Article Text

Abstract
Aims A severe syndrome characterised by life-threatening diarrhoea and severe sprue-like histology has been described in patients taking the angiotensin receptor blocker (ARB) olmesartan. It is unknown whether there are any histopathological changes in patients without severe diarrhoea exposed to this medication. It is also unknown whether other ARBs cause sprue-like histology.
Methods Retrospective cohort study of patients with abdominal pain undergoing upper gastrointestinal endoscopy with duodenal biopsy who were taking ARBs. Patients taking olmesartan (n=20) and a non-olmesartan ARB (n=20) were compared with age and sex-matched controls. Histological features (classic sprue-like and other inflammatory changes) were analysed.
Results No single histopathological finding was significantly more common in olmesartan-using patients than controls. However, 10 of 20 olmesartan patients had one or more sprue-like histological features compared with 4 of 20 age-matched and sex-matched controls not taking ARBs (p=0.10). Patients taking ARBs other than olmesartan were not more likely than controls to have one or more of these sprue-like histological features (9/20 vs. 12/20, p=0.34).
Conclusions There were no statistically significant differences between olmesartan users with abdominal pain and controls for any single histopathological abnormality. However, there were trends towards significance for individual abnormalities as well as for a composite outcome of sprue-like changes. This raises the possibility that there is a spectrum of histological changes associated with olmesartan use.
- SMALL INTESTINE
- INFLAMMATION
- GUT PATHOLOGY
- GASTROINTESTINAL DISEASE
Statistics from Altmetric.com
Introduction
Olmesartan medoxomil is a commonly used antihypertensive medication, which acts by blocking angiotensin receptors. Recently, a series of cases were described in which 22 patients presented with debilitating diarrhoea and had a sprue-like enteropathy on histological examination due to olmesartan. The diarrhoea was so severe that 14 patients required hospitalisation and 4 required total parenteral nutrition. Serological testing for coeliac disease was negative in all cases and none improved with a gluten-free diet. All had biopsies, which showed severe sprue-like changes (villous atrophy, lamina propria inflammation and intraepithelial lymphocytosis (IEL)). Seven of the patients had collagenous sprue. All patients had dramatic improvement, with resolution of their diarrhoea following cessation of olmesartan.1 As a major referral centre for coeliac disease, we have subsequently encountered a number of such cases and several other case series and reports have been published, which demonstrate similar clinical and histopathological findings.2–12 At present, this adverse drug reaction is thought to be a rare occurrence. A recent case–control study did not show an association between olmesartan use and chronic diarrhoea in patients presenting for oesophagogastroduodenoscopy (OGD) or colonoscopy.13
While it is unusual to encounter severe villous atrophy in non-coeliac patients, milder changes which may overlap with sprue-like enteropathies (such mild or focal IEL) are common.2 ,14 Medication reactions, particularly non-steroidal anti-inflammatory drugs, are commonly listed in the differential of such pathological findings.15 Other drugs also enter the differential, but it is unknown whether olmesartan exposure should be considered when encountering such findings. It is also unknown whether other angiotensin receptor blockers (ARBs) may cause histopathological changes.
Because it is unclear whether the severe sprue-like enteropathy seen in a few patients taking olmesartan is the severe end of a spectrum of intestinal injury, we identified patients taking olmesartan who had undergone endoscopy for abdominal pain with duodenal biopsy and systematically studied the biopsies. We also identified patients with abdominal pain taking other ARBs who had duodenal biopsy and examined their biopsies to determine whether the changes were specific for olmesartan. We identified those patients whose indication for the procedure was abdominal pain to avoid those whose symptom was diarrhoea.
Methods
We performed a retrospective cohort study using the electronic medical record of Columbia University Medical Center endoscopy unit (ProVation Medical Systems, Wolters Kluwer Health, New South Wales, Australia). This record includes all home medication use reported by outpatients undergoing OGD. This list of medications is ascertained by a trained nurse during an interview immediately preceding the procedure. We queried the medical record for patients in whom the indication for OGD was abdominal pain (self-reported, no formal diagnostic criteria employed) and identified 20 outpatients who listed olmesartan as one of their medications. We then matched each patient by age and gender to a control patient who did not report any ARB when listing his/her medications. Using the same process, we identified another 20 users of non-olmesartan ARBs and corresponding matched controls. We excluded all patients with a history of coeliac disease, inflammatory bowel disease or Helicobacter pylori infection (present or prior). In total, we identified 80 patients undergoing OGD for abdominal pain: 20 olmesartan users with 20 matched controls and 20 non-olmesartan ARB users with 20 matched controls. This study was approved by the Columbia University Medical Center Institutional Review Board.
Abnormalities that are seen in enteropathies that include coeliac disease and the sprue-like enteropathy of olmesartan including villous atrophy, crypt hyperplasia, increased IEL concentration, chronic lamina propria inflammation and increased subepithelial collagen deposition were evaluated on routine H&E-stained slides by a gastrointestinal pathologist who was blinded to the medication status (SML). The maximum IEL count in 100 epithelial cells was counted by routine H&E stain. In addition, increased crypt apoptosis (abnormal was considered more than 2 crypt apoptotic bodies in any 10 consecutive crypts or more than one apoptotic body per biopsy piece), active inflammation (defined as any extravascular neutrophils) and eosinophilia were also documented.
Statistical analysis
We compared the prevalence of each of the above histopathological findings among ARB users and their matched controls. We used the χ2 and Fisher exact test when comparing proportions, and used the Mann–Whitney test when comparing IEL counts. After reviewing these comparisons, we subsequently performed a post-hoc analysis comparing ARB-exposed subjects with controls with regard to the composite outcome of one or more of the following findings: architectural abnormalities (villous atrophy or crypt hyperplasia), increased IEL or chronic inflammation. In this analysis, individuals who met one or more of these aforementioned criteria were collectively compared, via χ2 testing, to those who met none of these criteria.
All p values reported are two-sided. We used SAS V.9.3 (Cary, North Carolina, USA) for statistical calculations.
Results
Among the 20 olmesartan users, the mean age was 59.5 years and 70% were women (table 1).
Patient characteristics
Among 20 non-olmesartan ARB users, the mean age was 58.5 years and 55% were women. The indication for OGD was abdominal pain in all cases and controls. When we compared duodenal biopsies of olmesartan users with controls, we identified no single histopathological finding that was significantly more frequent in either group (table 2).
Histological features of olmesartan and other ARB users compared with controls
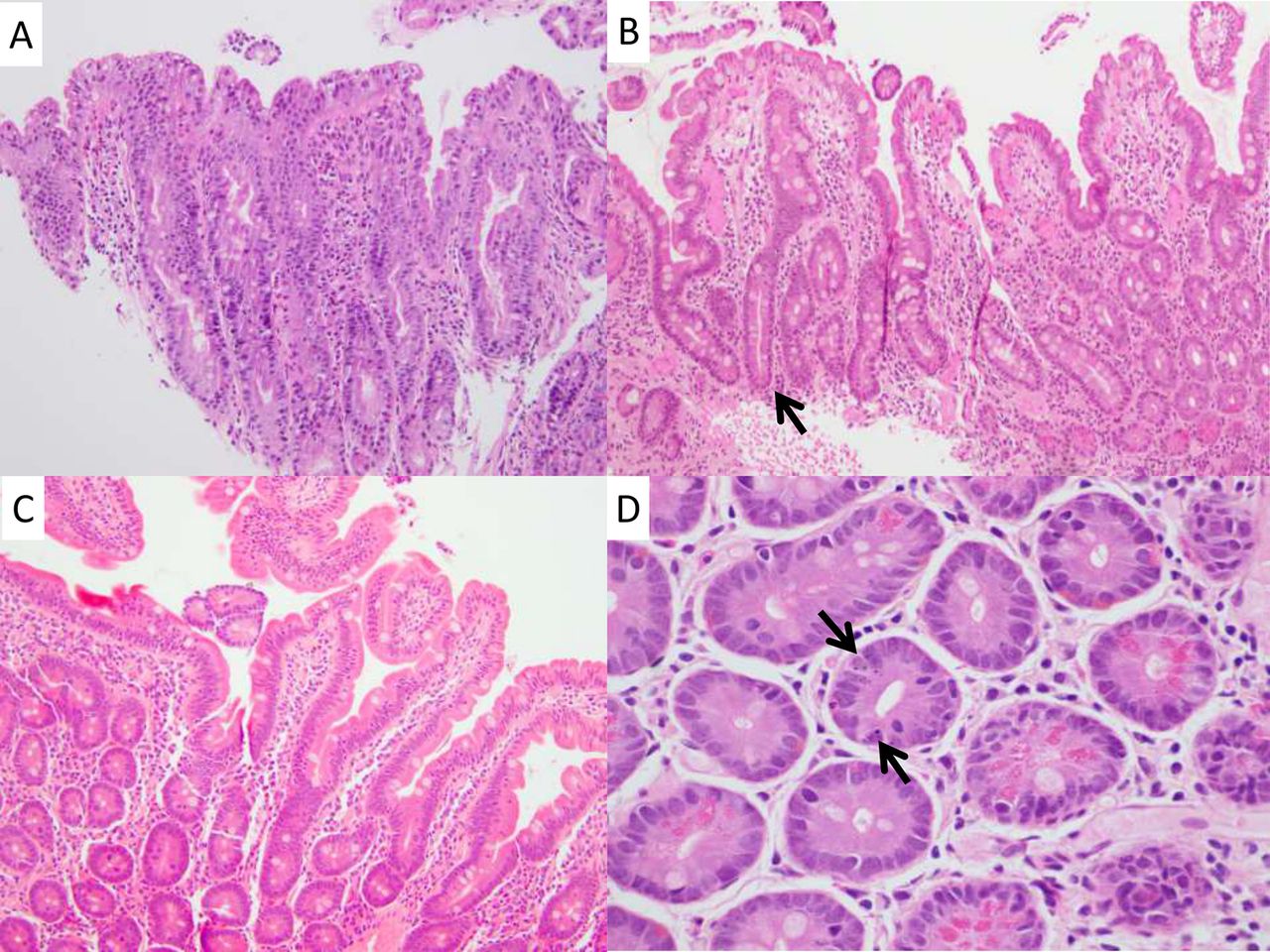
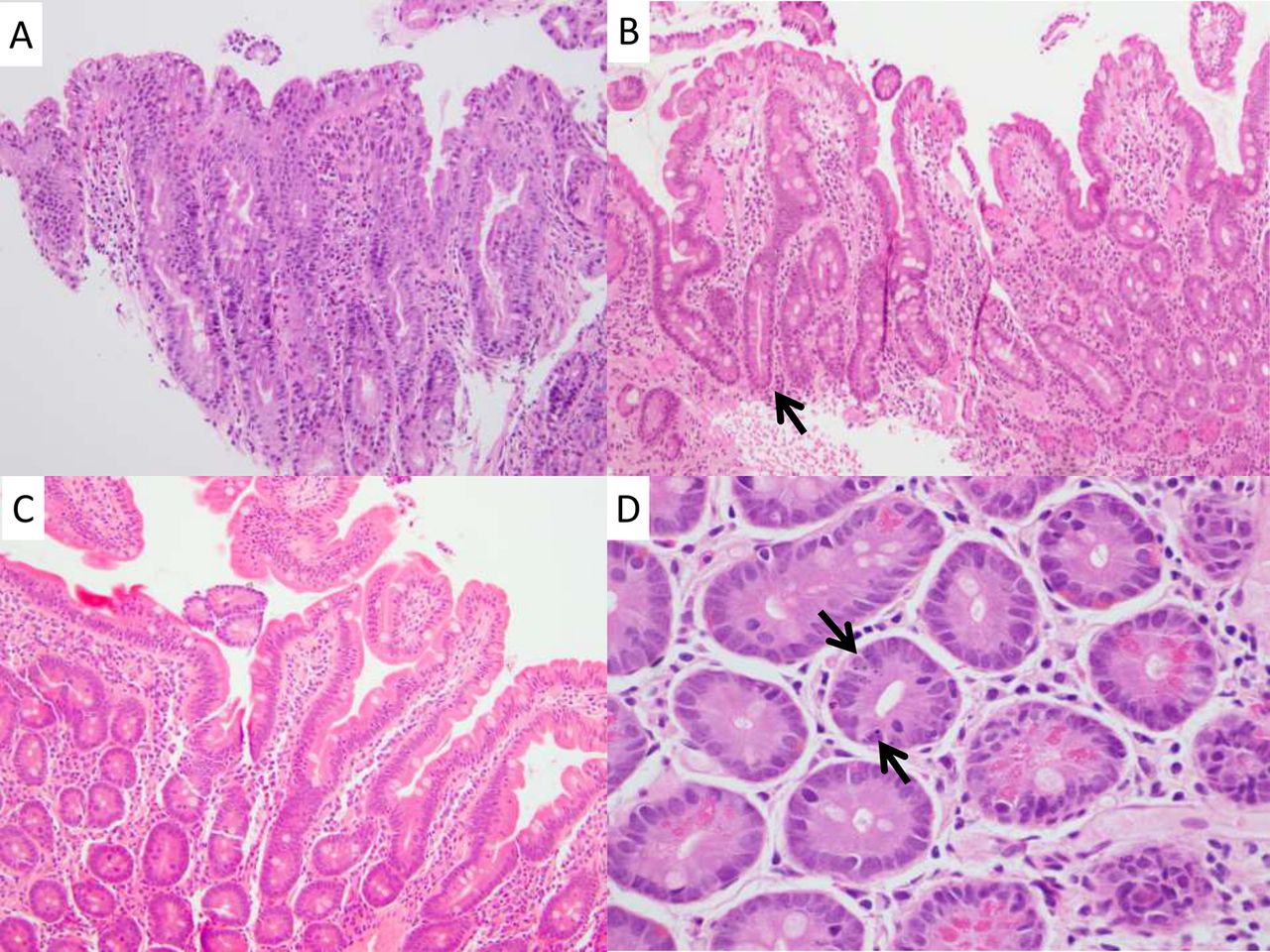
However, there were variables and a composite outcome which showed trends towards significance. Of note, 10 of 20 olmesartan-exposed patients (50%) had one or more of the following sprue-like features: architectural distortion (villous atrophy and/or crypt hyperplasia), generalised increase in IEL and chronic inflammation (figure 1A–C). This compares with 4 of 20 control patients (10%, p=0.10). Regarding individual findings, olmesartan users had more positive findings than control patients for each variable investigated (other than increased subepithelial collagen which was not seen in any case or control), though none achieved statistical significance. Specifically, 25% of olmesartan users had foci of villous atrophy compared with 6% of control patients (p=0.33). The mean maximum IEL count was 13.7 in the olmesartan group compared with 10.6 for controls (p=0.09). Certain other features also were more common in olmesartan users than in control patients, but they too failed to reach statistical significance. The most notable of these was increased crypt apoptosis, which was seen in 25% of olmesartan users compared with 10% of controls (figure 1D).
{kind=link}
Highlighted findings in olmesartan users. (A) Representative photomicrograph of a small bowel biopsy from an individual showing one of several foci of villous atrophy, this particular case shows total villous atrophy but lacks intraepithelial lymphocytosis (H&E 200×). (B) A case with milder findings, including mild villous atrophy and focally pronounced crypt hyperplasia (arrow; H&E 100×). (C) This case had normal architecture, but a mild, generalised increase in intraepithelial lymphocytes (H&E 200×). (D) The case depicted in panel C also showed increased crypt apoptosis, including a crypt with 3–4 apoptotic bodies (arrows; H&E 600×).
We also compared duodenal biopsies from individuals taking ARBs other than olmesartan with patients taking no ARB. There were no statistically significant differences and no trends that suggested a similar effect (table 2).
Discussion
Olmesartan is a widely prescribed ARB used in the management of hypertension. Rarely, patients taking this drug develop a life-threatening diarrheal illness with duodenal biopsies that reveal a severe enteropathy often with increased collagen deposition.1 A study performed at our institution showed that over 10 years, 72 patients had been referred with a diagnosis of seronegative villous atrophy (negative coeliac disease serologies). The most common diagnosis in this group was seronegative coeliac disease (20 patients who had coeliac disease associated human leucocyte antigen haplotypes and responded to a gluten-free diet). The second most common diagnosis (n=19) was medication-related enteropathy. Sixteen patients had olmesartan exposure and had similar clinical and histological findings as described in the Mayo Clinic series. Eleven of the 16 olmesartan-exposed patients had increased subepithelial collagen.2 Of considerable relevance to our study is a case reported by Talbot. The patient described was taking olmesartan, but did not have diarrhoea (presented with constipation). The patient had multiple endoscopies with biopsy. The first duodenal biopsy showed normal duodenal architecture but had increased lamina propria lymphoplasmacytic inflammation and IEL. A subsequent biopsy was similar, although showed ‘mild villous blunting.’ Based on the reports previously described, this patient was taken off olmesartan despite the lack of significant symptoms.16 It is intriguing to consider whether this patient would have developed the ‘full-blown’ clinical and histological syndrome if he had continued to take this agent. Also of particular relevance to this study is a case, which showed similar clinical and pathological characteristics as were described in the Mayo series of olmesartan patients in a patient taking another ARB, valsartan.17
To determine whether olmesartan usage was associated with intestinal damage, short of the severe sprue-like enteropathy, we identified patients with abdominal pain who were taking olmesartan or other ARBs and had a duodenal biopsy. We demonstrated a trend towards sprue-like enteropathic changes in individuals taking olmesartan compared with controls. The trend towards increased crypt apoptosis is interesting mechanistically, as certain other drugs known to cause intestinal damage often demonstrate this finding (e.g. mycophenolate mofetil).18 These changes appear to be specific for olmesartan as there were none identified in those taking other ARBs.
This is the first study to our knowledge that investigates whether exposure to olmesartan or other ARBs is associated with histopathological abnormalities among outpatients undergoing duodenal biopsy. Our study has several limitations including its retrospective design, single centre setting and lack of information regarding duration of ARB use. We did not systematically exclude patients with known microscopic colitis; however, a post-hoc review showed that only 1 of 80 patients had microscopic colitis in our records (olmesartan user with no histopathological findings in our study). A larger sample size may have been useful, as it is possible that olmesartan causes a true increase in duodenal histopathological abnormalities but that our study was underpowered to detect this effect. Finally, we do not know whether any of the patients has subsequently discontinued olmesartan, and if so, if their abdominal pain has resolved.
This study raises the possibility that there may be a spectrum of injury associated with olmesartan use, apart from the severe syndrome that causes life-threatening diarrhoea. Further studies are needed to determine whether olmesartan use is associated with abdominal pain or other gastrointestinal symptoms and signs, as opposed to the well-characterised diarrhoea with sprue-like enteropathy. Future studies should follow-up the patients in this study to determine whether any of the olmesartan-exposed patients develop the severe enteropathic phenotype and if any of the histopathological variables we investigated are predictive thereof.
Take home messages
-
This study raises the possibility that there is a spectrum of duodenal injury associated with olmesartan use.
-
Angiotensin receptor blockers other than olmesartan are not associated with any histopathological findings in duodenal biopsies of patients with abdominal pain.
-
Further studies are needed to determine whether olmesartan use is associated with abdominal pain and if the patients with the histopathological findings described here are at risk for developing the recently described severe sprue-like enteropathy.
References
Footnotes
-
Contributors SML: concept development, data collection, drafter of manuscript and guarantor of data. EDB: data collection and manuscript review. CA-G: concept development and manuscript review. GB: concept development and manuscript review. PG: concept development and manuscript review. BL: concept development, data analysis (statistics) and manuscript review.
-
Competing interests None.
-
Ethics approval Columbia University Medical Center Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.