent at low power magnification (fig 2), prominent tumour infiltrating lymphocytes (greater than 40 tumour infiltrating lymphocytes per 10 high power fields) (fig 3), and tumour heterogeneity defined as two morphologically distinct tumour populations juxtaposed but not intimately mixed with each other, and each constituting at least 10% of the tumour volume (fig 4).32 33 The dedifferentiated carcinoma, described by Silva’s group,38 is the prototypic example. Dedifferentiated carcinomas show foci of differentiated endometrioid adenocarcinoma (FIGO grade 1 or 2) with intimately associated undifferentiated carcinoma.38 The undifferentiated carcinomas are composed of sheets of fairly monotonous, ovoid to round cells with large nuclei that have vesicular chromatin and prominent nucleoli (fig 5). These are also remarkable for having variable amounts of background myxoid matrix and rhabdoid cells (fig 6). The study reporting the correlation between morphology and MSI33 targeted endometrioid carcinomas in particular, but other groups have reported MSI-H non-endometrioid tumours, some of which are HNPCC-associated, particularly clear cell carcinomas, rare serous carcinomas and malignant mixed Mullerian tumours (MMMT or carcinosarcomas).29 39–42

This endometrioid carcinoma shows prominent peritumoural lymphocytes evident even at scanning magnification.
The tumour shows prominent tumour infiltrating lymphocytes (only lymphocytes present between tumour cell borders qualify).

This dedifferentiated endometrial carcinoma shows a well differentiated glandular component juxtaposed against an undifferentiated component. Note the abrupt transition between the two elements.

The undifferentiated component is composed of solid sheets of round to oval cells without evidence of gland formation.

The undifferentiated carcinomas frequently show myxoid foci with rhabdoid cells containing abundant eosinophilic cytoplasm and eccentric nuclei with prominent nucleoli.
SCREENING ALGORITHM
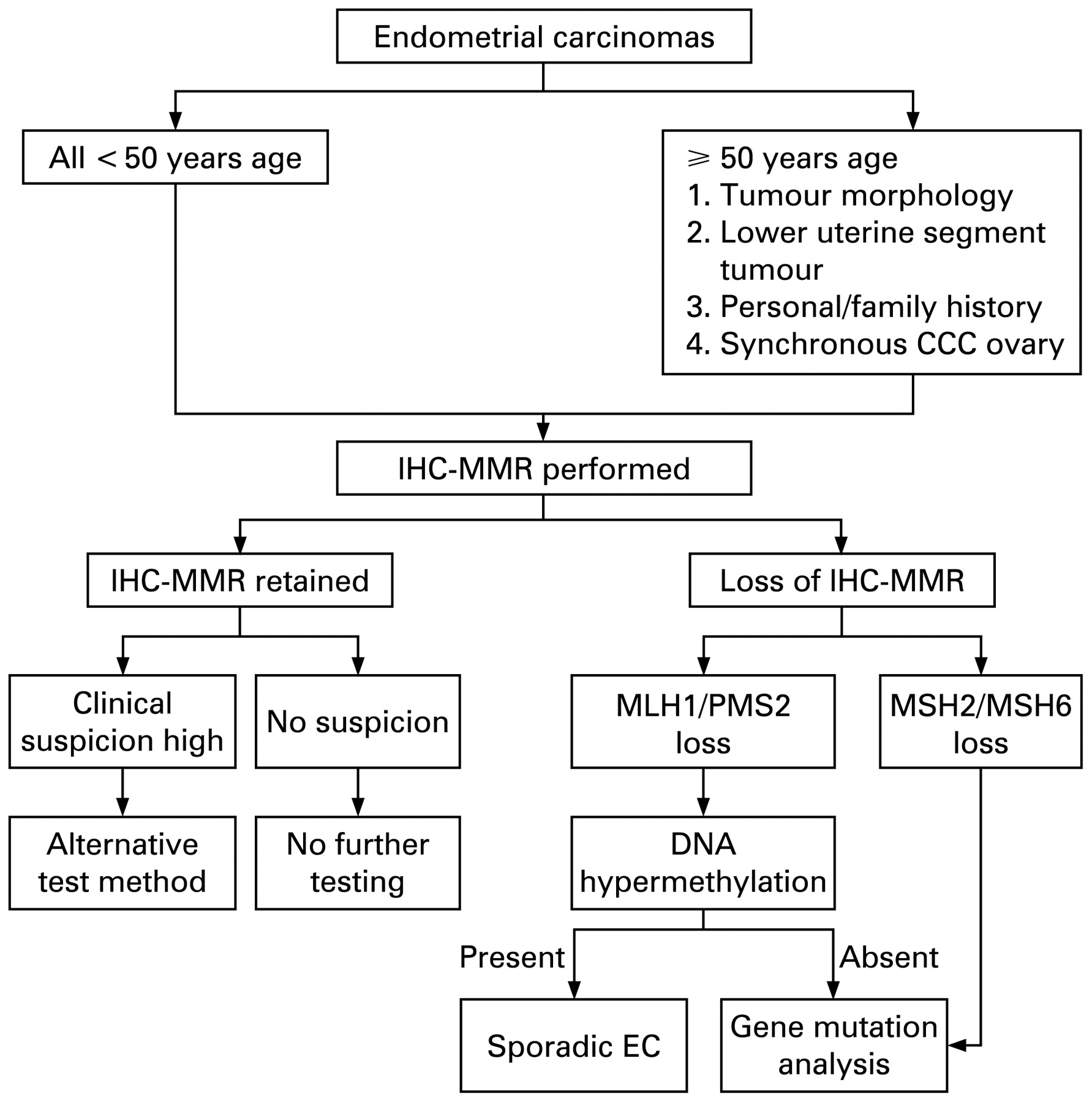
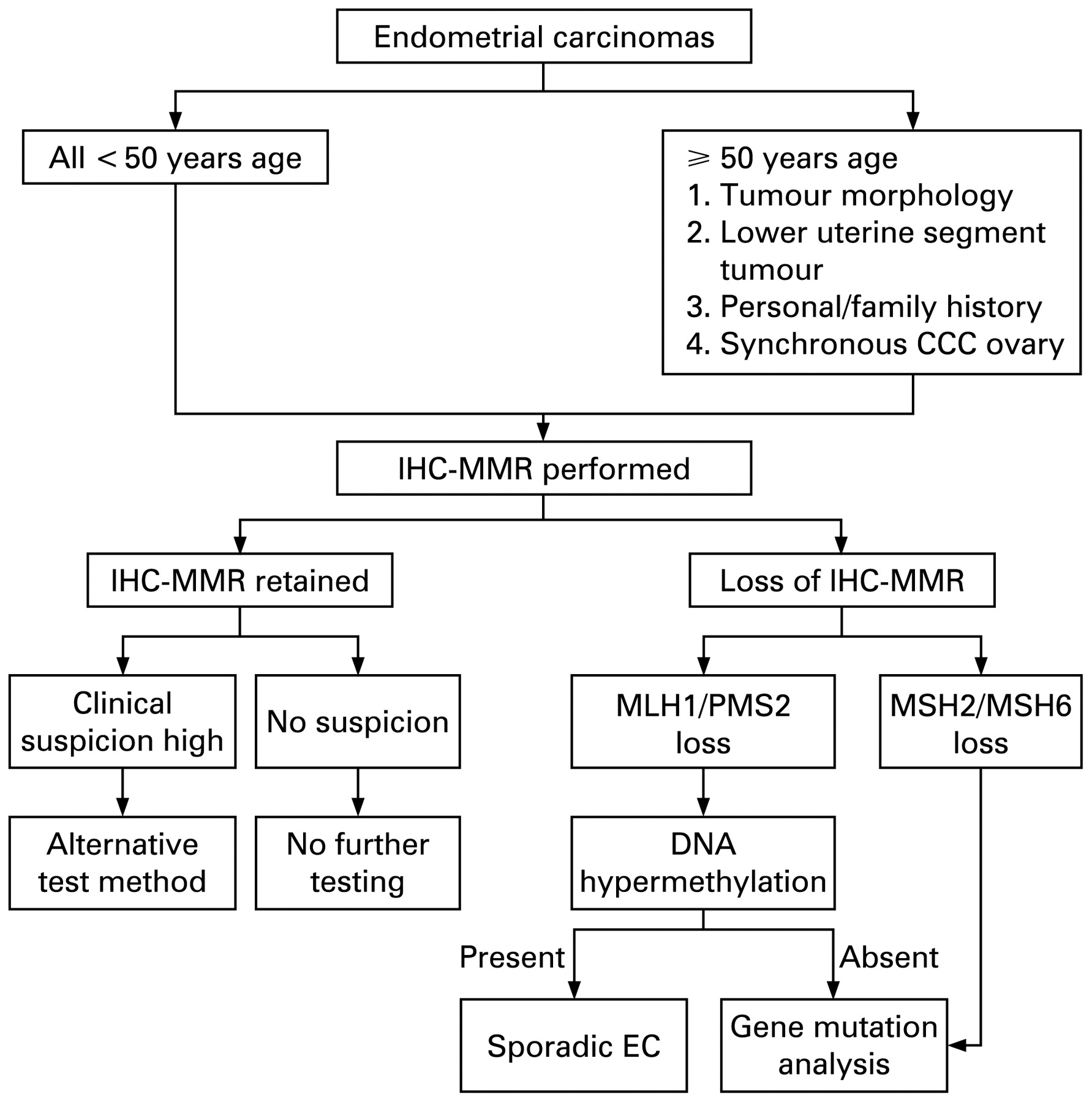
In an effort to define a target endometrial cancer population for HNPCC testing, we have begun to study DNA-MMR abnormalities by IHC in endometrial carcinomas that occur in women younger than 50 years, in older women whose tumours exhibit morphological features that have been reported to co-vary with high levels of microsatellite instability, as listed above,32 33 and when the personal or family history is highly suggestive of HNPCC (fig 7). The data from this study, which investigated the feasibility and utility of testing such patients’ tumours for DNA-MMR expression, indicated that tumour morphology significantly enhanced detection of tumours with loss of DNA-MMR by IHC.33 In patients 50 years of age or older, tumour morphology significantly enhanced the detection of loss of DNA-MMR by IHC (62%), compared to random EC patients of similar age (21%) (p<0.001).33 Furthermore, the detected cases showed a disproportionate representation of tumours lacking MSH2 and MSH6 expression, indirectly indicating mutation in either of the corresponding genes and membership in an HNPCC kindred.4 27 Tumours lacking MLH1 and PMS2 were also well represented, but additional testing is required in this scenario to determine whether loss of expression is due to epigenetic mechanisms (ie, a sporadic tumour) or a mutation.31 43 This study also confirmed that many of the patients with loss of IHC-MMR did not have personal and/or family history (60%) and many patients were older than 50 years (65%), including those with loss of MSH2 and/or MSH6.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proposed algorithm for detection of endometrial carcinoma patients at highest risk for hereditary non-polyposis colorectal cancer. IHC, immunohistochemistry; MMR, mismatch repair defect; EC, endometrial cancer; CCC, clear cell carcinoma.
In the younger than 50 years age group, approximately 30% showed abnormal IHC and in 63% of these cases, tumour morphology suggestive of MSI was present.33 In another study of endometrial carcinomas in women 40 years of age or younger, the rate of abnormal IHC for DNA-MMR proteins was 16% with a predominance of MSH2/MSH6 loss.44 The patients with abnormal IHC-MMR were notable for having lower body mass index (BMI) compared to those with retained IHC-MMR; they showed more frequent family history of cancer, and eight of these nine patients showed tumour morphology or topography (lower uterine segment localisation) associated with MSI.
In the study from Memorial Hospital, there was a large number of undifferentiated and dedifferentiated endometrial carcinomas, as described by Silva et al,38 that showed loss of DNA-MMR by IHC. These tumours have previously been described in association with MLH1 hypermethylation.29 In this study, most were associated with loss of MLH1/PMS2 but there were two cases with MSH2/MSH6 abnormalities, suggesting that they may be part of the HNPCC spectrum.
Recent literature also suggests that adenocarcinomas from the lower uterine segment (LUS) may be associated with HNPCC.45 These findings were confirmed in our study in which tumours from LUS were significantly over-represented in the group with abnormal DNA-MMR IHC.33
Patients with HNPCC are also at increased risk for developing ovarian carcinomas. An association between clear cell carcinoma of the ovary and MSI has been reported.46–49 In our series, there were two patients (one with a known MSH6 germline mutation) with EC and synchronous clear cell carcinoma of the ovary in the abnormal IHC group. On the other hand, synchronous endometrioid carcinomas of the ovary are not infrequent, and in the absence of significant personal or family history, do not appear to be associated with HNPCC.50
SCREENING ALGORITHM IN PRACTICE
Any patient with an abnormal immunohistochemical result is currently referred for a comprehensive genetics evaluation that might include MSI testing and, when indicated, methylation and mutational analysis of the candidate genes. The ethical and regulatory issues regarding reflexive IHC testing for DNA-MMR protein expression are currently unresolved. Some institutions require specific patient consent for IHC testing, whereas others have added general statements regarding genetic testing in standard surgical consent forms. Yet others do not currently require any patient consent, the idea being that IHC testing in this setting is not a direct test of a patient’s genome. If this approach is chosen, it is recommended that all involved pathologists, gynaecological oncologists and geneticists agree to the medical necessity of performing the test and arrange a chain of command that guarantees that all targeted patient material is tested and that all applicable patients are referred for the appropriate counselling.
PROGNOSTIC SIGNIFICANCE OF MSI IN EC
The clinical significance of MSI in endometrial carcinomas is unclear and controversial. Some studies have noted that in this setting, ECs are associated with poor prognostic indicators including higher histological grade, presence of lymphovascular invasion, deep myometrial invasion and higher clinical stage,33 44 51 while others have made the converse observations.52 Other studies have found no correlation between survival and MSI status in endometrial cancer,53 but others have found MSI to be independently associated with a favourable clinical outcome.54 The relative proportions of sporadic and heritable MSI-H ECs in each study might account for the differences reported. The clinical impact of MSI in EC is therefore currently poorly understood and should to be explored and validated in large studies with long-term follow-up.
Some small, retrospective studies have suggested that prophylactic hysterectomy and bilateral salpingo-oophorectomy may be an effective strategy for prevention of gynaecological cancers in women with HNPCC.55–57 Larger studies with long-term follow-up are required to establish the efficacy of prophylactic surgery in HNPCC.
CONCLUSIONS
The association between endometrial carcinoma and HNPCC/Lynch syndrome is important, but not well recognised. These patients and their family members are at risk for multiple cancers and should receive appropriate surveillance measures.
Available data suggest that application of immunohistochemistry for DNA mismatch repair proteins in EC with the following clinical and tumour characteristics may significantly enhance detection of MSI:
Endometrial carcinomas in women less than 50 years of age.
Endometrial endometrioid carcinomas in women of any age whose tumours demonstrate peritumoural or tumour infiltrating lymphocytes and tumour heterogeneity, particularly dedifferentiated EC.
Lower uterine segment localisation.
EC patients with synchronous ovarian clear cell carcinoma.
EC patients with strong personal or family history of HNPCC-related tumours.
The validity of these screening criteria should be tested with genotyping analysis. Once confirmed, consideration should be given to incorporating these screening criteria into a revision of the Bethesda guidelines for detecting EC patients at highest risk for HNPCC.
Acknowledgments
The authors would like to thank Dr David Klimstra and Dr Jinru Shia for their critical review of the manuscript.
REFERENCES
Footnotes
Competing interests: None.