Article Text

Abstract
Aims To quantify a range of haematological indicators of viral infection (leucocyte apoptosis, cytopenia of normal lymphocytes, reactive lymphocyte increase, neutropenia) in patients with recent onset invasive meningococcal disease (IMD), with a view to test the association of viral infection with IMD and identify possible haematological risk factors for its development.
Subjects and methods 88 patients with recent onset IMD, classified on clinical severity as fatal (n=14), septic shock survived (n=26) and no shock (n=48), and 50 healthy controls were studied. Blood film microscopy and leucocyte counts were used to quantify the virus-associated indicators. Cocci-containing neutrophils were also quantified.
Results All viral parameters were significantly more frequent or higher in patients than controls, with leucocyte apoptosis found only in the patients. A significant gradient in accord with clinical severity was found for neutrophil and lymphocyte apoptosis, neutropenia and cocci-containing neutrophils. Crucially, apoptotic neutrophils did not contain cocci, and cocci-containing neutrophils were not apoptotic.
Conclusions The correlation between magnitude of neutrophil apoptosis and severity of IMD suggests a cause–effect relationship. We propose that neutrophil apoptosis is more likely a facilitator rather than an effect of IMD for these reasons: (1) apoptotic neutrophils did not contain cocci and cocci-containing neutrophils were not apoptotic, (2) leucocyte apoptosis is a recognised viral effect and (3) Neisseria meningitidis is incapable of producing a Panton–Valentine type leucocidin. The lymphocyte apoptosis which accompanies neutrophil death may contribute to risk by impairing the generation of microbicidal antibody. Leucocyte apoptosis is a morphological expression of viral immunosuppression and, we suggest, is a likely contributor to a range of viral effects.
- Apoptosis
- Leucocytes
- Virus
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
A variety of factors affecting nasopharyngeal mucosal integrity, systemic immunity and the biology of the organism itself are risk factors for recent onset invasive meningococcal disease (IMD). These include: preceding viral infection, especially influenza A,1 mycoplasma infection,2 cigarette smoking, exposure to cigarette smoke or smokers, exposure to construction site dust,3–5 and deficiencies in systemic immunity relating to serum bactericidal antibody to meningococcus,6 ,7 mannose-binding lectin8 ,9 and more rarely, deficiencies in components of the terminal pathway of complement activation or properdin.10 A single risk factor may operate through several mechanisms; for example, the fact that postinfluenzal spikes of IMD are in general not accompanied by increased meningococcus carriage has suggested virus-induced neutrophil dysfunction as a contributor to risk.1 In addition, viruses have the capacity to enhance mucosal adhesiveness for bacteria11 ,12 or, in the case of influenza A, the capacity of its neuraminidase to cleave the sialic acid-containing capsular polysaccharides of Neisseria meningitidis serogroups B, C and W135 to enhance adhesiveness to epithelial surfaces.13 The innate capacity of the bacterial strain for invasiveness through epithelium is also significant in pathogenesis of IMD.14
We quantified a range of haematological indicators of viral infection with the aims of substantiating, from a novel perspective, the linkage between viral infection and IMD and of identifying possible haematological risk factors for its development. Leucocyte apoptosis was assessed, in addition to traditional leucocytic indicators of viral infection:15 reactive lymphocyte increase, cytopenia of normal lymphocytes (lymphocytopenia) and neutropenia. Apoptosis of leucocytes, including reactive lymphocytes, is a feature of the blood film in viral infections, including infectious mononucleosis (IM)16–19 (figures 2 and 3), neonatal herpes simplex viraemia17 ,20 (figure 1), rubella, measles17 and influenza A infection (Kerwick A-M, unpublished), and is the basis for the macrophage phenomenon in earlobe blood:16 ,21 monocytes/macrophages containing degenerate leucocytes (figure 3, ie, a process of haemophagocytosis), on account of their size, accumulate in the rich capillary bed of the earlobe, with simultaneous venous blood films showing few or none of these cells. The occurrence of apoptotic lymphocytes in the blood film in IM correlates with the upregulation of the Fas-receptor/Fas-ligand (Fas-L) system on the primed T lymphocyte population,22 and its propensity to substantial death in culture.23–25

Apoptotic neutrophil (left), apoptotic lymphocyte (right), blood film, neonatal herpes simplex viraemia. Reproduced, with permission, from Smith H. Diagnosis in Paediatric Haematology 1996. Churchill-Livingstone ©, Elsevier.

Degenerate neutrophil adherent to monocyte, earlobe blood film, infectious mononucleosis. Reproduced, with permission, from Smith H. Diagnosis in Paediatric Haematology 1996. Churchill-Livingstone ©, Elsevier.
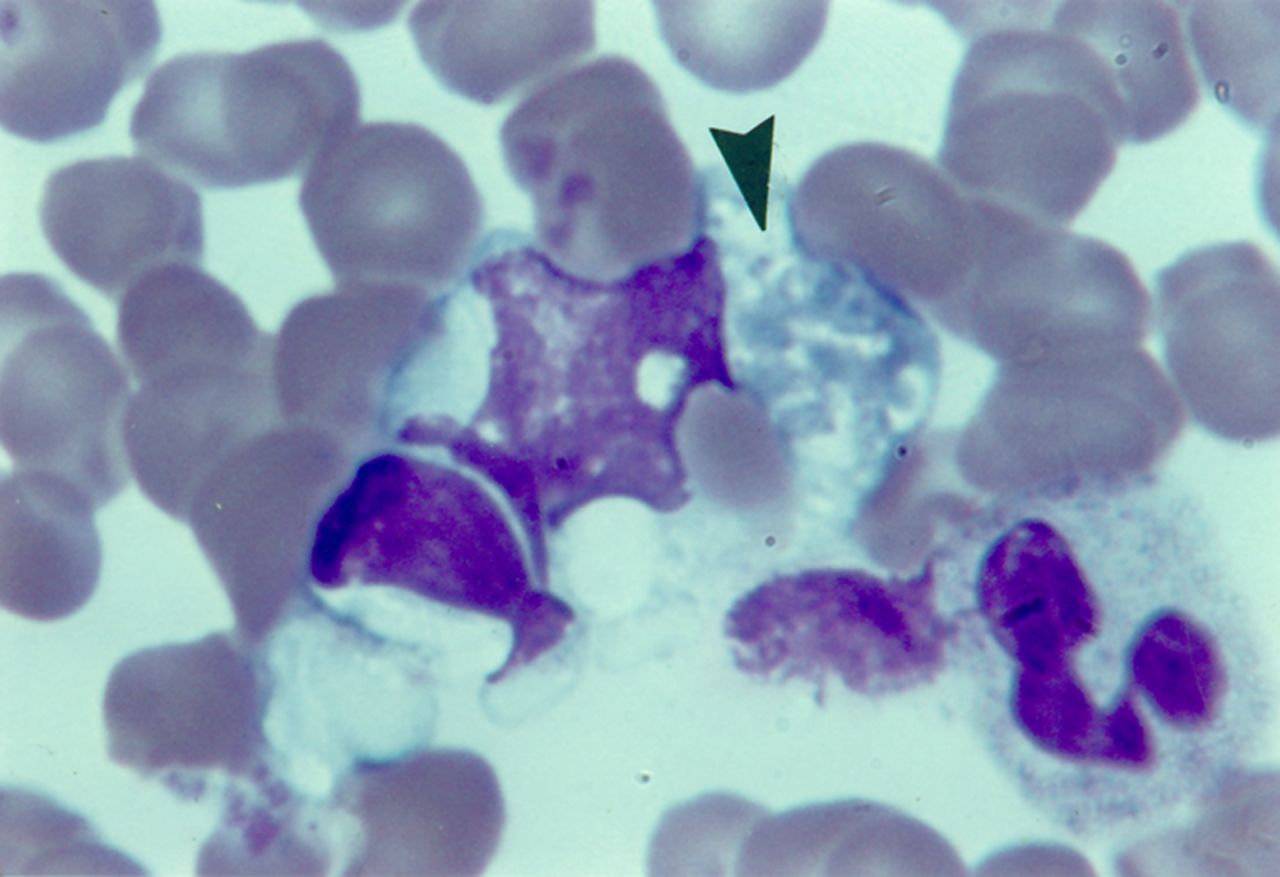
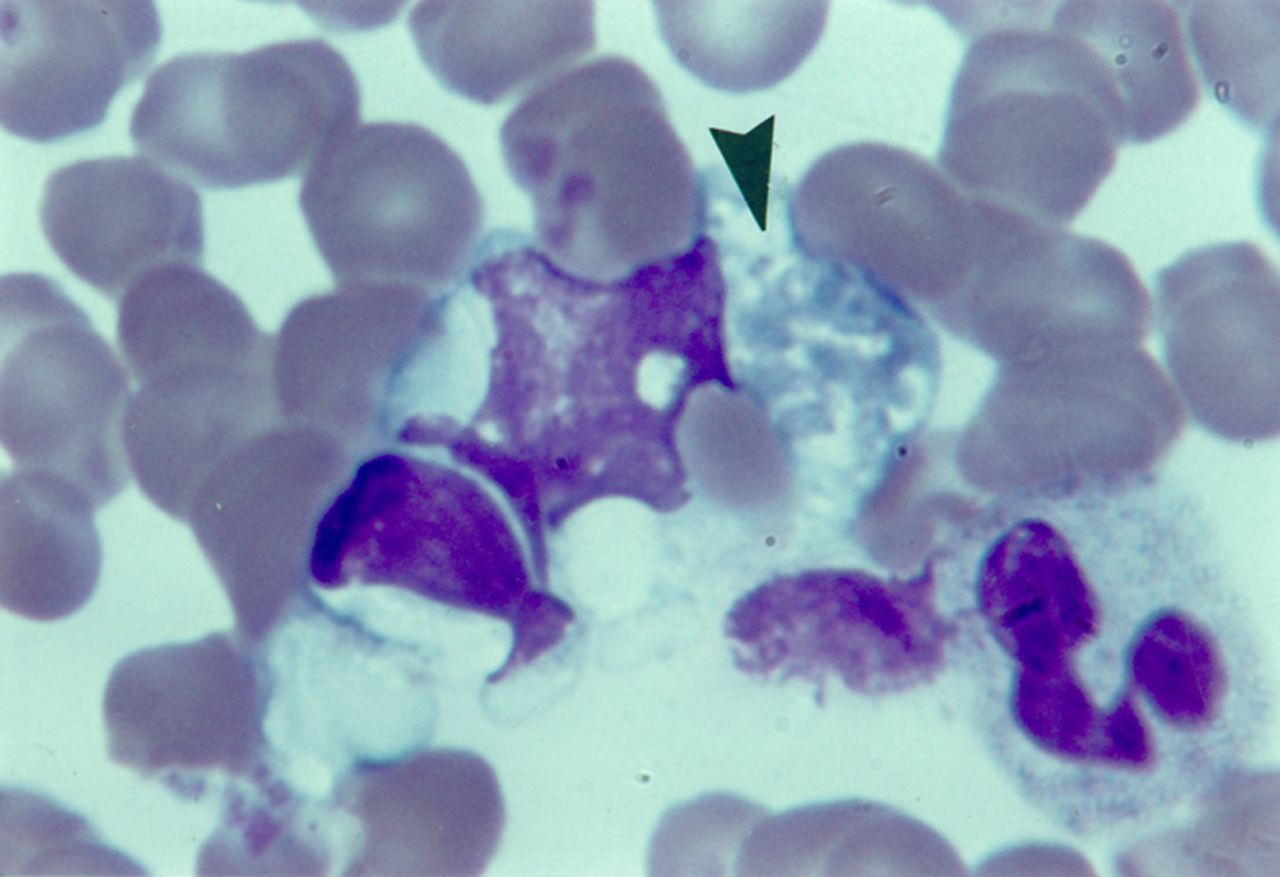
Inclusions of lymphocyte, erythrocyte and neutrophil in advanced degeneration (arrow) in monocyte, earlobe blood film, infectious mononucleosis. Reproduced, with permission, from Smith.17 Churchill-Livingstone ©, Elsevier.
Subjects and methods
Patients and controls
A total of 88 patients with recent onset IMD notified to the Queensland Health Public Health Microbial Reference Laboratory between October 2003 and October 2005 were studied. In all cases, cultures were positive from blood and/or cerebrospinal fluid, except for one patient, with culture positive only from the anterior chamber of an affected eye (table 1). Patients were classified into three groups on clinical severity: fatal, septic shock survived (hypotension with or without poor capillary refill) and no shock. There was a trend, but not significant, toward over-representation of younger patients in the fatal group. There was a significant over-representation of serogroup C in the fatal group. The control group comprised asymptomatic individuals with no clinical history of infection for at least 3 weeks prior to test. Children in this group were elective admissions for clean surgical procedures such as hernia repair.
Patients and controls
Blood film microscopy
Wright's stained blood films prepared immediately on receipt of EDTA-anticoagulated venous blood were used. Films were examined with an oil immersion ×60 planapochromat objective in the optimal part (one cell thick, evenly spread), working methodically in zigzag fashion from one edge to the other to end with a total of about 400–1000 leucocytes examined, depending on the leucocyte count (which took about 5 min). Large granular lymphocytes were counted as normal lymphocytes.
Apoptosis (figures 1⇑–3) was identified by condensation, obliteration of fine structure and glassy homogenisation of nuclear chromatin, leaching of chromatin stain into the cytoplasm, nuclear pyknosis and disintegration, and shrinkage of nucleus and cell as a whole. In advanced degeneration, especially of neutrophils, the chromatin may lose colouration and stain grey (figure 3). Some degenerate lymphocytes were recognisable as reactive or large granular types. These changes were readily distinguishable from anticoagulant/storage artefact.26
Established age-appropriate normal ranges for leucocyte counts15 ,17 were applied. Age-appropriate upper limits of normal for reactive lymphocytes were taken from our data for the controls as: for those <5 years, <0.09×109/L (<90 per mm3) and for those ≥5 years, <0.06×109/L (<60 per mm3). Apoptotic leucocytes and cocci-containing neutrophils (figure 4) were quantified both as a count per mm3 and, less precisely though nevertheless of some practical utility, as the proportion of subjects positive for the feature. This latter mode of expression of results, being only semiquantitative, was not subjected to statistical analysis. Cocci-containing monocytes17 were not seen in this study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Neisseria meningitidis within neutrophil, which is well preserved, blood film, invasive meningococcal disease. Courtesy of RG Wells.
Statistics
Proportions were compared by contingency tables analysis, including Armitage–Mantel–Haenzel ordered test between patient groups. Quantitative variables were compared by Kruskal–Wallis non-parametric one-way analysis (χ2 statistics).
Results
All viral parameters were significantly greater or more frequent in patients than in controls, with leucocyte apoptosis found only in the patients (table 2). The following characteristics showed a significant gradient in accord with clinical severity: apoptotic leucocytes as a whole (which included on average across all patient groups, 14.4% of dead leucocytes of unidentified type), apoptotic neutrophils, apoptotic lymphocytes, neutropenia and cocci-containing neutrophils. Crucially, apoptotic neutrophils did not contain cocci, and cocci-containing neutrophils were not apoptotic (figure 4). Of the traditional indicators of viral infection, lymphocytopenia was more sensitive than reactive lymphocyte increase or neutropenia, occurring in 77%–79% across all patient groups and in 10% of controls.
Leucocyte data, patients and controls
Discussion
The correlation between magnitude of neutrophil apoptosis and severity of IMD (table 2) suggests a cause–effect relationship. We propose that neutrophil death is a facilitator of IMD rather than an effect for these reasons: (1) Cocci-containing neutrophils were not apoptotic (figure 4) and apoptotic neutrophils did not contain cocci; these observations are in accord with studies suggesting that phagocytosed Neisseriea sp. can manipulate intracellular processes to enhance the survival of the neutrophil as a safe haven for dissemination of the infection.27 (2) The apoptosis of neutrophils and the death of lymphocytes which accompanies it in viral infection cannot be attributed to the operation of a Panton–Valentine type leucocidin (PVL): the meningococcus is incapable of producing PVL, and PVL targets neutrophils but not lymphocytes.28 (3) Neutrophil and lymphocyte apoptosis is a recognised effect of viral infection as noted in the Introduction section.
These observations substantiate the recognised linkage between viral infection and IMD. Of the leucocytic indicators of viral infection, neutropenia is the least specific, resulting as it may, from viraemia and from the disseminated intravascular coagulation which is common in severe IMD.29 In the discussion following therefore, we assume without prejudice, that apoptosis is cause rather than effect and that apoptosis is a result of viral infection and not of meningococcaemia.
The lymphocyte apoptosis which accompanies neutrophil apoptosis may be significant in pathogenesis of IMD by disrupting the T-B lymphocyte activation and interaction required for generation of bactericidal antibody.6 ,7 We have obtained preliminary confirmation of virus-associated lymphocyte apoptosis using flow cytometric assessment of annexin-V binding30 in IM, which showed enhanced binding by CD4, CD19, and especially CD8, but not natural killer lymphocytes (Smith H, unpublished). Apoptosis of monocytes, which may accompany the death of neutrophils and lymphocytes in viral infection,16 may contribute to pathogenesis of IMD by impairing the clearance of cocci and cocci-containing neutrophils.
Virus-associated apoptosis of neutrophils is not for the most part a consequence of viral penetrance of the cells. For example, in vitro studies of neutrophil apoptosis induced by herpes simplex virus (HSV)-131 and influenza virus-A (IVA)32 showed that the majority of apoptotic cells were not infected; in IM, only a small minority of blood neutrophils contain Epstein–Barr virus (EBV),33 though in vitro, a substantial proportion of neutrophils can bind EBV in spite of their lack of the EBV receptor, CD21.34 Virus-induced neutrophil apoptosis is attributed to upregulation of Fas and Fas-L on the few cells that are infected, with release of soluble Fas-L to then diffuse and bind to Fas-receptor on uninfected cells to initiate apoptosis.35 It is also possible that the susceptibility of neutrophils in vitro to the destructive effect of tumour necrosis factor (TNF)-α35 renders them vulnerable in vivo as well to TNF-α released from apoptotic lymphocytes whose death accompanies neutrophil death in viral infection. Neonatal, in contrast to adult neutrophils, may be especially susceptible to viral destruction, at least by HSV-131 which correlates with the marked leucocyte death in neonatal herpes simplex viraemia (figure 1).20
As with apoptosis of neutrophils, virus-induced death of lymphocytes is in general associated with low viral penetrance into cells and heightened Fas (CD95) expression. The in vitro induction of lymphocyte apoptosis by IVA36 affects CD8 rather than CD4 lymphocytes, and is diminished by anti-Fas but not anti-TNF-α antibodies; the clinical virulence of IVA strains correlated with the capacity to induce lymphocyte apoptosis and with neuraminidase activity. In IM, the expanded CD8 population shows strong expression of markers of activation24 ,25 and Fas,22 and high susceptibility to apoptosis in culture,23 ,25 and in vivo (Smith H, unpublished). Although EBV can infect CD4 and CD8 T lymphocytes in vitro,37 the expanded EBV-specific CD8 population in IM is not infected;23 and though Fas is upregulated on this population, inhibition studies show that the Fas system is not required for their apoptosis in culture25 (compare with IVA above). The cellular toxicity of cytochrome-c if released from damaged mitochondria, together with the fact that IM T cells in culture can be rescued from apoptosis by a range of cytokines, has suggested a mitochondrial/cytokine rescuable mechanism for the cell death.25 Interleukin-2, as an inhibitor of apoptosis,38 may have especial relevance, being markedly depleted in apoptosis-prone IM T cells in culture.39 In neonatal herpes simplex viraemia, the virus can invade and destroy lymphocytes.20
The relation between clinical severity and burden of cocci-containing neutrophils (table 2) accords with the experience that the main determinant of clinical severity in IMD is the magnitude of the bacteraemia.29
In the wider context of virus-induced pathology, we suggest that leucocyte apoptosis is a likely contributor to a range of viral effects: (a) Leucocyte death would add to T lymphocyte activation and proliferation as a source for the increase in plasma cytokines to which the malaise and fever of viral infection are attributed.40 A linkage between a profusion of apoptotic lymphocytes in the blood film in IM and a more severe and protracted illness19 supports this proposition. (b) Shedding from degenerating leucocytes would be a source of phosphatidylserine, which has the capacity to complex with plasma coagulation factors such as prothrombin, to enhance their antigenicity and generate antiphospholipid antibodies (lupus type anticoagulants),41 which are a not uncommon, transient occurrence in viral infections.42 (c) Leucocyte apoptosis may contribute to the neutropenia and lymphocytopenia of viral infection. (d) Leucocyte apoptosis may add to the increase in serum lactate dehydrogenase resulting from the liver damage and, less commonly, the immune haemolysis of viral infection.15 (e) Apoptosis contributes to depletion of CD4 lymphocytes which, together with depletion of functional macrophages, underlies the cutaneous anergy, as assessed by delayed hypersensitivity testing, which is common and severe in measles,43 ,44 and less so in IM.45 (f) The high increase in serum levels of soluble (s) CD8 in IM (sCD8∼102× normal, sCD4∼1.2× normal)46 may be attributed to high activation and proliferation of the CD8 population, and to its high death rate in vivo (see above). (g) Leucocyte apoptosis, by stimulating phagocytosis, and activation of macrophages may be significant in the genesis of virus-associated haemophagocytic syndrome,47 the morphology of which can be readily appreciated in first drop earlobe blood films (figure 3), a technique now rarely employed.16
The model we propose for virus–IMD association may also apply to other viral–bacterial associations, such as postinfluenzal pneumococcal sepsis, and neonatal herpes simplex viraemia presenting as bacterial septicaemia.
What the study adds
-
Haematological indicators of viral infection substantiate the association of viral infection with invasive meningococcal disease (IMD). Leucocyte apoptosis is a morphological expression of viral immunosuppression and a likely facilitator of IMD: neutrophil death by impairing phagocytic capacity, and lymphocyte death by impairing generation of microbicidal antibody. In the wider context of viral pathology, we suggest that leucocyte apoptosis is a likely contributor to a range of viral effects, including fever and malaise, lupus-type anticoagulants, blood cytopenias, cutaneous anergy, and virus-associated haemophagocytic syndrome.
Take home messages
-
Haematological indicators of viral infection substantiate the association of viral infection with invasive meningococcal disease (IMD).
-
Leucocyte apoptosis is a morphological expression of viral immunosuppression and a likely facilitator of IMD by impairing two arms of the immune system: phagocytic capacity (neutrophil death) and generation of microbicidal antibody (lymphocyte death).
-
Leucocyte apoptosis is a likely contributor to a range of viral effects.
-
The virus–meningococcal link may be a model for other viral–bacterial associations.
-
We suggest that virus-associated leucocyte apoptosis merits more detailed analysis.
Acknowledgments
We thank the following for their assistance in this study: M Coulthard, L Dial, J Faoagali, S Hall, Herston Medical Library, S Miller, R Minchinton, J McEniery, R Potter, R Prentice, C Wainwright and B Webster.
References
Footnotes
-
Contributors HS: conception, design and coordination; writing of manuscript, which was approved by all coauthors. SLR: blood film microscopy. HVS: meningococcus identification and serogrouping. DG: critical commentary on immunological aspects of the phenomenon. VS: statistical analysis. JAS: sourcing and critical assessment of references, presentation of manuscript.
-
Funding Royal Brisbane and Women's Hospital Foundation.
-
Competing interests None.
-
Ethics approval Only blood samples already taken for routine diagnostic purposes were used in this study. Queensland Health Research Ethics Committee approval HREC/03/QH/029, Chair Professor M Eadie .
-
Provenance and peer review Not commissioned; externally peer reviewed.