Article Text

Abstract
Accurate histopathological assessment of biopsies is important for the diagnosis, subclassification, and management of chronic idiopathic inflammatory bowel disease (IBD). British Society of Gastroenterology (BSG) guidelines for the initial histopathological diagnosis of IBD were published in 1997. Changes since then include: more widespread use of full colonoscopy; greater recognition of the effects of time and treatment; improved documentation of variations in anatomical distribution; better understanding of the mimics of IBD; significant progress in clinical management; and modifications of terminology. Accordingly, an update is required. These revised guidelines aim to optimise the quality and consistency of reporting of biopsies taken for the initial diagnosis of IBD by summarising the literature and making recommendations based on the available evidence. Advice from existing clinical guidelines is also taken into account. Among the subjects discussed are: distinguishing IBD from other colitides, particularly infective colitis; subclassification of IBD (as ulcerative colitis, Crohn's disease, or IBD unclassified); the discriminant value of granulomas; aspects of disease distribution, including discontinuity in ulcerative colitis; time-related changes; differences between paediatric and adult IBD; the role of ileal and upper gastrointestinal biopsies; differential diagnoses such as diverticular colitis and diversion proctocolitis; and dysplasia. The need to correlate the histological features with clinical and endoscopic findings is emphasised. An approach to the conclusion of an IBD biopsy report based on the acronym Pattern, Activity, Interpretation, Dysplasia (PAID) is suggested. The key recommendations are listed at the end of the document.
- Histopathology
- Inflammatory Bowel Disease
- Colitis
- Crohn's Disease
- Diagnosis
Statistics from Altmetric.com
Introduction: guideline development process
Update: reasons
The British Society of Gastroenterology (BSG) guidelines for the initial histopathological diagnosis of inflammatory bowel disease (IBD) were published in 1997.1 An update is now due. In a national survey, histopathologists identified diverticular colitis, diversion colitis, indeterminate colitis and grading of activity as subjects needing attention.2 Further reasons for an update include greater use of full colonoscopy rather than limited site sampling,3 and better recognition of the effects of time and treatment on histology.3 ,4
Objectives
-
To optimise the quality of reporting of biopsies taken for the diagnosis of IBD.
-
To promote consistency of pathologists’ approach to reporting.
-
To encourage correlation between histological and clinical findings, including discussion at clinicopathological meetings.
-
To minimise the use of ambiguous or confusing terms.
Process
The advice provided by the BSG at the time of writing was followed, with some exceptions which are mentioned below (see online supplementary appendix 1 for more details).
Authorship and review
Draft versions were initially submitted by the author to the pathology section committee of the BSG for review. The content has now been discussed with and approved by the pathology section committee, the clinical services and standards committee of the BSG, and the chair of the IBD section of the BSG. The document is also approved by the British Division of the International Academy of Pathology (BDIAP).
Patient groups
The patient groups covered are those with IBD and relevant related gastrointestinal diseases. At the time of drafting, patient representation was not considered appropriate for the development of a guideline of this type. However, the document repeatedly emphasises the need for good communication between pathologists and clinicians.
Search strategy and sources of evidence
The advice and recommendations are variably based on peer-reviewed publications, expert opinions, accepted practice and consensus. To identify relevant studies, a PubMed search was done using combinations of key words, for example, IBD, ulcerative colitis (UC), Crohn's disease (CD), histopathology (see online supplementary appendix 1). With one exception, papers published before 1984 were not included. Publications were reviewed critically, followed where required by detailed tabulation of findings from multiple studies.
Recommendations and evidence from established guidelines were also taken into account. These included clinical and pathological guideline documents produced by the European Crohn's and Colitis Organisation (ECCO),3 ,5 the BSG,6 the World Congress of Gastroenterology,7 the UK Royal College of Pathologists,8 and UK cancer screening programmes.9 The previous set of BSG IBD reporting guidelines for histopathologists was consulted frequently.1
Evidence levels
Evidence levels (EL) and graded recommendations (RG) suggested by the Oxford Centre for Evidence-Based at the time of writing (http://www.cebm.net/index.aspx?o=1025, and reproduced in online supplementary appendix 3), are given where possible. This system was preferred over others because it is used in existing ECCO and BSG IBD guidelines.3 ,5 However, it can sometimes be difficult to apply to histopathology.
Initial versus follow-up biopsies
The guidelines have, where possible, distinguished initial biopsies from follow-up biopsies. This is very important because histological features and patterns of disease are influenced by the passage of time and by drug therapy.
Discriminant histological features: further considerations
In the tables and discussions of discriminant features in the sections on IBD versus non-IBD: histology, and ulcerative colitis versus Crohn's disease: histology:
-
Studies confined to initial biopsies are favoured strongly over those which include non-initial biopsies.
-
Abnormalities are generally regarded as reliable if they are consistently discriminant in at least two reports, with no contradictory findings in other reports.
-
Additional emphasis is given to studies of multiple-site biopsies, though such publications are sparse.
-
True ‘meta-analysis’ is often impossible because terminology, definitions, comparisons and subgroups may differ.
Implications
Acceptance of the recommendations in this document might generate more biopsies and increase the workload for histopathologists and other staff. However, it could also help improve patient management, which in the longer term might reduce both workload and costs. An audit after at least 18 months of the value and practicality of the guidelines would help determine the content of a further update. A more detailed summary of possible implications is given in online supplementary appendix 2.
Clinical considerations
Value of biopsy assessment
Reasons for taking a biopsy include:
-
confirmation of the diagnosis of IBD
-
exclusion of coexistent conditions or complications.10
The following may also be assessed:
Most initial biopsies for IBD are taken because symptoms or endoscopic features suggest the diagnosis.
Clinical details
Diagnosis and classification of IBD depend on a combination of clinical, endoscopic and pathological features.11 ,13–15 Several entities can mimic IBD clinically and histologically (EL2a RGB) (see section on Mimics of IBD).13 ,14 Correlation of histological features with clinical and endoscopic findings is essential and is facilitated by participation in multidisciplinary meetings where IBD cases are discussed. Indeed, better interaction between histopathologists and endoscopists has been formally recommended in clinical guidelines.16
Tissue sampling
Biopsies from endoscopically normal and abnormal mucosa should be available.5 ,17 For optimal diagnosis and classification of IBD there should be samples of the ileum, at least four colonic sites, and the rectum, with a minimum of two biopsies from each site (EL1b RGB).5 Biopsies should be submitted in such a way that their site of origin can be determined, for example, using multiple specimen containers, acetate strips, or multiwell cassettes.5 ,8
Diagnostic categories
The main questions asked by the histopathologist when assessing an initial biopsy for IBD are (as suggested previously)1:
-
Is the mucosa inflamed?
-
If the mucosa is inflamed: is it IBD or not?
-
If it is IBD: is it UC, CD, or IBD unclassified?
The term ‘indeterminate colitis’ is not used for biopsy reporting (see section on Terminology).
Probability
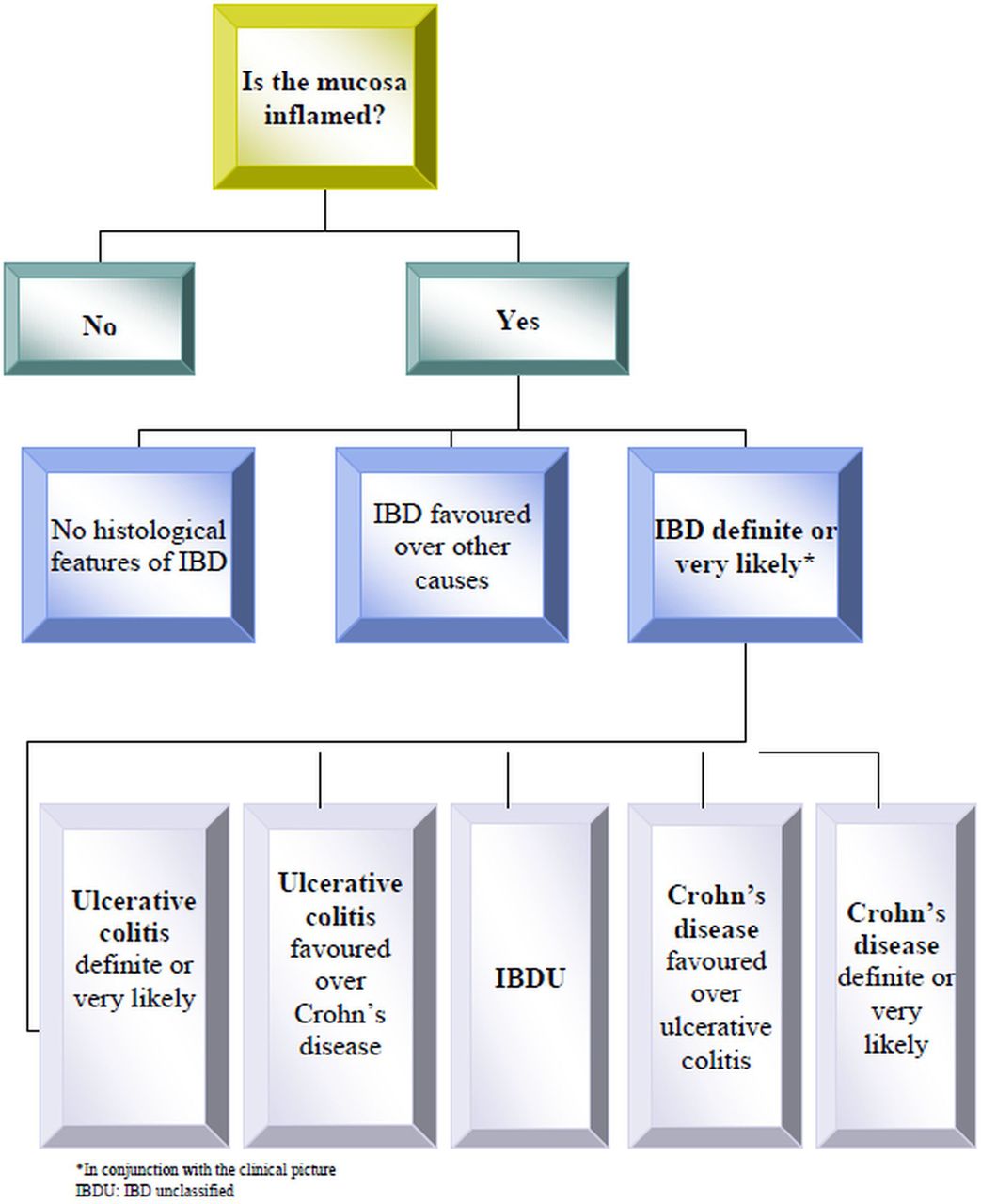
It may be convenient to consider categories of probability, for example, definite/very likely and favoured. This is discussed in more detail in the sections on Terminology and Reporting scheme for IBD biopsies (PAID) and outlined in figure 1.

Categorisation of inflammation in biopsies taken for the initial diagnosis of inflammatory bowel disease. This is a simplified outline of the steps. In practice, the process is more complex and also considers the clinical and endoscopic features. All cases are categorised in conjunction with the clinical and endoscopic picture.
Recommendations: clinical considerations
-
Accurate histopathological assessment is important for optimum diagnosis, subclassification and management of IBD.
-
Biopsies for the diagnosis of IBD should be accompanied by a full clinical history and a record of endoscopic findings (EL2a RGB).3 ,13 The history should include the duration of disease and details of medical and surgical treatment.3
-
A regular clinicopathological meeting for discussion of IBD cases should be available.
Features of normal and abnormal mucosa
Normal mucosa
Chronic inflammatory cell density
When assessing chronic inflammatory cells, plasma cells are easier to identify than lymphocytes (EL5 RGD).5 ,18 Normally, chronic inflammatory cells are most dense in the upper third of the mucosa. Their density decreases towards the base, resulting in the ‘plasma cell gradient’ (figure 2A).15 ,19

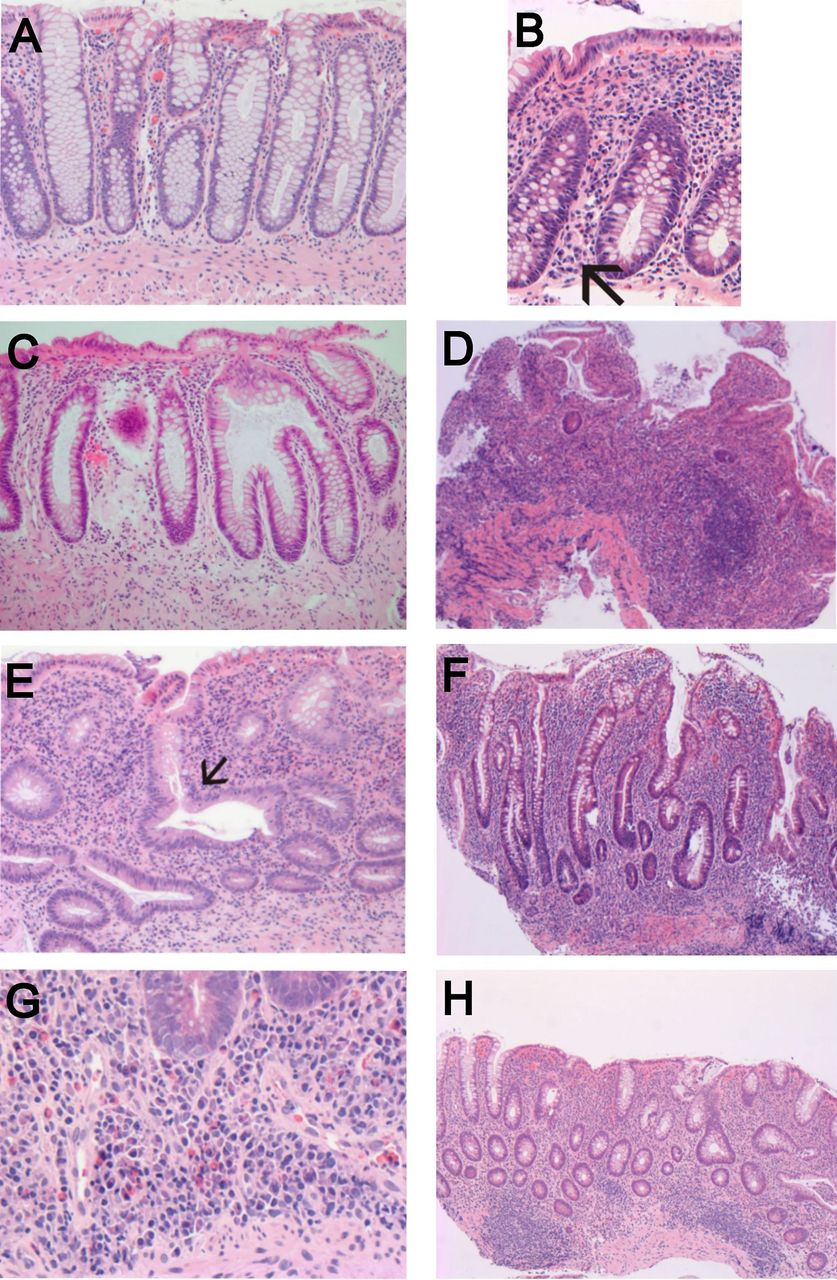
(A) Normal large bowel mucosa with a decrease in plasma cell density from the upper third of the lamina propria to the lower third—the ‘plasma cell gradient’. Basal plasma cells are infrequent or absent. Note also that crypt architecture is preserved; the crypts are parallel to each other and extend from the lumenal surface to the muscularis mucosae. (B) In the caecum and ascending colon, overall lamina proprial cell density is higher than elsewhere. Basal plasma cells may be seen at these sites (arrow) and should not necessarily be interpreted as chronic inflammation. (C) Occasional branched crypts, as in this biopsy, are acceptable if unaccompanied by any other abnormality. However, they should prompt a search for other evidence of inflammation. (D) An irregular or villiform mucosal surface in the large bowel is abnormal and is a useful marker for inflammatory bowel disease (IBD). It is more prevalent in ulcerative colitis than in Crohn's disease. Severe diffuse crypt atrophy and diffuse chronic inflammation are also apparent in this case of ulcerative colitis. (E) Crypt architectural distortion. Crypt distortion includes crypt branching and loss of parallelism. The centrally placed crypt shows ‘horizontal’ branching (arrow). (F) Mild crypt distortion, including ‘vertical’ crypt branching. The diagnosis of IBD is lent additional support by a ‘transmucosal’ lamina proprial chronic inflammatory infiltrate with loss of the plasma cell gradient and by the presence of crypt atrophy (which is mild). (G) Basal plasmacytosis (plasma cells at the base of the mucosa) is a very useful objective marker for IBD if there is doubt about the presence of chronic inflammation. Some of the plasma cells lie beneath shortened crypts—‘crypts with their feet in pools of plasma cells’.4 Other inflammatory cells are present, but plasma cells are the easiest to detect. (H) Basal lymphoid aggregates may be seen in IBD mucosa. They can be difficult to distinguish from normal lymphoid aggregates.
The density and distribution of chronic inflammatory cells varies with anatomical site.15 Cellularity is highest in the caecum/ascending colon (figure 2B) and may be low in the rectum (EL5 RGD).15 ,19 Absence of the plasma cell gradient is accepted as normal in the caecum and ascending colon (figure 2B) (EL5 RGD). Dense lymphoid tissue may be found in the normal large bowel, particularly in the rectum (EL5 RGD).20
Histiocytes/macrophages
Recognition of histiocytes is difficult unless they contain pigment or mucin (muciphages)19 ,21 or form aggregates. Muciphages are a normal finding and are more common in the rectum than elsewhere (EL5 RGD). They are of no diagnostic significance. However, they can resemble the cells seen in other conditions, such as atypical mycobacterial infection and Whipple's disease, which should be excluded if appropriate.22
Eosinophils
The normal lamina propria contains eosinophils. There are few definitions of the criteria for normality or for a significant increase.23 Furthermore, assessment of their density or numbers is of limited value11 despite earlier reports to the contrary. Sparse eosinophils may be seen in the normal surface epithelium.19
Acute inflammatory cells
A few intraepithelial neutrophils (eg, two or three per biopsy) may reflect bowel preparation (EL5 RGD).1 Nevertheless, the presence of any intraepithelial neutrophils is probably not normal and should trigger a search for other evidence of inflammation.19
Crypt architecture
Normal crypts in a perfectly orientated biopsy are parallel to one another and extend from the surface to the muscularis mucosae (figure 2A). Imperfect orientation can produce a false impression of crypt distortion or shortening (EL5 RGD). Occasional branched crypts can be ignored (figure 2C),1 particularly at innominate grooves.19 The rectal mucosa may show more irregularity and shortening of crypts, especially near the anorectal junction. Also, the mucosa up to a distance of three crypts from a lymphoid aggregate is not entirely reliable for assessment of architecture.
Microscopic abnormalities
Definitions
Published definitions of microscopic abnormalities are not always consistent. A summary of some definitions is given in table 1.1 ,5 ,25–27
Definitions of some histological features
Categories of abnormality in colorectal biopsies
Three main categories of colorectal mucosal histological abnormality may be considered (as discussed in previous guidelines).1 ,3
-
Architectural; for example, crypt distortion, crypt atrophy, surface irregularity (figure 2D–F).
-
Inflammatory; for example, lamina proprial chronic inflammation, granulomas, neutrophils.
-
Epithelial; for example, mucin depletion, Paneth cell metaplasia.
Crypt distortion
This category encompasses various terms (table 1) (figure 2E,F).5 ,28 Crypt branching may be the easiest to define and recognise. Branching has occasionally been subclassified as vertical and horizontal4 but this may be difficult to apply (figure 2F). In most examples of crypt distortion the ‘test-tube’ arrangement of normal crypts is at least partly lost, that is, there is ‘loss of parallelism’ (figure 2E,F).
Crypt atrophy
Crypt atrophy (figure 2D) encompasses crypt shortening and wider crypt spacing. It is closely related to crypt architectural changes. However, its inclusion under the heading of architectural distortion is not recommended (EL5 RGD).
Chronic inflammation and lymphoid aggregates
Basal plasmacytosis and ‘loss of the plasma cell gradient’ are objective markers of IBD (figure 2D,F,G) (table 1).4 Attempts to define numbers21 have not been widely accepted. A transmucosal increase in lymphocytes is also likely to be significant but is difficult to confirm objectively. Basal lymphoid aggregates can be difficult to distinguish from normal lymphoid aggregates (figure 2H).
Granulomas and giant cells
It has been suggested that a granuloma should include at least five epithelioid macrophages (EL5 RGD).25 Crypt rupture should be excluded (figure 3A) (EL4 RGC) (see section on Ulcerative colitis vs Crohn's disease: histology).29 Multinucleate giant cells (not necessarily part of a granuloma) may be diagnostically useful but can also reflect crypt rupture.

{kind=link}
{kind=link}
{kind=link}
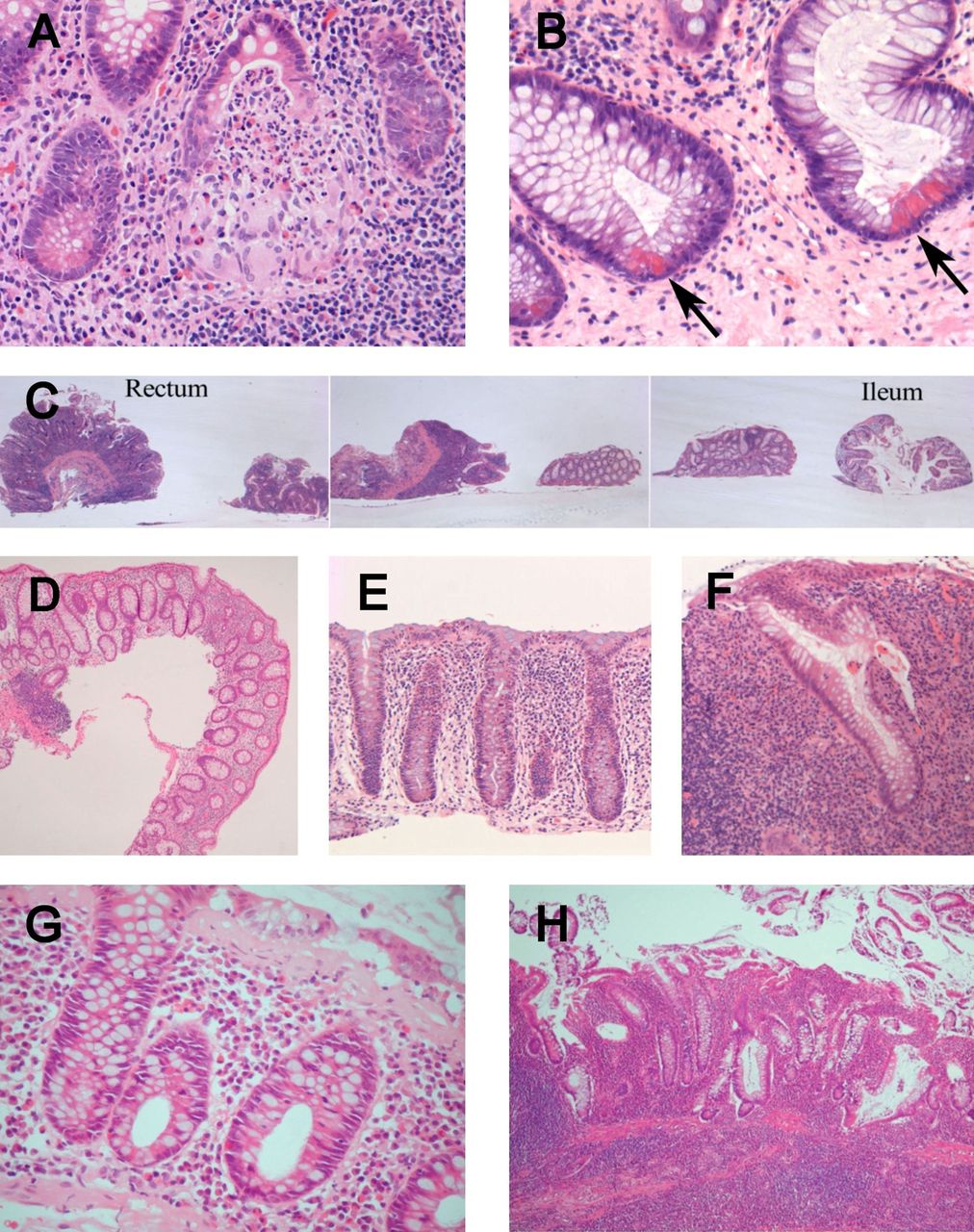
(A) A cryptolytic granuloma resulting from rupture of a crypt abscess. Cryptolytic granulomas are not discriminatory. (B) Paneth cell metaplasia (arrows) with supranuclear eosinophilic granules. This is a case of longstanding ulcerative colitis. (C) Distribution within and between sites. The ileum (far right) and adjacent more proximal colonic biopsies are not inflamed, while the three most distal (left-sided) biopsies show chronic inflammation, crypt distortion and crypt atrophy which are continuous between sites and diffuse within each biopsy. This is virtually diagnostic of ulcerative colitis (assuming the appropriate clinical setting). (D) Distribution of changes within a biopsy: patchy chronic inflammation in Crohn's colitis. Note the variation in lamina proprial cellularity and very focal crypt distortion. (E) Probable infective colitis. There is upper lamina proprial hypercellularity but no basal plasmacytosis or loss of the plasma cell gradient. Cryptitis is unusually extensive for an infective colitis. (F) Diversion proctocolitis showing diffuse chronic inflammation and crypt distortion. This inflammatory bowel disease (IBD)-like pattern can be seen whether or not there is a past history of IBD, but tends to be most severe in the setting of ulcerative colitis. (G) Collagenous colitis. Basal plasma cells and loss of the usual plasma cell gradient might raise the possibility of IBD, but the correct diagnosis is indicated by the presence of a thickened subepithelial collagen band, epithelial degenerative changes and preserved crypt architecture. Lymphocytic colitis might pose similar problems. (H) Diverticular colitis showing features reminiscent of ulcerative colitis, including diffuse chronic inflammation and extensive crypt distortion. This is a relatively common mimic of IBD in biopsy diagnosis.
Mucin depletion
Normal mucosa contains abundant mucin as droplets in goblet cells. This is usually less plentiful in the surface than in the crypt epithelium (figure 2A). Depletion can be graded as mild, moderate, or severe, but this is subjective (figure 2D,F).
Paneth cell metaplasia
Paneth cell metaplasia (figure 3B) is probably only significant if it is distal to the splenic flexure (EL3b RGC)30 and, additionally, is probably a marker of longstanding disease rather than a reliable discriminant feature.3 ,25
Recommendations: features of normal and abnormal mucosa
-
Pathologists should be familiar with the features of normal mucosa and with definitions of the abnormalities that are encountered in IBD biopsies.
Distribution, extent and activity
Distribution of disease
Assessment of distribution
It is useful to assess the distribution of chronic inflammation and crypt changes
-
between anatomical sites
-
between biopsies from the same site
-
within biopsies.
The distribution of acute inflammation should also be noted.
Terms for distribution within biopsies and within a single site
The terms diffuse, patchy and focal are used for chronic inflammation. The terms diffuse and focal are also used to describe crypt changes and acute inflammation (although the latter has less value for disease categorisation). The boundary between ‘focal’ and ‘patchy’ is not well defined. Suggested definitions include:
-
Diffuse chronic inflammation: an overall increase in chronic inflammatory cell density throughout the biopsy/biopsies (figures 2D,F and 3C).3
-
Patchy chronic inflammation: areas of increased chronic inflammatory cell density in a background of variable cellularity (figure 3D).3
-
Focal chronic inflammation: well circumscribed foci of increased chronic inflammatory cell density in a normocellular background.3
Terms for the distribution between sites
The terms listed above for a single site are sometimes also used to describe distribution between anatomical sites. This can cause confusion. The alternative terms ‘continuous between sites’, ‘discontinuous between sites’ or ‘segmental’ (ie, non-continuous anatomically)21 are preferable.
Diagnostic value of distribution in untreated disease
Assessment of the distribution of changes between sites, within sites, and within biopsies is very helpful for distinguishing UC from CD.36 As a result of the increased use of full colonoscopy there are more opportunities to observe distribution between sites than there were in the past. There is strong evidence that IBD is classified more accurately by multiple site sampling than by limited site sampling (EL1b RGA).5 ,14 ,21 ,34 ,36 ,37
-
Distribution between sites: continuous involvement favours UC while discontinuous/segmental abnormalities favour CD (figure 3C) (EL2a RGB).21 ,36 However, well-recognised exceptions exist (table 2).
-
Distribution within sites or within biopsies: diffuse involvement favours UC while focal or patchy changes favour CD (EL2b RGB) (figure 3C,D).
-
An increase in severity from proximal to distal favours UC, while right-sided predominance favours CD (EL5 RGD).3 ,36
-
Treatment and duration of disease can modify the distribution (see below).
Discontinuous changes in ulcerative colitis
Analysis of distribution between sites also helps distinguish IBD from some other colitides, for example, diverticular colitis (typically confined to the sigmoid colon), infective colitis (may involve all sites, but varies according to the infective agent), and ischaemic colitis (often localised, eg, to the splenic flexure).
Exceptions: discontinuous change in UC
Although UC is typically continuous between anatomical sites, there are various exceptions to the rules (table 2).
-
The caecum may show changes reminiscent of UC despite an uninvolved adjacent colon (caecal patch). Also, there may be apparent rectal sparing endoscopically or in biopsies (though not in resections) (EL1a RGA).28 ,31 ,38–40 These phenomena do not change the diagnosis but should lower the threshold for considering CD.3
-
‘Appendiceal UC’ may be discontinuous with colonic disease (‘skip’ lesion).39 ,41–44
-
Longstanding and/or treated UC may be distributed unevenly between sites, within sites, and within biopsies.
Extent of disease
Extent of IBD is mainly determined endoscopically. The extent of UC helps predict the risk of dysplasia.7 The extent of CD is more difficult to define.5 Histological extent does not always correlate with endoscopic extent,5 ,39 but its documentation may be useful to clinicians.
Activity
Inflammation in IBD biopsies may be classified as chronic, active chronic, or active (acute).48 Histological confirmation of activity requires cryptitis, crypt abscesses, surface epithelial neutrophils, erosion, or ulceration. Lamina proprial neutrophils may be seen in IBD, but their presence is not usually regarded as a criterion for histological activity.45 ,49–51 There is no widely agreed scheme for grading histological activity in IBD,3 but several have been proposed40 ,52–54 and have been taken into account in the scheme suggested in the section entitled ‘Reporting scheme for IBD biopsies (PAID)’ later in this document.
The assessment of activity is often based on endoscopy.12 The value of histological estimation of activity is uncertain5 and has not been compared to the value of endoscopic measures of activity. However, its use has increasingly been recommended to help stratify patients into risk categories for cancer screening,12 and to determine completeness of remission following treatment.55–57 Comparisons between endoscopic and histological activity may be limited by sampling error.5 ,40
Recommendations: distribution, extent and activity
-
Distribution of microscopic changes within biopsies, between biopsies and between sites should be assessed (EL1b-2b RGB).
-
The terms ‘diffuse’, ‘patchy’ and ‘focal’ can be used for distribution within sites.
-
The terms ‘continuous between sites’ and ‘discontinuous between sites’ (or its synonym ‘segmental’) can be used for distribution between sites.
-
There are several exceptions to the typical continuous distribution of UC, even at initial presentation, (EL1a RGA) that should not necessarily prompt a change of diagnosis. These include a caecal patch and rectal sparing.
-
Histological activity in IBD should be graded,3 while recognising the limitations of this assessment (EL5 RGD).
IBD versus non-IBD: histology
IBD versus normal
Some studies list the features that are more frequent in IBD than in normal mucosa, for example, abnormal crypt architecture, crypt distortion, crypt atrophy, basal plasmacytosis, lamina proprial hypercellularity, mucin depletion, granulomas, crypt abscesses, cryptitis and ulceration.11 ,34 ,50 However, these changes can also occur in other types of colorectal inflammation. Therefore, comparisons between IBD and other colitides, and especially infective colitis, are much more useful than comparisons with normal. It is also worth noting that normal histology does not exclude a clinicopathological diagnosis of IBD, especially in early disease or longstanding disease.
IBD versus acute infective colitis/acute self-limiting colitis/non-IBD colitis
Features favouring IBD over acute infective colitis/non-IBD
Comparisons in most reports are with acute infective colitis, acute infective-type colitis or acute self-limiting colitis, that is, diarrhoea (which may be bloody) and associated symptoms, lasting for a short time (eg, less than 1 month), not relapsing, and usually either demonstrably or presumably secondary to common infections such as Campylobacter, Salmonella, and Shigella.1 ,4 ,25 ,58 The main reason is that this is the closest clinical mimic of newly presenting IBD. Certain infections, for example, Clostridium difficile,1 HIV-related infections, tuberculosis (TB), amoebiasis and schistosomiasis have distinctive histological features and are generally excluded from these comparisons.
The observed discriminant value depends partly on the proportion of UC and CD cases in the IBD group in each study. Many of the features distinguishing IBD from infective or acute self-limiting colitis also distinguish IBD colitis from other types of non-IBD colitis.
The features favouring IBD over acute infective colitis are outlined in table 3. It is essential to take the clinical details into account at all times.
Features favouring IBD over acute infective colitis/acute self-limiting colitis
Features favouring infective colitis over IBD
In infective colitis it is common to see acute inflammatory changes, for example, cryptitis, crypt abscesses, lamina proprial neutrophils and oedema, especially in the early phase (up to 2 weeks).1 In one study, acute infective-type diarrhoea biopsied 1–10 weeks after onset typically showed mild lamina proprial hypercellularity, mainly in the upper two-thirds of the mucosa, with a slight increase in lamina proprial and crypt epithelial neutrophils.58 However, distinction from IBD relies mainly on the absence of features of IBD rather than on positive features of infection (table 4) (figure 3E).1 ,25 ,26 ,36 ,58 It is often more appropriate to suggest the diagnosis of infection than to make a definite statement.1
Features favouring infective colitis over IBD
IBD versus infective colitis: exceptions
There are several exceptions to the usual picture.
-
Crypt distortion occurs in a minority of infective colitides,18 ,26 ,33 ,59 particularly in the healing phase or if infection is severe or prolonged.4 ,11 ,59
-
A few infective colitis biopsies have basal plasmacytosis or other evidence of chronic inflammation.4 ,18 ,26
-
Crypt abnormalities may be absent from IBD biopsies, especially in early or treated disease.3 ,4 ,33 ,60
-
Some IBD biopsies have little or no basal plasmacytosis/chronic inflammation, particularly early in the course of disease or after treatment.3 ,18 ,26
Recommendations: IBD versus infection/non-IBD
-
The microscopic features that favour IBD over infective colitis include basal plasmacytosis and architectural changes (EL1a RGA).
-
Combinations of changes are more useful than single features.
-
Correlation with the clinical picture is essential.
UC versus CD: histology
Considerations
Even when a diagnosis of IBD is made confidently or favoured over other causes, further classification as UC or CD can be difficult. However, the distinction is very important for medical and surgical management. In particular, pouch surgery may be offered to patients with UC but is generally regarded as unsuitable for those with CD as they have a high risk of pouch failure.6 ,46 ,61 Accordingly, every effort to distinguish between these two forms of IBD should be made, especially in initial biopsies.15 Also, subclassification of IBD should be based on a combination of histological and clinical findings and not on microscopic changes alone.
Histological features which help discriminate UC from CD are outlined in tables 5 and 6.
Features favouring ulcerative colitis over Crohn's disease
Features favouring Crohn's disease over ulcerative colitis
Granulomas
Granulomas unrelated to crypt injury (non-cryptolytic granulomas) are very reliable for distinguishing CD from UC in a patient with new or established IBD, and are consistently more discriminant than any other single feature.5 ,30 ,63 ,65 ,66 However, they also occur in TB and, rarely, in other infective colitides.5 ,18 They are not, in isolation, diagnostic of CD. Granulomas in CD show no necrosis.5
Cryptolytic granulomas occur as a response to crypt injury and have been described in most colitides (including UC,5 ,29 infective colitis,26 diverticular colitis and diversion colitis) (figure 3A).67 Although there has been some dissent, they are generally regarded as non-discriminatory.29 ,67 Accordingly, crypt rupture should be excluded as a cause of granulomas, particularly if the evidence for CD is otherwise weak. Serial sections help define the relationship between granulomas and ruptured crypts (figure 3A) (EL5 RGD).18
Recommendations: subclassification of IBD and assessment of granulomas
-
The microscopic features that help distinguish UC and CD from one another include granulomas, architectural changes and distribution of disease (EL1a RGA).
-
Non-cryptolytic granulomas are more useful than any other feature for discriminating between CD and UC (EL1a RGA).
-
Cryptolytic granulomas occur in many colitides and probably have little or no discriminant value (EL4 RGC).
-
Isolated granulomas may merit serial sections to help define their relationship with ruptured crypts (EL5 RGD).
-
If granuloma formation is the sole abnormality, cautious interpretation is advised (EL5 RGD).
Assignment to a category: further considerations and summary
No histological feature is diagnostic of IBD or of a type of IBD. Instead, features are found to be more prevalent in one disease group than in another.
Diagnostic accuracy is optimised if several features rather than a single feature are assessed, if the distribution of changes is also analysed, and if the clinical details are considered. For example, a combination of diffuse architectural distortion, villous surface, crypt atrophy and basal plasmacytosis, especially if continuously distributed within and between sites, is essentially diagnostic of UC in the appropriate clinical setting,3 while segmental involvement of multiple site biopsies together with variable chronic inflammation and crypt changes within sites accompanied by non-cryptolytic granulomas is virtually diagnostic of CD.
A minimum number of histological features required for a particular diagnosis is not definable.3 ,36
Severity of changes may also be important. For example, severe crypt changes are more characteristic of UC than of CD while mild crypt changes are less discriminant. However, published data is sparse.
Features typically used to distinguish IBD from non-IBD/infective colitis and to distinguish UC from CD when examining an initial biopsy are summarised in table 7.
Some features which may be useful for initial diagnosis and classification of IBD
Recommendations: assignment to a category on the basis of histology
-
No histological feature is diagnostic in isolation of IBD or of a subtype of IBD. Instead, certain features are more prevalent in one disease group than in another.
-
Diagnostic accuracy is optimised if multiple features are assessed together, if the intersite and intrasite distribution of changes is also analysed, and if the clinical details are taken into account.
Frequency and reproducibility
Frequency
Pathologists should be aware of the frequency of various features in different settings and should also bear in mind the reproducibility of each feature. The published prevalence of each histological feature in various settings is shown in table 8.
Reported frequencies of histological features in initial biopsies (%)
Interobserver agreement and reproducibility
Interobserver variability is often high, both for the presence of abnormal features and for disease classification.11
Agreement for individual histological features
Compared with most other features, there is consistently good interobserver agreement for identification of granulomas and giant cells (table 9). There is also good agreement for the presence of basal plasmacytosis and for distinguishing focal from diffuse chronic inflammation. There is more variability in the assessment of architecture, mucin depletion and Paneth cell metaplasia.11 ,30
Reproducibility of some histological features
Agreement for category of disease
Histopathologists are better at distinguishing IBD from non-IBD than distinguishing UC from CD (EL2b RGB).11 ,50 ,68 Also, agreement for diagnosing UC is better than for diagnosing CD (EL2b RGB).11 ,36 ,69 Underdiagnosis of CD by histopathologists is a recognised problem. However, it is likely that the accuracy and confidence of interpretation of IBD biopsies is improved if there is careful correlation with clinical and endoscopic findings (EL2b RGB),11 ,13–15 ideally supplemented by discussion at a regular multidisciplinary meeting (EL5 RGD).
Recommendations: frequency and reproducibility
-
In addition to knowing the discriminant value of each feature, pathologists should be aware of its frequency and reproducibility. This should help optimise the accuracy of interpretation and categorisation.
-
Correlation with clinical findings and discussion at a dedicated clinicopathological meeting should help consensus to be reached if there is initial disagreement.
Effects of time and treatment
Time-related changes in untreated IBD
The likelihood of observing various histological features in newly diagnosed IBD changes with the duration of symptoms. Focal basal plasmacytosis, probably the earliest abnormality,4 can be seen in the first 15 days of symptoms (table 10). It becomes more extensive and more prevalent with time (EL1b RGB).4 Architectural changes typically develop later. For example, crypt distortion is not seen before 15 days of symptoms but is present in more than 75% of patients after 4 months (table 10) (EL1b RGA).4 ,11 ,47 ,60
Time-related changes in untreated IBD
Most adult patients present after at least 6 weeks of symptoms.28 Therefore, ‘chronic’ histological features are usually discernible at initial diagnosis.4
Treated/longstanding IBD: changes in histology, extent and distribution
Follow-up biopsies may confirm or refine a diagnosis of IBD.3 However, treatment modifies IBD histology. Treatment effect is unpredictable, depends partly on disease duration and initial intensity of inflammation,45 ,47 and cannot be distinguished reliably from chronic time-related changes.
Basal plasmacytosis may diminish in longstanding/treated disease,3 while crypt changes are more likely to persist.4 Paneth cell metaplasia appears to be a feature of longstanding disease. Lamina proprial fibrosis may be seen. In some patients, abnormal mucosa reverts to normal.35
Extent and distribution can also vary with time and treatment (EL2a RGB) (see section on Distribution, extent and activity).5 ,39 ,42 Rectal sparing, discontinuity between sites, and patchy or focal changes within sites are recognised features of longstanding UC and are not sufficient for a change of diagnosis. They may be enhanced by medical therapy (EL2a RGB),17 ,28 ,39 ,45 ,47 ,70 but the type of medication does not correlate with the prevalence of rectal sparing or discontinuity.17 ,40 ,65
Certain drugs have specific effects. 5ASA and topical steroids may be associated with normalisation of mucosa in some patients with UC.47 Granulomas may diminish in number after some types of treatment.47 Cyclosporine may cause dysplasia-like changes.71 Recent clinical trials have documented histological changes after treatment with specific agents.57 ,72
Recommendations: effects of time and treatment
-
Early untreated IBD may show few or no histological changes. There is some correlation between the onset of each abnormality and duration of symptoms. Basal plasmacytosis is the earliest feature. Crypt changes typically appear later (EL1b RGB).
-
Time and treatment may modify the histology, distribution and extent of IBD (EL2a RGB). Longstanding UC not infrequently shows patchiness, discontinuity and/or rectal sparing.
-
Interpretation of biopsies from early or longstanding IBD should be cautious (EL2a RGB).
-
Modification of an established diagnosis of UC or CD should only be made if there is convincing evidence for a change, ideally after review of previous histology and of clinical data in a multidisciplinary setting.39
Paediatric UC
Considerations
UC in children and adults differs slightly (table 11). Children may have a higher prevalence of discontinuous disease, rectal sparing and pancolitis, and a lower prevalence of ‘chronic’ histological changes28 ,38 ,48 ,73 (possibly because of earlier presentation)28 although not all reports agree that rectal sparing is more common. Discrepancies with adult disease may be greater in those aged <11 years than in those aged 11–17 years.31 As in adults, discontinuous disease and absence of crypt changes should not cause UC to be excluded (EL1b RGB).3 ,48 Upper gastrointestinal involvement by IBD appears to be more prevalent in children than in adults (see section on Ileal and upper gastrointestinal biopsies).73
Differences between adults and children with ulcerative colitis
Recommendations: paediatric IBD
-
The histology of paediatric IBD is similar to that of adult disease.
-
Compared with adult disease, the prevalence of ‘chronic’ changes in paediatric UC may be lower, and the prevalence of patchy/discontinuous changes higher (EL2b RGB).
-
Upper gastrointestinal involvement may be more common in children than in adults.
Ileal and upper gastrointestinal biopsies
Ileal biopsies in IBD
Occasionally, there is distal terminal ileal inflammation in UC. Despite being attributed to ‘backwash’, it is not always accompanied by caecal involvement.39 ,52 Villous atrophy, mixed lamina proprial inflammation, cryptitis, crypt abscesses and focal erosion may be seen.3 ,52 Non-cryptolytic granulomas are not observed.65 Pyloric metaplasia (mucous gland metaplasia) can occur, but is not common.52
Terminal ileal mucosa is abnormal in most patients with CD.64 Features include disturbed villous and crypt architecture, focal or patchy inflammation, focal erosions and pyloric metaplasia.3 ,74 Granulomas and giant cells are uncommon but are useful for discriminating Crohn's ileitis from ileal UC.64
Upper gastrointestinal biopsies in IBD
Microscopic upper gastrointestinal tract inflammation is quite common in CD76 and comparatively rare in UC.77 However, upper gastrointestinal involvement by UC may be more common in children than in adults.73
Gastric granulomas occur in 0–83% of CD, depending on study design.76 ,78 Granulomas at any site strongly favour CD over UC. However, they are not diagnostic of CD in isolation, as there are many other possible causes.76
Duodenal involvement is not uncommon in CD but is also seen in a few UC patients77 ,79 whose biopsies may show a pattern of diffuse chronic inflammation and crypt changes resembling the colorectal abnormalities.77
‘Focally enhanced gastritis’,77 ,80 characterised by a focal mixed perifoveolar/periglandular inflammatory infiltrate with epithelial damage, was first reported as a feature of CD,5 ,75 ,81 but is not specific,5 ,65 ,77 ,82 and can also be seen in UC.77 ,83 Helicobacter pylori infection should always be excluded if there is gastric inflammation, even if a patient is known to have IBD.
Oesophageal involvement can be attributed to known CD if there are granulomas. Otherwise, gastro-oesophageal reflux and other causes should be excluded.84 Lymphocytic oesophagitis has also been described in Crohn's patients.84 Oesophageal involvement by UC is probably very rare.77 ,78
Upper gastrointestinal inflammation may raise the possibility of a new diagnosis of CD but is rarely diagnostic in isolation.5 ,76 UC should not be diagnosed on the basis of upper Gastrointestinal (GI) tract abnormalities.77
Recommendations: upper gastrointestinal biopsies in IBD
-
Upper gastrointestinal involvement by CD is considerably more frequent than involvement by UC (EL4 RGC).
-
Other more common causes of upper gastrointestinal inflammation, especially gastro-oesophageal reflux and H pylori-associated gastritis, should be excluded before involvement by IBD is suggested (EL5 RGD).
-
In the setting of IBD, upper gastrointestinal granulomas strongly favour CD over UC (EL4 RGC).78
-
Upper gastrointestinal granulomas may raise the possibility of new CD, but caution is advised (EL5 RGD).
Mimics of IBD
Considerations
Several entities can mimic IBD histologically (table 12). The possibility of an alternative cause should be considered, especially when clinical details are limited.
Histological mimics of IBD
Diversion proctocolitis
After colonic resection, the faecal stream may be diverted. The excluded large bowel may develop diversion proctocolitis (DPC) which can show a variety of histological mucosal abnormalities including patchy or diffuse lamina proprial chronic inflammation, prominent lymphoid follicles, crypt distortion, crypt atrophy, and aphthous or non-aphthous ulcers, thus sometimes resembling IBD (figure 3F).85–88 The changes can be attributed entirely to diversion if there is no prior history of colorectal inflammatory disease. However, in patients with pre-existing IBD, the features of DPC and IBD overlap and are difficult to separate from one another.
In diverted UC, inflammation is typically severe, while CD mucosa may improve after diversion.86 However, histological features in biopsies (and resections) from a diverted segment do not distinguish reliably between UC and CD. For example, granulomas in DPC may be more common when the underlying pathology is CD than when it is UC,89 but can also occur in the latter and in other settings.87 ,90
Microscopic colitis
The term ‘microscopic colitis’ is qualified as collagenous colitis or lymphocytic colitis, if possible.91 Collagenous colitis is characterised by a thickened subepithelial collagen band (>15 µm)92 and a variable, often mild, increase in intraepithelial lymphocytes.93 Lymphocytic colitis requires an increase in intraepithelial lymphocytes (>20 per 100 epithelial cells).94 Surface epithelial degeneration and an increase in lamina proprial plasma cells occur in both.92 ,95 Very rarely, there are subepithelial multinucleate giant cells.96 There is usually no endoscopic abnormality.92
Collagenous and lymphocytic colitis may show basal plasmacytosis (figure 3G), raising the possibility of IBD (EL2b RGC).21 ,93 However, other features of IBD, particularly crypt distortion, are usually absent (EL1a RGA).93 ,97 Conversely, early IBD with mild intraepithelial lymphocytosis and preserved architecture could resemble microscopic colitis.21 There are a few reports of a microscopic colitis-type picture in IBD or prior to its onset.98 ,99
Diverticular colitis
Diverticular colitis (diverticular disease-associated colitis; isolated sigmoiditis) refers to mucosal changes in the segment affected by diverticula, usually the sigmoid colon. In biopsies, lamina proprial plasmacytosis, cryptitis and crypt abscesses are usual (figure 3H). Crypt distortion is typically present though not severe. Basal plasmacytosis and Paneth cell metaplasia are also quite common. Villous surface change and non-cryptolytic granulomas are rare.27 ,100
Histologically, diverticular colitis can resemble IBD closely (EL4 RGC).26 ,27 ,101 Misdiagnosis as UC is a recognised problem (EL5 RGD).26 Assessment of biopsies from both the sigmoid colon and the rectum is helpful (EL4 RGC).27 ,102 Resemblance to CD can also occur, especially in resections.103 Some authors have distinguished ‘segmental colitis associated with diverticulosis (SCAD)’, which often resembles IBD, from diverticulitis (ie, inflammation extending directly from diverticular mucosa into the adjacent mucosa), and have subcategorised it, for example, crescent fold disease, UC-like, and Crohn's colitis-like.104 Also, IBD seems particularly likely to develop in diverticular segments in patients who have both IBD and diverticular disease.105 Accordingly, the relationship between IBD and diverticular disease is not straightforward.
Radiation colitis
Radiation therapy can cause a chronic colitis with crypt atrophy, crypt distortion and mucin depletion, potentially resembling IBD (EL3b RGC).21 ,35 ,102 Other features, including hyalinisation, fibrosis and vascular ectasia and absence of basal plasma cells, help make the distinction,15 ,21 ,35 but diagnosis depends on a clinical history.
Ischaemic colitis
Ischaemic colitis may overlap with IBD clinically. Microscopically, chronic ischaemia can cause crypt atrophy and distortion (EL3b RGC).21 ,35 ,65 ,102 Basal plasma cells are absent or sparse. Mild acute inflammation, hyalinisation of the lamina propria, and fibrosis are typical.15 ,21 Extensively damaged crypts may be represented by deeply located aggregates of neuroendocrine cells.35 The clinical picture and anatomical distribution help make the distinction from IBD.15 ,35
Graft-versus-host disease
Acute graft-versus-host disease (GVHD) can cause crypt atrophy and distortion, but chronic inflammation is absent or mild and crypt epithelial cell apoptoses are usual. Chronic GVHD may also result in crypt distortion and atrophy, with or without fibrosis.35 After substantial epithelial loss, endocrine cells may be the only sign of a pre-existing crypt.106
Mass lesion
The mucosa overlying an intramural or subserosal mass (eg, diverticular disease, carcinoma, endometriosis) may show features reminiscent of IBD, including lamina proprial chronic inflammation and crypt distortion.107 Granulomas are less common (EL2b RGC).107
Infections
HIV
Colorectal biopsies from HIV-positive patients with chronic diarrhoea often reveal no pathogen but may show mild chronic inflammation, lymphoid aggregates, lymphoid follicles and crypt epithelial cell apoptoses.108 The picture can closely resemble IBD, especially CD, but crypt distortion is uncommon.35 ,109 Some cases may be secondary to lymphogranuloma venereum (LGV) (see below).110 The label ‘Crohn's disease’ is not recommended for HIV-related IBD-like changes.
Lymphogranuloma venereum and syphilis
Chronic LGV-related and syphilitic proctocolitis may be similar to one another histologically and can both resemble IBD, particularly CD.110 ,111 The rectum is most commonly involved and is typically most severely affected, but any part of the colon can be inflamed.111 ,112 Most patients are HIV-positive men who have sex with men.111 Histological changes include a prominent lymphohistiocytic and plasma cell infiltrate, fibrosis, relatively mild acute inflammation and minimal basal plasmacytosis or crypt distortion.35 ,111 Granulomas and Paneth cell metaplasia can occur but are not common.35 ,111 ,113 Reliable distinction from IBD depends on the clinical setting, although the diagnosis is often unsuspected at endoscopy.111
Yersinia and TB
Yersinia and TB can elicit granulomas, occasionally cause crypt distortion, and may mimic CD.59 ,114 Caseous necrosis and demonstrable acid fast bacilli indicate TB but are confined to a minority of cases. TB is favoured over IBD by confluent granulomas, numerous granulomas, Langhans giant cells, a lymphoid cuff around granulomas, and granulomas more than 400 μm in diameter.115 Yersinia is favoured over IBD by granulomas with central necrosis, granulomas surrounded by a lymphoid cuff, and stellate abscesses.59 ,114
Other infections
Amoebic colitis if prolonged can cause crypt distortion but tends to lack other features of IBD.59 This and other protozoan infections can coexist with IBD and worsen disease activity.116 Schistosomiasis can elicit granulomas.35 These conditions are obvious if micro-organisms are seen. Chronic infection with Clostridium difficile is a recognised cause of crypt architectural changes.88 The clinical setting is very important.
Drugs
Drugs should always be considered, especially if a colitis has unusual features. Non-steroidal anti-inflammatory drug (NSAID) colitis has a wide spectrum of presentations and can occasionally cause crypt distortion, IBD-like changes, and even granulomas; clues to the cause include epithelial cell apoptoses and increased intraepithelial lymphocytes.101 ,117 Mycophenolate Mofetil colitis may resemble IBD with crypt architectural changes and chronic inflammation, but more commonly mimics GVHD.118
Other potential mimics of IBD
Mucosal prolapse
Mucosal prolapse may cause distortion of crypts, potentially resembling IBD. Other features of prolapse, such as vertical smooth muscle fibres and ‘diamond-shaped’ crypts, help make the distinction, while basal plasma cells are not usually present.88 ,119
Behcet's disease
Behcet's disease rarely involves the colon. It typically causes ulcers and preferentially affects the ileocaecal region. It can mimic IBD (particularly CD) clinically. There are few descriptions of the histological changes, but lymphoid aggregates may occur and granulomas are unusual.120 ,121
Autoimmune enteropathy
Autoimmune enteropathy is a rare entity which may involve the large bowel and cause IBD-like changes, particularly lamina proprial chronic inflammation.122 ,123
Common variable immune deficiency
Common variable immune deficiency (CVID) can cause crypt distortion, granulomas and acute inflammation, and may sometimes mimic IBD clinically and histologically. The hallmark feature of sparse or absent lamina proprial plasma cells is not universal.124
Focal active colitis
The histological pattern of ‘focal active colitis’, characterised by focal cryptitis or crypt abscess formation in the absence of other changes, is not specific and may represent IBD, infection, ischaemia, drugs (especially NSAIDs) or other causes.59 ,125 ,126 It should not be regarded as a diagnosis. If this pattern is seen, the possibility of underlying IBD and other causes should be mentioned.
Ileoanal pouch biopsies
Biopsies from an ileal pouch anal anastomosis are taken for various reasons, for example, to assess severity of inflammation, seek evidence of IBD, exclude other conditions, such as Cytomegalovirus (CMV), or exclude dysplasia. Rectal/columnar cuff (distal pouch) biopsies may also be taken. Adaptive changes, including villous atrophy and a colorectal phenotype, are common.127 Inflammation is frequent, and a diagnosis of ‘pouchitis’ should not be based solely on histology.127 Histological inflammatory scoring schemes may be useful clinically and as a guide for the pathologist.127–129 Identification or subclassification of IBD is difficult because changes resembling those of IBD, particularly CD, can occur for other reasons in this setting.127 Misinterpretation may occur if clinical details are suboptimal.
Recommendations: mimics of IBD
-
There are numerous histological mimics of IBD (EL1b RGA).
-
Diverticular colitis and Diversion proctocolitis may closely resemble IBD.
-
A full clinical and endoscopic history is necessary before the histological mimics of IBD can be excluded confidently.
Terminology
Considerations
Some terms are ambiguous or can cause confusion. They are often avoidable (table 13).
Some terms which may cause problems
Colitis
This word may mean UC to clinicians and inflammation of the colon to histopathologists. Qualification is essential so that the conclusion ‘colitis’ is not misinterpreted as meaning UC, with possible serious consequences.
‘Non-specific colitis’ and ‘non-specific chronic colitis’
These terms may be misconstrued by clinicians as diagnoses91 and should be avoided. Mild crypt changes and borderline inflammation can occur in various circumstances.91 A description can be made, and the lack of specificity noted.
IBD unclassified, ‘indeterminate colitis and colitis of undetermined type/etiology’
Distinction between UC and CD is sometimes impossible. Treatment may exacerbate the problem.61 The label ‘indeterminate colitis’ has been used for resection specimens with definite IBD in which further classification is not appropriate.3 ,7 ,65 ,130 ,131 Unfortunately, the term has caused confusion and has often been used incorrectly to mean ‘colitis, cause unknown’ or to describe a non-existent intermediate category between UC and CD.3 ,7 ,11 ,13 ,37 ,61 ,65 ,88 ,130 ,132 The term ‘colitis of undetermined type/etiology’ (CUTE) has also been suggested. Both terms are best avoided by histopathologists, and are certainly not used for biopsy diagnosis. The designation ‘IBD unclassified (IBDU)’ is recommended as it states unequivocally that the disease is IBD.6 ,7 If there is uncertainty about the presence of IBD, this should be made clear.
Microscopic colitis
This term has sometimes been used inappropriately for any form of histological inflammation occurring in the absence of endoscopic or radiological abnormalities, and might then encompass some examples of IBD. This usage is not recommended.
Probability
Histopathologists use various terms to express probability (see also section on Reporting scheme for IBD biopsies (PAID)). The terms ‘in keeping with’, ‘consistent with’ and ‘compatible with’ are convenient, but may cause misunderstandings with clinicians and with other pathologists.133 To many pathologists they convey at least some degree of diagnostic uncertainty. These terms should not be used for dysplasia or malignancy.
Unfortunately, there are no universally agreed terms to describe the various levels of certainty or uncertainty encountered by histopathologists and clinicians, unless the diagnosis is definite.133 Discussion of difficult cases with clinicians, ideally in the setting of clinicopathological meetings, should reduce the risk of terminological (and other) misunderstandings.133
Recommendations: terminology and IBDU
-
IBD should be subcategorised as UC or CD, or a preference for one of these diagnoses expressed.
-
The term ‘IBD unclassified’ is recommended when IBD cannot be classified further.
-
Clinicopathological meetings may improve the accuracy and precision of IBD diagnosis (EL5 RGD). Discussion of IBD cases which at first cannot be subcategorised may allow a preference to be expressed.
-
The term ‘indeterminate colitis’ is not used for biopsy reporting and is best avoided.
-
The term ‘CUTE’ should not be used.
-
The terms ‘non-specific colitis’ and ‘non-specific chronic colitis’ should not be used.
-
Caution is recommended when using terms such as ‘in keeping with’.
Dysplasia
Clinical considerations
Dysplasia is a marker for future and underlying malignancy.65 ,134 Pancolonic dye spraying with targeted biopsies of macroscopically abnormal areas is recommended in clinical guidelines. If this is not possible, the colon is biopsied randomly; recommendations include 2–4 biopsies per site at 100 mm intervals.5 ,12 However, evidence helping to determine the ideal number is sparse.
Diagnosis of dysplasia
Diagnosis of dysplasia depends on atypical architecture (eg, crowding of glands) and cytology (eg, nuclear hyperchromasia, pseudostratification, enlargement, pleomorphism and loss of polarity).5 ,88 ,135 Typically, dysplasia extends to the mucosal surface (EL5 RGD)65 ,88 ,101 while regenerative changes do not.
Dysplasia in IBD often resembles that seen in colorectal adenomas.101 The epithelium in IBD-associated dysplasia is sometimes serrated.35 ,101 Inflammatory polyps occasionally develop foci of dysplasia (EL5 RGD).101
The term ‘indefinite for dysplasia’ may be appropriate if a decision cannot be made as to the presence of dysplasia for any reason, for example, atypical changes in the setting of inflammation.65 ,135 It is not an intermediate category between negative for dysplasia and low-grade dysplasia. If used, it should be qualified in the text of the conclusions. Sometimes, a description is preferable to this category. Further biopsies should be advised.
Low-grade dysplasia versus high-grade dysplasia
Architecture and cytology both help categorise dysplasia, and some authors rely on one or the other rather than both.9 ,101 The UK bowel cancer screening pathology guidelines emphasise architecture.9 Cytological features favouring high-grade dysplasia over low-grade dysplasia include nuclei in the upper half of a cell and complete loss of nuclear polarity.35 ,88 ,101 Nuclei tend to be larger, more hyperchromatic, more stratified and round or ovoid rather than ‘pencil shaped’. Mitoses are more numerous and nucleoli more prominent. Architectural changes are also more severe, with cribriform areas.35 ,88 To be classified as having high-grade dysplasia a lesion should have at least a few crypts with high-grade changes, but the proportion required for a final diagnosis of high-grade dysplasia has not been agreed.9 ,88 The term ‘carcinoma in situ’ is not recommended.
DALM versus adenoma
The management of localised dysplastic lesions depends on their endoscopic features and resectability, and on whether they are located within or outside the area affected by IBD, rather than on categorisation of a polyp as a ‘sporadic’ adenoma or an IBD-associated dysplastic lesion. Furthermore, histology does not distinguish reliably between the latter two diagnoses. However, documentation of dysplasia in the perilesional mucosa is very important because it governs management after polypectomy.5 ,12 ,88
Dual reporting of dysplasia
Interobserver variability for the diagnosis and grading of gastrointestinal dysplasia is a recognised problem.101 ,134 ,136 Biopsies should ideally be reported by more than one histopathologist (EL5 RGD)5 ,8 although there is conflicting evidence as to the clinical benefits of this approach.5 ,134 Distinction between low grade and high grade influences the management of flat dysplasia. The recent trend towards primary local endoscopic resection of all visible and well-delineated dysplastic lesions (with histological confirmation of margins) has meant that grading of dysplasia in such lesions is assuming less importance for the management of many cases.12
Additional techniques for diagnosing dysplasia
Reliance on additional techniques such as mucin stains and immunohistochemistry to help diagnose or grade dysplasia is not currently recommended. Nevertheless, they may sometimes provide corroboration of a diagnosis of dysplasia (EL5 RGD).5 ,8 ,101
Recommendations: dysplasia
-
Diagnosis and grading of dysplasia relies on architecture and cytology.
-
Dysplasia is graded as low grade or high grade.
-
The term ‘indefinite for dysplasia’ can be used when distinction between dysplastic and non-dysplastic atypia is not possible.
-
Double reporting of cases with dysplasia or suspected dysplasia is recommended (EL5 RGD).
Reporting scheme for IBD biopsies (PAID)
Approach and suggested scheme
The acronym ‘PAID’ is a suggested aide memoire for the layout of the conclusion to an IBD biopsy report (table 14).
- P
- Pattern: of chronic changes: presence, distribution, extent
- A
- Activity: maximum grade, location
- I
- Interpretation: probability of IBD and, if relevant, probability of UC or CD
- D
- Dysplasia: location, severity
‘PAID’ scheme for summarising IBD biopsy histology
The suggested scheme represents a consensus opinion between the author, the BSG pathology section, and reviewers acting on behalf of the BSG IBD section, the BSG Central Services and Standards Committee, and the BSG Council (EL5 RGD).
Codes may be useful, and a scheme for these is also suggested.
The suggested proforma in the section on The ‘PAID’ scheme: proforma and text-based summaries, based on the PAID scheme in table 14, may serve as an aide-memoire or have other uses, for example, teaching and audit.
Probability
Clinicians often ask for a comment on the probability of a diagnosis (table 14). It is reasonable to attempt this, within the limitations of the perspective of the histopathologist. As noted above, ideal terms are difficult to find. Sometimes, the histology is highly characteristic and almost diagnostic in isolation, that is, the word ‘definite’ might be used (assuming that the histology fits with the clinical picture). Alternatively, the features could be strongly suggestive/supportive of a new diagnosis or highly supportive of a known diagnosis, in which case the diagnosis is ‘very likely’. From a management point of view these two categories are similar and are combined in the scheme. If the features are less convincing but still allow one diagnosis to be preferred, the term ‘favoured’ is suggested.
Clinicopathological correlation
In this scheme, the histopathological findings are interpreted in the context of the clinical picture. If necessary, final classification should be delayed until discussion with clinicians has taken place.
Recommendations: structured approach to conclusion (‘PAID’ scheme)
-
A structured approach to the conclusion of an IBD biopsy report is recommended. This should include comments on the Pattern of changes, Activity, Interpretation and Dysplasia. The acronym ‘PAID’ can be used as an aide-memoire.
The ‘PAID’ scheme: proforma and text-based summaries
Reporting scheme (PAID): text-based summaries
The dataset proforma (above) can be used to summarise the findings. Alternatively, text conclusions might be structured as in the following examples.
Initial biopsies
Rectal bleeding. Colonoscopic biopsies.
- P
- Diffuse chronic colitis involving sigmoid colon and rectum
- A
- Mild activity, rectum
- I
- IBD, strongly favouring UC over CD
- D
- No dysplasia
Histology codes. A1; IBD-DVL UC-DVL; D0
Abdominal pain. Colonoscopic biopsies.
- P
- Patchy chronic colitis from caecum to transverse colon with minimal rectal inflammation
- A
- Severe activity, caecum and ascending colon; mild activity elsewhere
- I
- Features strongly suggestive of IBD, favouring CD over UC
- D
- No dysplasia
Histology codes. A3; IBD-DVL CD-F; D0
Follow-up biopsies
The PAID approach can also be used for follow-up biopsies, with some modifications. A statement of the level of support for the established diagnosis is often useful.
UC for 10 years. Left colonic and rectal biopsies.
- P
- Chronic colitis involving sigmoid and rectum
- A
- Mild activity, sigmoid and rectum
- I
- The histological features are those of IBD and strongly favour the known diagnosis of UC over CD
- D
- No dysplasia
Histology codes. A1; IBD-DVL UC-DVL; D0
Known IBD, unclassified. Ileal, colonic and rectal biopsies.
- P
- Patchy chronic colitis involving all sites, with granulomas
- A
- Mild activity in caecum and rectum
- I
- The features are those of the known diagnosis of IBD and favour CD over UC
- D
- Low-grade dysplasia, rectum
Histology codes. A1; IBD-DVL CD-F; DL
Key recommendations
Clinical considerations
-
Accurate histopathological assessment is important for optimum diagnosis, subclassification and management of IBD.
-
Biopsies for the diagnosis of IBD should be accompanied by a record of endoscopic findings and by a full clinical history, including duration of disease and details of treatment (EL2a RGB).
-
A regular clinicopathological meeting for discussion of IBD cases should be available.
Distribution and extent of disease
-
Distribution of microscopic changes within biopsies, between biopsies and between sites should be assessed (EL1b-2b RGB).
-
The terms ‘diffuse’, ‘patchy’ and ‘focal’ can be used for distribution within sites.
-
The terms ‘continuous between sites’ and ‘discontinuous between sites’ (or its synonym ‘segmental’) can be used for distribution between sites.
-
There are several exceptions to the typical continuous distribution of UC, even at initial presentation (EL1a RGA), that should not necessarily prompt a change of diagnosis. These include a caecal patch and rectal sparing.
IBD versus infection/non-IBD
-
The microscopic features that favour IBD over infective colitis include basal plasmacytosis and architectural changes (EL1a RGA).
Subclassification of IBD and assessment of granulomas
-
The microscopic features that help distinguish UC and CD from one another include granulomas, architectural changes and distribution of disease (EL1a RGA).
-
Non-cryptolytic granulomas are more useful than any other feature for discriminating between CD and UC (EL1a RGA).
-
Cryptolytic granulomas occur in many colitides and probably have little or no discriminant value (EL4 RGC).
-
Isolated granulomas may merit serial sections to help define their relationship with ruptured crypts (EL5 RGD).
-
If granuloma formation is the sole abnormality, cautious interpretation is advised (EL5 RGD).
Assignment to a category on the basis of histology
-
No histological feature is diagnostic in isolation of IBD or of a subtype of IBD. Instead, certain features are more prevalent in one disease group than in another.
-
Diagnostic accuracy is optimised if multiple features are assessed together, if the intersite and intrasite distribution of changes is also analysed, and if the clinical details are taken into account.
Effects of time and treatment
-
Early untreated IBD may show few or no histological changes. There is some correlation between the onset of each abnormality and duration of symptoms. Basal plasmacytosis is the earliest feature. Crypt changes typically appear later (EL1b RGB).
-
Time and treatment may modify the histology, distribution and extent of IBD (EL2a RGB). Longstanding UC not infrequently shows discontinuity and/or rectal sparing.
-
Interpretation of biopsies from early or longstanding IBD should be cautious (EL2a RGB).
-
Modification of an established diagnosis of UC or CD should only be made if there is convincing evidence for a change, ideally after review of previous histology and of clinical data in a multidisciplinary setting.
Paediatric IBD
-
The histology of paediatric IBD is similar to that of adult disease.
-
Compared with adult disease, the prevalence of ‘chronic’ changes in paediatric UC may be lower and the prevalence of patchy/discontinuous changes higher (EL2b RGB).
Ileal biopsies
-
In the setting of IBD, ileal inflammation strongly favours CD over UC (EL1b RGB).
-
Granulomas (non-cryptolytic) in inflamed ileal biopsies help discriminate CD from UC (EL1b RGB). Few other features are useful.
Upper gastrointestinal biopsies
-
Upper gastrointestinal involvement by CD is considerably more frequent than involvement by UC (EL4 RGC).
-
Other more common causes of upper gastrointestinal inflammation, especially gastro-oesophageal reflux and H pylori-associated gastritis, should be excluded before involvement by IBD is suggested (EL5 RGD).
-
In the setting of IBD, upper gastrointestinal granulomas strongly favour CD over UC (EL4 RGC).
-
Upper gastrointestinal granulomas may raise the possibility of new CD, but caution is advised (EL5 RGD).
Mimics of IBD
-
There are numerous histological mimics of IBD (EL1b RGA).
-
Diverticular colitis and diversion proctocolitis may closely resemble IBD.
-
A full clinical and endoscopic history is necessary before the histological mimics of IBD can be excluded confidently.
Terminology and IBDU
-
IBD should be subcategorised as UC or CD, or a preference for one of these diagnoses expressed.
-
The term ‘IBD unclassified’ is recommended when IBD cannot be classified further.
-
Clinicopathological meetings may improve the accuracy and precision of IBD diagnosis (EL5 RGD). Discussion of IBD cases which at first cannot be subcategorised may allow a preference to be expressed.
-
The term ‘indeterminate colitis’ is not used for biopsy reporting and is best avoided.
-
The term ‘CUTE’ should not be used.
-
The terms ‘non-specific colitis’ and ‘non-specific chronic colitis’ should not be used.
-
Caution is recommended when using terms such as ‘in keeping with’.
Dysplasia
-
Diagnosis of dysplasia relies on architecture and cytology.
-
Dysplasia is graded as low grade or high grade.
-
The term ‘indefinite for dysplasia’ can be used when distinction between dysplastic and non-dysplastic atypia is not possible.
-
Double reporting of cases with dysplasia or suspected dysplasia is recommended (EL5 RGD).
Structured approach to conclusion: ‘PAID’ scheme
-
A structured approach to the conclusion of an IBD biopsy report is recommended. This should include comments on Pattern of changes, Activity, Interpretation and Dysplasia. The acronym ‘PAID’ can be used as an aide-memoire.
Acknowledgments
The author is very grateful to Professor Neil Shepherd for consistent support and encouragement; to Dr Adrian Bateman for much practical assistance; and to Professor Geraint Williams, Dr Chris Probert, Dr Norman Carr, Dr Philip Kaye, Dr Newton Wong, and other unnamed reviewers for their valuable comments on the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendices
Footnotes
-
Correction notice This paper has been corrected since it was published online. Table 14 and the PAID Scheme table have been reformatted for clarity.
-
Competing interests None
-
Provenance and peer review Not commissioned; internally peer reviewed.