Article Text

Abstract
Immune checkpoint inhibitors (CPIs) are a relatively new class of ‘miracle’ dugs that have revolutionised the treatment and prognosis of some advanced-stage malignancies, and have increased the survival rates significantly. This class of drugs includes cytotoxic T lymphocyte antigen-4 inhibitors such as ipilimumab; programmed cell death protein-1 inhibitors such as nivolumab, pembrolizumab and avelumab; and programmed cell death protein ligand-1 inhibitors such as atezolizumab. These drugs stimulate the immune system by blocking the coinhibitory receptors on the T cells and lead to antitumoural response. However, a flip side of these novel drugs is immune-related adverse events (irAEs), secondary to immune-mediated process due to disrupted self-tolerance. The irAEs in the gastrointestinal (GI) tract/liver may result in diarrhoea, colitis or hepatitis. An accurate diagnosis of CPI-induced colitis and/or hepatitis is essential for optimal patient management. As we anticipate greater use of these drugs in the future given the significant clinical response, pathologists need to be aware of the spectrum of histological findings that may be encountered in GI and/or liver biopsies received from these patients, as well as differentiate them from its histopathological mimics. This present review discusses the clinical features, detailed histopathological features, management and the differential diagnosis of the luminal GI and hepatic irAEs that may be encountered secondary to CPI therapy.
- colon
- histopathology
- liver
Statistics from Altmetric.com
Immune checkpoint inhibitors (CPIs) are a relatively new class of drugs that stimulate an antitumour response by targeting immune cell checkpoints.1–3 These wonder drugs have broadened treatment options and have improved survival in patients with advanced-stage cancers.4 Originally used for advanced malignant melanoma, this novel immunotherapy has now been approved or is currently being tested in clinical trials for other malignancies as well, such as non-small cell lung carcinoma, renal cell carcinoma, microsatellite unstable colorectal carcinoma and urothelial carcinoma.5–10 Immune checkpoints include cytotoxic T lymphocyte-associated antigen 4 (CTLA-4), programmed cell death protein-1 (PD-1) and programmed cell death protein ligand-1 (PD-L1) receptors, and approved immune CPIs include ipilimumab (CTLA-4 inhibitor); nivolumab, pembrolizumab and avelumab (anti-PD-1 drugs); and atezolizumab (anti-PD-L1 drug).1–3
Although CPIs improve tumour control, they have the potential to cause autoimmune pathology as bystander non-tumour host cells are also affected—referred to as immune-related adverse events (irAEs). The irAEs most commonly affect the skin, luminal gastrointestinal (GI) tract, liver, endocrine organs and the lungs, sometimes long after completing the therapy.11 12 The irAEs in the GI tract/liver may result in diarrhoea, colitis or hepatitis. Acute pancreatitis has been reported in some studies; however, clinical pancreatitis is rare and is hence proposed as anecdotal by experts, at this time.2
Given the successful therapeutic responses and survival benefits seen in many patients treated with CPI therapy, it is anticipated that the use of these drugs will increase more so in the future, and will probably lead to an increased number of patients seen in clinical practice affected by CPI therapy-induced irAEs. An accurate diagnosis is crucial for optimal patient management and preventing further worsening of irAEs in these patients.
The current review gives an overview of the clinical findings, detailed histopathological features, differential diagnosis and management of CPI therapy-induced irAEs encountered in the luminal GI tract and the liver.
Mechanism of action
Immune checkpoints including CTLA-4, PD-1 and PD-L1 receptors downregulate T cell immunity. Blockage of these checkpoints promotes activation and proliferation of the effector T cells, thereby enhancing the cellular immunity.
The activation of T cells requires a binding antigen along with costimulation via the CD28 receptor. CD28 binds ligands of the B7 family, leading to proliferation of T cells and migration towards the tumour cells, harbouring those specific tumour-associated antigens. The activated T cells also express CTLA-4 receptor on its surface, and CTLA-4 outcompetes CD28 for binding to B7, as it has higher affinity for these ligands. The lymphocytes are arrested in the G1 of the cell cycle, thereby preventing death of the tumour cell. Blockage of CTLA-4 by ipilimumab (a human monoclonal antibody that binds to and inhibits CTLA-4) enables cytotoxic T lymphocytes to exert their cytotoxic effects on the tumour cells.1 2 13–16
PD-1 is another immune checkpoint and is present on the surface of activated T cells. PD-L1 is the primary PD-1 ligand that is upregulated in solid tumours. The interaction of PD-1 on the T cell surface with PD-L1 present on the tumour cells deactivates T cells, hence allowing the tumour cells to escape the immune system. The PD-1/PD-L1 inhibitors inhibit this binding, and thereby facilitate the activation of cytotoxic T cells against the tumour cells.1 2 15 17
Since the target of immune CPI therapy is T cells, it can potentially be used against a variety of malignant neoplasms.1
Luminal GI tract injury due to CPI therapy
Clinical features
In most cases, CPI therapy-induced GI side effects are transient and mild or moderate. The most commonly reported GI side effect is diarrhoea. Diarrhoea is graded by clinicians using the Common Terminology Criteria for Adverse Events (CTCAE) V.4 developed by the National Cancer Institute of the National Institutes of Health, as stated below2:
Grade 1: increase of <4 stools per day over baseline.
Grade 2: increase of 4–6 stools per day over baseline.
Grade 3: increase of 7 or more stools per day over baseline, incontinence, hospitalisation indicated, limiting self-care activities of daily living.
Grade 4: life-threatening consequences, urgent intervention indicated.
Grade 5: death.
Colitis is graded using the CTCAE V.4 developed by the National Cancer Institute of the National Institutes of Health, as stated below2:
Grade 1: asymptomatic, clinical or diagnostic observations only, intervention not indicated.
Grade 2: abdominal pain, mucus or blood in stool.
Grade 3: severe abdominal pain, change in bowel habits, medical intervention indicated, peritoneal signs.
Grade 4: life-threatening consequences, urgent intervention indicated.
Grade 5: death.
CPI-induced diarrhoea occurs in up to 30% of patients in clinical trials.3 The incidence of GI side effects is reported to be higher and more severe in patients treated with CTLA-4 blocking antibodies as compared with patients receiving PD-1 receptor inhibitors.2 18 19 One of the studies reports that diarrhoea is seen in 35% of patients treated with CTLA-4, 17%–20% in anti-PD-1 and 44% in those treated with combination therapy.13 Another study has shown that treatment-related adverse events of grade 3 or 4 occurred in 16.3% of patients in the nivolumab (anti-PD-1) group, 55% of those in the nivolumab-plus-ipilimumab group (combination therapy) and 27.3% of those in the ipilimumab group (anti-CTLA-4 group), suggesting that the combination therapy increases the risk of irAEs more than either agent used alone.20 Clinically significant cases of colitis with perforation have also been reported in the literature, particularly after treatment with CTLA-4 inhibitors.21
Diarrhoea and colitis usually occur within a median of 6 weeks into starting the therapy, but can start later as well. Hence, suspicion for CPI therapy-induced colitis should remain high for several months after therapy.3 Studies have reported that the median time to onset of diarrhoea is 5–8 weeks after start of ipilimumab (or combination with ipilimumab), compared with 3–6 months for anti-PD-1 therapy.2 13 22
Endoscopic findings
Although diarrhoea is the most common irAE in the GI tract associated with CPI treatment, colonoscopy is only recommended for persistent grade 2 or higher diarrhoea due to the risks associated with these procedures.23 Endoscopic examination can range from normal findings to mild colitis, or severe inflammatory changes such as exudates, granularity, erythema, loss of vascularity and erosions/ulcerations. The predominant pattern of injury seen is pancolitis, with a minority of cases showing left-sided colitis, as well.18 24–26 However, even if signs of inflammation are absent on gross examination, it is still recommended that the biopsies be taken to confidently exclude colitis.2
Histopathological features in colonic biopsies
The most common site biopsied in patients with CPI-induced diarrhoea and/or colitis is colon. Hence, the histopathological features encountered in colonic biopsies would be reviewed in detail. It is debatable whether the therapy directly causes colitis or rather unmasks a pre-existing susceptibility to colitis.25
Anti-CTLA-4 (ipilimumab)-induced colitis
The most common histopathological feature reported in colonic biopsies is that of ‘autoimmune-like colopathy’13 27 28 (figures 1–3) and consists of the following:
Dense, predominantly lymphocytic infiltrate in the lamina propria along with frequent plasma cells and eosinophils (figure 1).
Neutrophilic inflammation is commonly seen, including neutrophilic cryptitis and crypt microabscesses, as well as increased crypt epithelial apoptosis (figures 1 and 2).
Variable increase in intraepithelial lymphocytes (IELs) (figure 3).
Notably, in most studies, features of chronicity (such as well-formed basilar lymphoplasmacytosis, significant architectural distortion and Paneth cell metaplasia in the left colon) are typically absent.
Granulomas are absent.

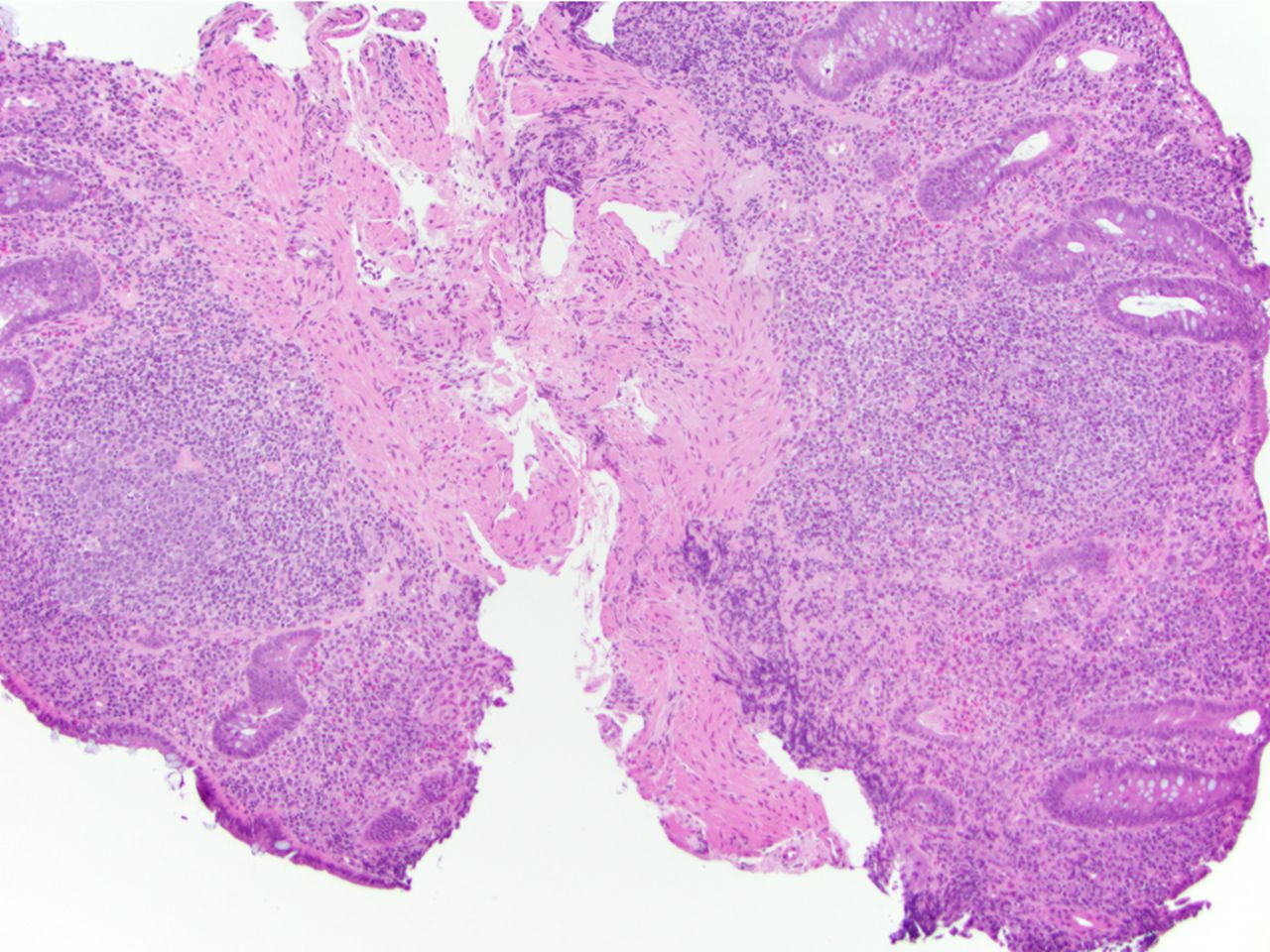
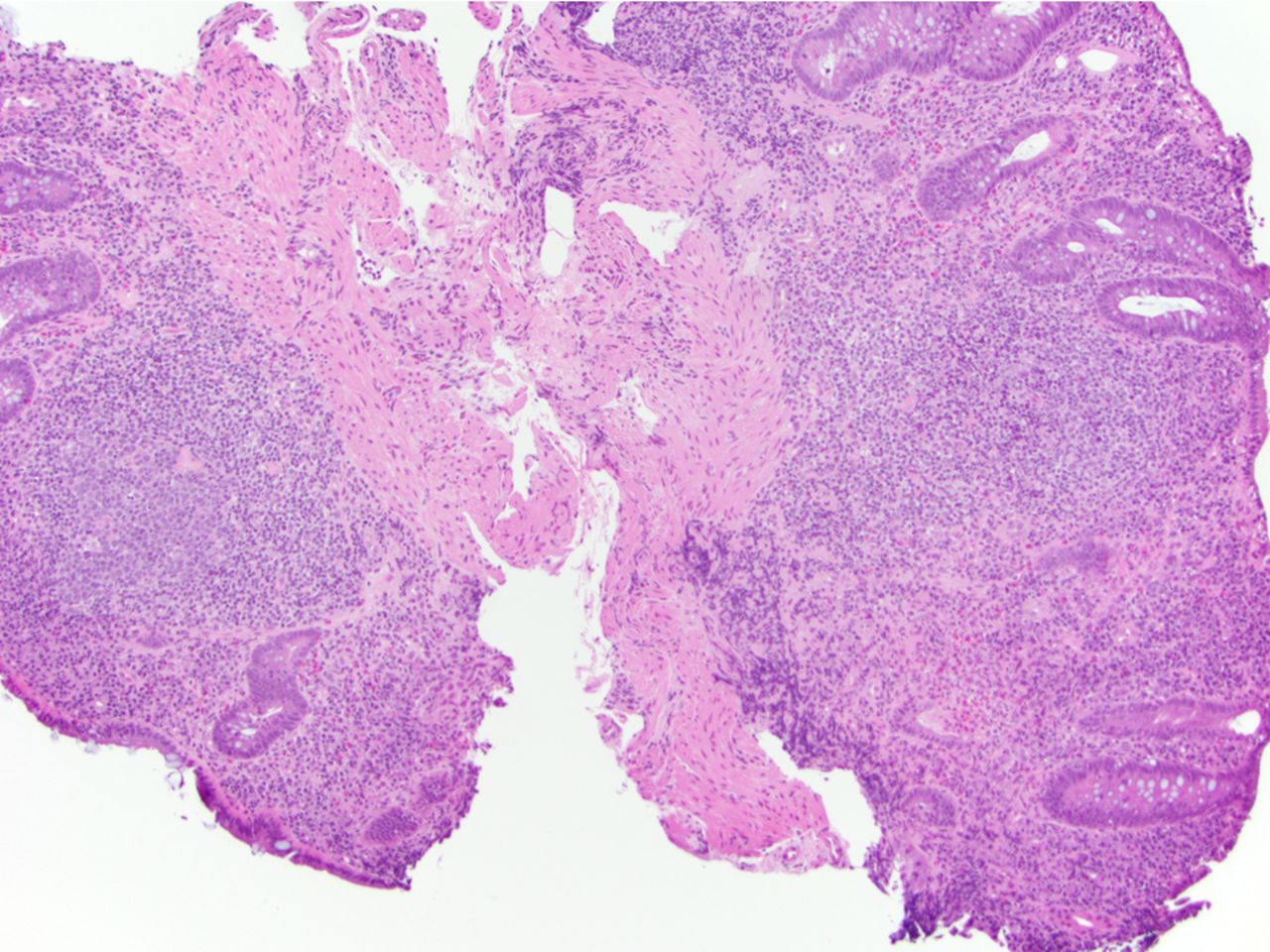
Low-power photomicrograph highlighting dense, predominantly lymphoplasmacytic lamina propria inflammatory cell infiltrate along with frequent eosinophils seen with anti-CTLA-4-induced colitis (H&E ×100). A similar pattern of injury has been reported with anti-PD-1 colitis. The bottom left inset (H&E ×200) highlights neutrophilic cryptitis and crypt abscess, and the top right inset shows neutrophilic crypt abscess and crypt atrophy, typically seen in these cases (H&E ×400). CTLA-4, cytotoxic T lymphocyte antigen-4; PD-1, programmed cell death protein-1.
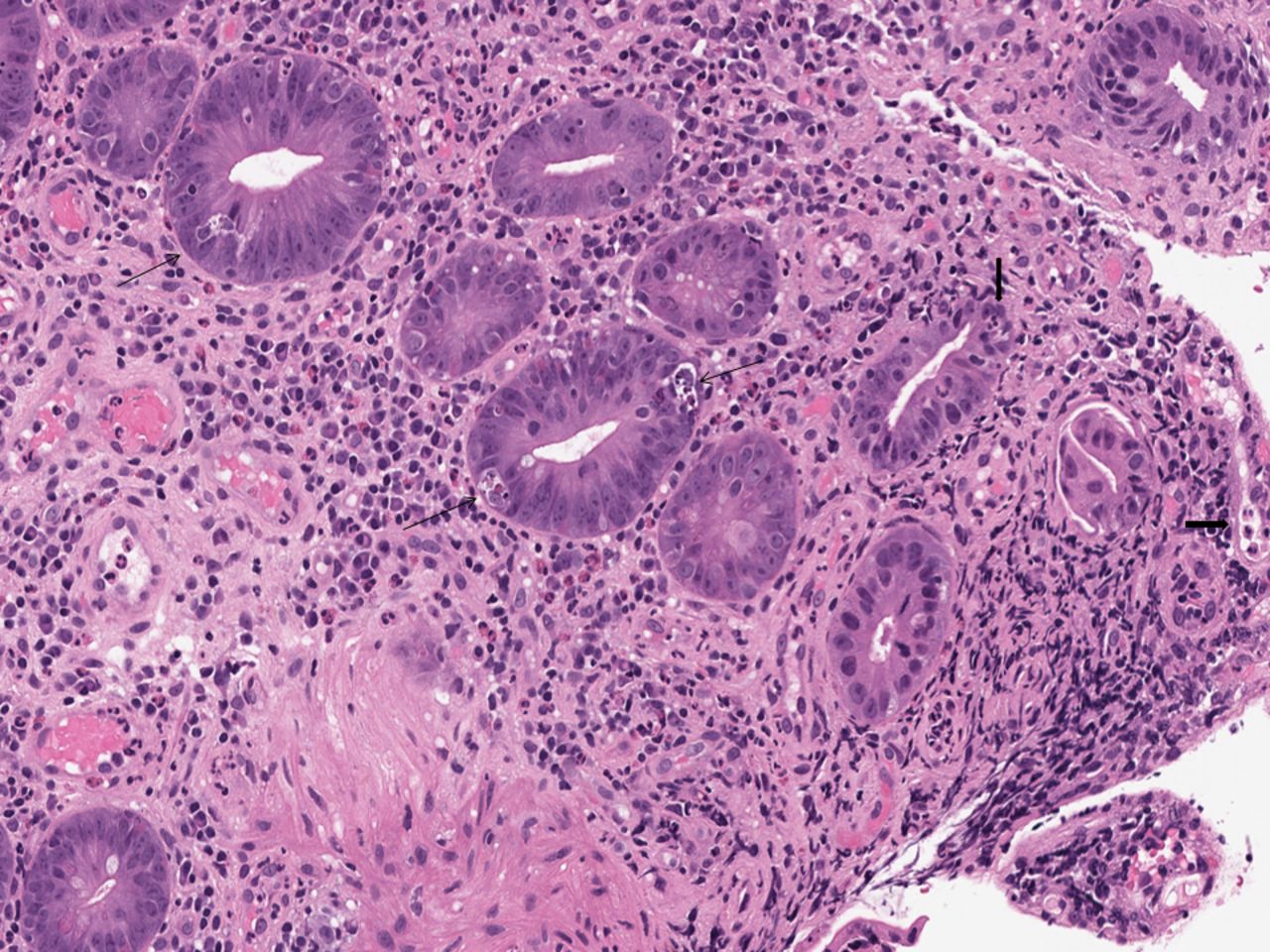
Lower power photomicrograph highlighting active colitis with increased apoptosis seen with anti-PD-1 therapy in this case. The biopsy shows active mucosal injury including neutrophilic crypt microabscesses and cryptitis (highlighted by thick arrows), and increased crypt epithelial cell apoptosis (highlighted by thin arrows) with the presence of crypt atrophy and dropout. Similar features have been described with anti-CTLA-4-induced colitis (H&E ×200). CTLA-4, cytotoxic T lymphocyte antigen-4; PD-1, programmed cell death protein-1.

‘Lymphocytic colitis pattern of injury’ seen with anti-PD-1 therapy effect. Similar findings can be seen in patients with anti-CTLA-4 colitis. The biopsies exhibit increase in intraepithelial lymphocytes along with evidence of surface epithelial injury, and increased lamina propria mononuclear inflammatory cells. Neutrophilic injury is absent in this case (H&E ×100; inset H&E ×400). CTLA-4, cytotoxic T lymphocyte antigen-4; PD-1, programmed cell death protein-1.
In one study, intraepithelial neutrophils were detected in 72% of samples, cryptitis in 92% and crypt abscesses in 60%. Notably, crypt irregularities were found in 40% of colon biopsy specimens in this study.24
Anti-PD-1-induced colitis
The histopathological features of anti-PD-1-associated colitis reported in the literature are fairly similar and usually fit into one of the patterns of injury described below.
The most commonly reported pattern of injury is an active colitis with increased apoptosis and crypt atrophy/dropout, somewhat similar to the above-described features of anti-CTLA-4 colitis. The biopsy shows active mucosal injury, including neutrophilic crypt microabscesses and cryptitis, increased crypt epithelial cell apoptosis, and presence of crypt atrophy and dropout. Atrophic crypts can exhibit prominent attenuation of crypt epithelium along with luminal apoptotic debris mixed with inflammatory cells, somewhat reminiscent of ‘apoptotic microabscesses’ commonly seen in colitides of some other aetiologies as well (figures 1 and 2).1 25 26
The other observed pattern of injury is lymphocytic colitis, which has also been previously observed in patients with anti-CTLA-4 colitis. The biopsies exhibit increase in IELs along with evidence of surface epithelial injury, and increased lamina propria mononuclear inflammatory cells in a top-heavy distribution (figure 3). In these cases, there are no features of chronic mucosal injury, and either no or minimal neutrophilic inflammation, along with absence of neutrophilic crypt microabscesses.25
A single case of an anti-PD-1-associated collagenous colitis has also been reported.29
Granulomas associated with ruptured crypts are seen in 18% of biopsies.26
Features of chronic mucosal injury (such as basilar lymphoplasmacytosis, significant crypt architectural distortion or Paneth cell metaplasia in the distal colon or pyloric gland metaplasia) can be seen in patients with recurrent anti-PD-1 colitis (figure 4).1 25
A patient with recurrent anti-PD-1 colitis showing features of chronic mucosal injury, in the form of basilar lymphoplasmacytosis and significant crypt architectural distortion. The lamina propria shows mixed inflammatory infiltrate including prominent eosinophils (H&E ×100). PD-1, programmed cell death protein-1.
Multiple drugs (anti-CTLA-4 and PD-1 inhibitors, either sequentially or in combination)
There is a very limited literature about the histopathological features of colon biopsies from patients treated with both anti-PD-1 and CTLA-4 inhibitors, either sequentially or in combination.1 Bavi et al 30 reported a series of 34 GI biopsies taken from 21 patients, and all of their patients received PD-1/PD-L1 inhibitors, namely pembrolizumab (MK3475) or durvalumab (MEDI4736), along with chemotherapy and CTLA-4 inhibitors, either sequentially or in combination. They found a predominance of IELs in the colon (28%) rather than intraepithelial neutrophils (17%). The IELs were identified both on the surface epithelium and within tubules in the lamina propria.30
Histopathological features in extracolonic GI biopsies
Since patients with CPI-induced GI injury mostly undergo colonic biopsies, there is very limited body of literature reviewing histopathological findings in biopsies taken from other luminal GI sites outside of the colon.
The limited data report that when biopsied, the most commonly observed histological features in the gastric mucosal biopsy are expansion of lamina propria by inflammatory cells as well as intraepithelial neutrophils. An increased number of IELs and apoptosis has also been reported. The duodenal and ileal biopsies commonly show villous blunting, lamina propria expansion by lymphoplasmacytic infiltrates consisting of lymphocytes, plasma cells and eosinophils, with few neutrophils, increased number of IELs, and neutrophilic cryptitis and/or villitis. Increased apoptosis is a variable finding in different studies. Granulomas are absent.1 26 27 30 31
Differential diagnosis
The differential diagnosis of active colitis pattern of injury with apoptosis is not entirely specific and requires clinical history of CPI therapy with a fair index of clinical suspicion to make a definitive diagnosis. The histological differential includes infections (particularly cytomegalovirus (CMV)), acute graft-versus-host disease (GVHD), other drug-induced colitis and autoimmune enteropathy. CMV colitis should always be considered with the above histological picture as patients receiving CPI therapy are already immunosuppressed and hence are inherently susceptible to opportunistic infections. It is recommended that pathologists have a low threshold for ordering CMV immunohistochemical stain. There are many drugs that may exhibit similar pattern of injury as above, but clinical history and discussion with the patient’s clinician, including the use of specific drugs, can help narrow down this differential. Some of the drugs that may produce similar pattern of injury, particularly prominent apoptosis, include mycophenolate mofetil (MMF). MMF colitis may also be associated with a significant increase in lamina propria eosinophils. Some other drugs that may exhibit an almost similar pattern of injury include fluorouracil and antitumour necrosis factor antibody therapy, methotrexate and phosphoinositide 3-kinase-d inhibitor idelalisib, among others. GVHD colitis may exhibit similar histological picture; however, a clinical history of allogenic stem cell transplantation versus CPI therapy may help clinch the diagnosis.1 25 32–36
Lymphocytic colitis pattern of injury can be seen secondary to multiple other medications reported in the literature, such as non-steroidal anti-inflammatory drugs, proton pump inhibitors and histamine receptor inhibitors, among others.37 Again a definitive diagnosis requires clinical history of CPI therapy, along with being aware that CPI therapy can produce a microscopic colitis pattern of injury, mostly lymphocytic colitis and very rarely, collagenous colitis.
In cases of recurrent CPI colitis, chronic mucosal injury may be seen, and the histological findings of chronic active colitis may lead the pathologist to consider a diagnosis of inflammatory bowel disease (IBD). However, these cases also show increased crypt apoptosis along with crypt atrophy/dropout, which is unusual for IBD.13 25 26 Also, the knowledge that recurrent CPI therapy-induced colitis can occur many months after stopping CPI therapy may at least help the reviewing pathologist suggest that these histological findings may be secondary to recurrent CPI therapy-induced colitis particularly when apoptotic features are conspicuous versus rendering a new diagnosis of IBD (provided that the patient has no history of IBD).25
Management and follow-up
The management varies by the grade and severity of symptoms. When CPI injury is suspected, it is prudent to perform a detailed history, physical examination and/or tests (such as stool examination and cultures) to exclude infectious colitis. For grade 1 symptoms, it is recommended to continue the therapy with close monitoring and symptomatic treatment. For grade 2 symptoms, CPI therapy should be withheld along with symptomatic treatment including antidiarrhoeal agents. For persistent grade 2 symptoms, systemic corticosteroids are started. If severe (grade 3 or 4) symptoms develop, CPIs should be stopped permanently and corticosteroids should be initiated. For persistent or worsening severe symptoms, infliximab (a monoclonal antibody against the inflammatory cytokine tumour necrosis factor-alpha) is recommended and has been shown to dramatically improve symptoms within 24 hours.2 3 38–41
Hepatic injury due to CPI therapy
Clinical features
Hepatic side effects from CPI therapy are less frequently encountered as compared with those of the luminal GI tract, and have been reported in approximately 3%–10% of patients receiving these drugs.2 42–44 Most commonly, this manifests as an asymptomatic increase in liver function tests (LFTs), particularly aspartate aminotransferase (AST) and alanine aminotransferase (ALT) with mildly elevated total bilirubin (T-BIL).2 11 14 15 43–45
The National Cancer Institute’s CTCAE V.4 grades the severity of CPI therapy-induced hepatitis as follows2:
Grade 1: AST or ALT 1–2.5×upper limit of normal (ULN) and/or T-BIL1–1.5×ULN.
Grade 2: AST or ALT 2.5–5×ULN and/or T-BIL 1.5–3×ULN.
Grade 3: AST or ALT>5×ULN and/or T-BIL >3×ULN.
Grade 4: AST or ALT>8×ULN.
Grade 5: death.
Hepatitis most often becomes clinically evident 8–12 weeks after starting the therapy but may occur at any time.2
Radiological features
Hepatic findings on abdominal CT differ depending on the severity of side effects. In relatively mild cases, findings mostly appear normal. However, more severe cases show findings similar to that seen in other common causes of acute hepatitis, namely mild hepatomegaly, attenuated liver parenchyma, periportal oedema and periportal lymphadenopathy. Findings on ultrasonography may include conspicuous periportal echogenicity and/or oedema of the gallbladder wall.2 11 43
Histopathological features
Anti-CTLA-4 (ipilimumab)-induced hepatic injury
Most of the reported cases of ipilimumab-induced liver injury show active panlobular hepatitis with a mixed inflammatory infiltrate consisting predominantly of lymphocytes along with numerous lobular macrophages in aggregates (figures 5 and 6). The macrophages often show a prominent sinusoidal distribution and frequently form loose ‘microgranulomas’ within the hepatic lobules. Scattered eosinophils and neutrophils are present in most cases. The number of plasma cells is variable, with the majority of the cases showing rare or few plasma cells. Foci of confluent necrosis, multifocal hepatocyte apoptosis and ballooning degeneration are also seen. Central vein endothelialitis with variable foci of perivenular inflammatory infiltrate and collapse has also been reported in many cases.14 Hepatocytes show varying degrees of regenerative changes, including binucleation, increased cell size, prominent nucleoli and mitotic figures.
The next common pattern of injury seen is the centrilobular (zone 3) hepatitis, where active hepatitis with the above-described features is restricted to zone 3.2 14 15 43 45
Less reported patterns: A biliary pattern of injury has also been reported with a case showing mild portal mononuclear inflammatory cell infiltrate around the foci of bile ductular proliferation, suggestive of a predominant injury to the bile duct.43 A case of mixed, neutrophil-rich, predominantly portal inflammatory infiltrate with foci of acute cholangitis has also been reported. Steatohepatitis is rarely reported and the authors propose that this may represent exacerbation of underlying fatty liver disease secondary to ipilimumab.14

Low-power photomicrograph seen with checkpoint inhibitor-induced hepatic injury depicting the most common acute hepatitis (autoimmune hepatitis-like) pattern of injury characterised by active panlobular hepatitis with a mixed inflammatory infiltrate consisting predominantly of lymphocytes along with lobular macrophages. Scattered eosinophils are also seen (H&E ×100). (Photo courtesy of Amitabh Srivastava, MD, Brigham and Women’s Hospital.)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Medium-power photomicrograph of checkpoint inhibitor-induced hepatic injury showing lobular hepatitis with a mixed inflammatory infiltrate consisting predominantly of lymphocytes with lobular macrophages, and scattered acidophilic bodies. The hepatocytes show varying degrees of regenerative changes (H&E ×200). (Photo courtesy of Amitabh Srivastava, MD, Brigham and Women’s Hospital.)
Anti-PD-1 (nivolumab, pembrolizumab)-induced hepatic injury
There have been only limited papers describing anti-PD-1-induced hepatic injury. All reported cases exhibit predominantly lobular hepatitis with milder portal inflammation (figures 5 and 6). Lobular injury is manifested in the form of randomly scattered foci of patchy necrosis and acidophilic bodies with no confluent necrosis. Only a single reported case showed centrilobular zonal necrosis. Other described changes include bile ductular proliferation, cholangiolitis, focal endothelialitis and bile duct injury.15 46
The overall pattern of hepatic injury appears to be alike between anti CTLA-4-induced and anti-PD-1-induced hepatitis, although confluent necrosis and histiocytic aggregates may be less common or practically absent in the latter.15 47
Combination ipilimumab and nivolumab therapy
Everett et al 48 described two cases of fibrin ring granulomas in patients with hepatitis secondary to combination ipilimumab (anti-CTLA-4) and nivolumab (anti-PD-1) therapy. These are characterised histologically by a central lipid vacuole surrounded by histiocytes, a ring of fibrin and an outer layer of histiocytes. Both the biopsies in this study showed lobular inflammation with histiocytic aggregates and endothelial injury similar to ipilimumab-induced hepatitis; however, unlike the latter, steatosis was a conspicuous feature and fibrin ring granulomas were present in both cases with combination therapy.48
Differential diagnosis
The above histological findings of CPI-induced hepatic injury are not specific and require clinicopathological correlation, including a temporal relationship with the drug use for a definitive diagnosis. The histological differential diagnosis includes autoimmune hepatitis (AIH), acute viral hepatitis and drug-induced liver injury (DILI) secondary to other drugs, and acute alcoholic liver disease.
AIH can show almost similar histological picture as CPI therapy-induced hepatitis given the panlobular hepatitis or zone 3 hepatitis patterns of injury and confluent necrosis. Although clinical history including history of CPI therapy and serological studies such as IgG levels and autoantibodies (like antinuclear antibody, antismooth muscle antibody) are required to distinguish primary AIH from ipilimumab-associated hepatitis, there are some histopathological features that may suggest a diagnosis of ipilimumab-associated injury. In contrast to primary AIH, the plasma cell infiltrate is usually not prominent in CPI therapy-induced hepatitis, and in anti-CTLA-4 (ipilimumab)-induced hepatic injury there is prominent histiocytic inflammatory infiltrate, typically showing a sinusoidal distribution and frequently forming aggregates or ‘microgranulomas’ within lobules. These findings are unusual in primary AIH and may suggest a diagnosis of CPI therapy-induced hepatitis in the correct clinical setting.
The diagnosis of acute viral hepatitis is based on clinical history/presentation and viral serologies. DILI from other hepatotoxic drugs can show a varied range of histological findings and requires clinical history for a definitive diagnosis.
Treatment
Discontinuation of CPI therapy in addition to immunosuppression with steroids, either alone or in combination with MMF or 6-mercaptopurine, usually leads to near or complete resolution of LFTs in all cases, confirming the diagnosis of a CPI-associated hepatic injury. During steroid treatment, a waxing and waning of LFT abnormalities may be seen, and several courses of tapering steroids may be required.11 14
Summary
Although immune CPIs have improved survival significantly in patients with advanced-stage cancers, these drugs have the potential to cause irAEs, which in the GI tract/liver may manifest as diarrhoea, colitis or hepatitis. The histopathological features of CTLA-4 inhibitors-induced colitis include autoimmune-like enterocolopathy, and anti-PD-1-induced colitis consists of an active colitis with increased apoptosis and crypt atrophy/dropout and a less reported pattern of lymphocytic colitis. Features of chronicity may be seen in recurrent cases. The histopathological features of CTLA-4 inhibitors-induced hepatic injury consist mostly of active panlobular hepatitis with numerous lobular macrophages in aggregates or centrilobular hepatitis. The anti-PD-1-induced hepatic injury exhibits predominantly lobular hepatitis, although confluent necrosis and histiocytic aggregates are less common in the latter. These histopathological features are not entirely specific, and hence correlation with clinical history (particularly drug history), knowledge of the above varied CPI therapy-induced histological patterns and clear communication with the clinical team are crucial for pathologists to differentiate CPI therapy-induced injury from its histopathological mimics in the GI tract (such as infections, acute GVHD, other drug-induced colitis, lymphocytic colitis) and liver (such as AIH, acute viral hepatitis and DILI). Early detection and treatment of these adverse events is important to avoid significant morbidity and mortality. Most irAEs are reversible and respond well to steroid treatment.
Take home messages
Checkpoint inhibitor (CPI) therapy has the potential to cause immune related adverse events such as diarrhoea, colitis or hepatitis.
Histologic features of CPI induced colitis usually manifest as active colitis with increased apoptosis and a less reported pattern of lymphocytic colitis.
The most common histologic feature of CPI induced hepatic injury is that of an acute hepatitis(autoimmune hepatitis-like)pattern of injury.
Correlation with clinical history, high index of clinical suspicion, and knowledge of varied histologic features is essential for a definite diagnosis of CPI induced injury.
Acknowledgments
The authors would like to thank Amitabh Srivastava, MD (Department of Pathology, Brigham and Women’s Hospital) for providing us with figures 5 and 6 in this manuscript.
References
Footnotes
Handling editor Cheok Soon Lee.
Contributors Both the authors (DMK, RC) participated actively in this manuscript and can take public responsibility for the content of this paper. All authors critically revised the paper for intellectual content and have approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; internally peer reviewed.