Article Text

Abstract
The RAS family is among the most commonly mutated genes in all human malignancies including colon cancer. In normal cells, RAS proteins act as a link in the intracellular signal transduction initiated by binding of growth factors to cell membrane receptors mediating cell survival. RAS isoproteins have great morphological similarities, but despite that, they are thought to have different functions in different tissues. RAS mutations, as supported by several studies including animal models, have a role in the development and progression of colorectal cancer. The detection of RAS mutations in patients with colorectal carcinoma, specifically KRAS and NRAS, has significant clinical implications. It is currently recommended that patients with colon cancer who are considered for antiepidermal growth factor receptor monoclonal antibodies, get RAS mutation testing since only those with wildtype-RAS genes benefit from such treatment. Despite decades of research, there is currently no effective and safe treatment that directly targets RAS-mutated neoplasms. Multiple therapeutic approaches directed against RAS mutations are currently experimental, including a promising immunotherapy study using T-cells in patients with metastatic colon cancer.
- colorectal cancer
- molecular diagnostics
- personalized medicine
- kras
- nras
- microsatellite instability (msi)
- braf
Statistics from Altmetric.com
- colorectal cancer
- molecular diagnostics
- personalized medicine
- kras
- nras
- microsatellite instability (msi)
- braf
Introduction
In the USA, colorectal carcinoma is the third most common cancer in men and women and the second leading cause of cancer-related death.1 The current cancer statistics in the USA estimate that in 2018, 237 470 men and women will be diagnosed with colorectal cancer and 50 630 will die from it.1 Colorectal cancer develops because of a complex interaction between various genetic and environmental factors.2 3
Our understanding of the genetic alterations associated with the development and progression of colorectal carcinoma, in both hereditary and sporadic cases has tremendously improved over the last few decades. Colorectal cancer usually develops as a result of stepwise, multiple mutations involving oncogenes and tumour suppressor genes. Currently, the transcriptome data from a multitude of research helped categorise colorectal carcinoma into four molecular subtypes called consensus molecular subtypes (CMS).4 The first group, CMS1, is microsatellite instable and characterised by multiple mutations, hypermethylation and BRAF mutations. The consensus molecular subtypes 2, 3 and 4 (CMS2, CMS3 and CMS4) are chromosomally instable and differ based on their gene expression signal. Most KRAS-mutated colorectal cancers fall within the CMS3 category.4 The recurrent somatic genetic alterations in colon cancer lead to the development of neoplasia by affecting cells through different signalling routes. Genes of the RAS family are usually affected as part of the RTK–RAS signalling pathway.2 Mutations involving the RAS genes are seen in approximately 52% of colorectal carcinoma.5
RAS genes and proteins in the normal state
The RAS family is formed of three genes, KRAS, NRAS and HRAS.6–8 Two of these genes were discovered more than four decades ago as retroviral oncogenes within two viruses: Kristen rat sarcoma virus (KRAS) and Harvey rat sarcoma virus (HRAS).9 NRAS (neuroblastoma RAS viral oncogene) was later discovered as the third member of the family.10
RAS genes code for four isoproteins: K-RAS4A, K-RAS4B, H-RAS and N-RAS, which share 82%–90% sequence identity (figure 1).6–8 These proteins act as a link in the intracellular signal transduction initiated by binding growth factors to cell membrane receptors.6 8 They help mediate signals related to cell survival, senescence and others.6 8 Despite their shared similarity, there is compelling evidence that RAS isoproteins have distinct functions in different tissues in both health state and cancer.6–8 The differences in function are at least partially attributed to the differences in the C-terminal hypervariable region of these proteins.

The basic structure of the KRAS gene (upper diagram). The exons represented by the blue rectangles are the ones that code for proteins. Differential splicing to either include or exclude exon 4a results in the two KRAS isoforms: KRAS4A and KRAS4B. The recommended exons to be included in testing in the previous and current guidelines are highlighted. The lower diagram shows the basic KRAS protein structure with two domains; the G domain (GTP binding domain), which is similar between the four RAS isoproteins (per cent similarity shown, 100% for first 85 amino acids and ~85% for the whole G domain) and the hypervariable region with CAAX motif at the end, forming the membrane targeting part of the protein.
RAS proteins are GTP-binding proteins with relatively weak GTPase functionality that allow these proteins to switch between two states: active (GTP-pound) and inactive (GDP-pound).6–8 This switching mechanism is supplemented by the actions of two classes of proteins: GTPase activating proteins, which helps to ‘switch off’ the signal by hydrolysing and releasing GTP and guanine nucleotide exchange factors, which ‘switches on’ the signal by favouring the formation of RAS–GDP complex.11
Although RAS proteins interact with several effectors, the two major signalling pathways through which RAS proteins exert their function are mitogen-activated protein kinase (MAPK) and phosphoinositide-3 kinase (PI3K). Discussing these pathways is beyond the scope of this review. Figure 2 shows a simplified summary of the RAS protein as a signal transducer and its interaction with the various intracellular effectors, focusing on the MAPK and PI3K pathways.
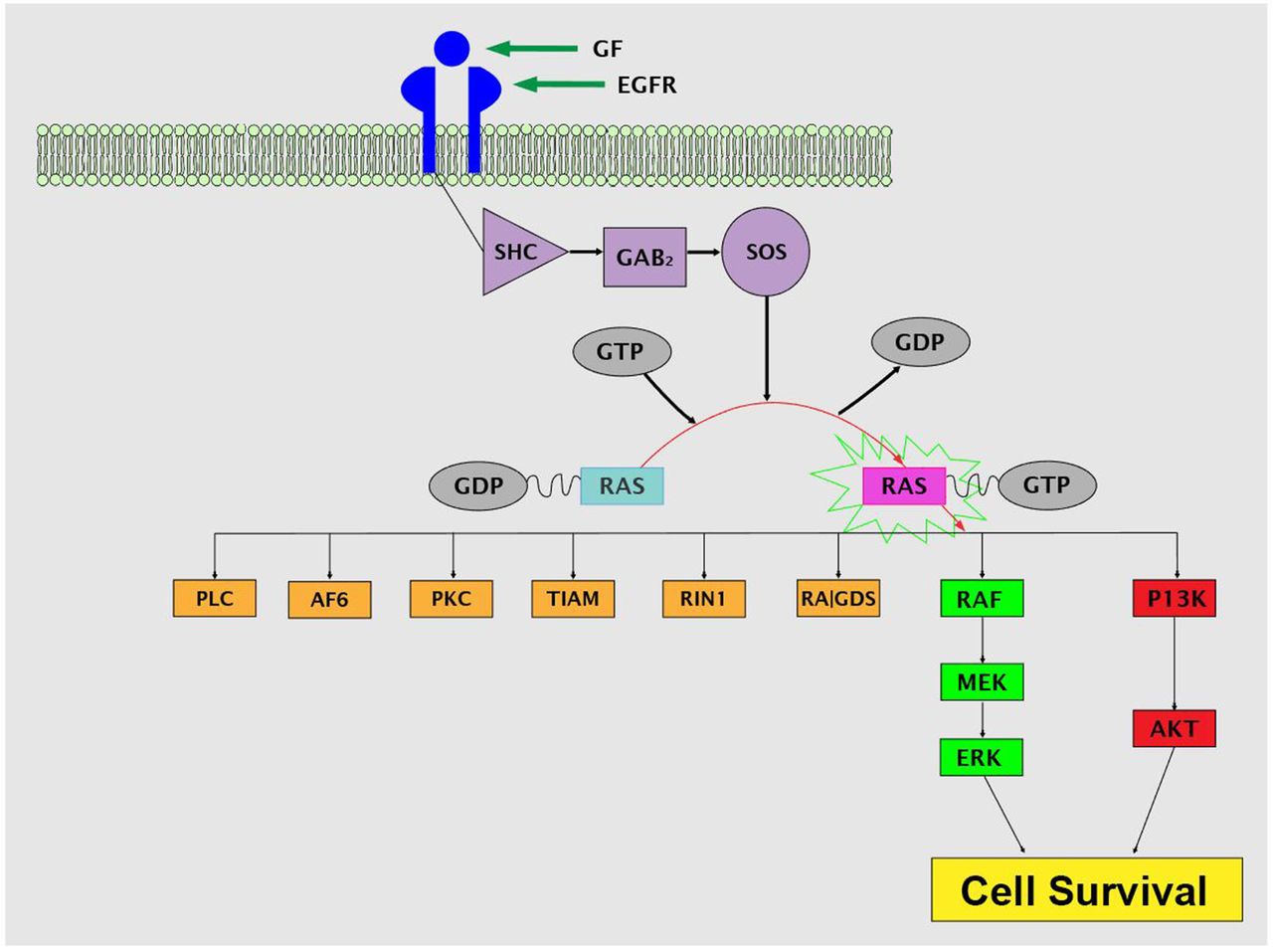
The role of RAS protein as a signal transducer connecting to multiple downstream effectors. The two downstream effector pathways commonly involved in colon cancer pathogenesis and known to mediate cell survival are further detailed. AF6, Afadin, AKT, protein kinase B; eGFR, epidermal growth factor receptor; ERK, extracellular signal-regulated kinase; Gab2: Grb2 associated binding protein 2; GDP, guanosine diphosphate, phospholipase C; GF, growth factor; GTP, guanosine-5'-triphosphate; MEK, mitogen-activated protein kinase; Pi3K, phosphatidylinositol (3,4,5)-trisphosphate; PKC, protein kinase C; RalGDS, Ral guanine nucleotide dissociation stimulator; RAF, rapidly accelerated fibrosarcoma; RIN1, RAS and RAB interactor-1; Shc, Src homolog and collagen; SOS, Son of Sevenless; TIAM, T-lymphoma invasion and metastasis inducing protein.
RAS mutations and colorectal carcinoma pathogenesis
Mutations of RAS genes are among the first mutations to be discovered in malignant tumours. They still represent the most mutated genes in cancers, being found in approximately 25% of all human malignancies.7 RAS genes differ greatly in their mutational frequency among different malignancies with KRAS being the most commonly mutated.6 While KRAS represents approximately 100% of RAS mutations in pancreatic ductal carcinoma, NRAS accounts for 94% of RAS mutations in cutaneous melanoma.6 Despite the presumed functional differences between the three RAS isoforms in health and cancer pathogenesis, mutations affecting these genes usually involve the identical amino acid domains shared by the isoforms.6 Most of RAS mutations occur in only three codons: 12, 13 (exon 2) and 61 (exon 3).6 The remaining few mutations usually involve codons 59 (exon 3) and codons 117, 146 (exon 4).12
KRAS has a contributory role in the development and progression of colorectal adenomas. This conclusion was supported by demonstrating that KRAS mutations are more frequent in large adenomas compared with smaller ones.13
In the setting of colorectal carcinoma, both KRAS and NRAS mutations are frequently encountered in approximately 44.7% and 7.5% of cases, respectively.5 Most of KRAS mutations affect codon 12 and codon 13.2 14 The essential role of KRAS mutations in the carcinogenesis of colorectal cancers has been illustrated by animal studies. In one study, although KRAS mutation alone was not sufficient to initiate colon cancer in mice, an APC-mutated mouse with secondary KRAS mutation developed a significantly larger number of adenocarcinomas with uniform high-grade dysplasia compared with those with wildtype-KRAS genes.15
In addition to the role of KRAS mutations in tumour progression, they seem to play an essential role in tumour maintenance.6–8 Loss of KRAS expression in animal models was associated with increased apoptosis in primary and metastatic colon cancers.16 17 KRAS-mutated colorectal cancers seem to have a specific clinicopathological profile. They tend to affect males and have classical adenocarcinoma morphology, are well or moderately differentiated and are microsatellite stable.14
Testing of RAS mutations in colon cancer: guidelines and new advances
Purpose of testing
Testing for RAS mutations have a proven predictive value in patients with metastatic colon cancer. One treatment modality for patients with metastatic colon cancer is the addition of antiepidermal growth factor receptor (anti-EGFR) monoclonal antibodies, panitumumab and cetuximab, to the standard chemotherapy. These antibodies are known to improve outcome in patients with metastatic colorectal cancer and wildtype-RAS genes (lacking mutations in exons 2, 3 and 4).18
Who should be tested
The American Society for Clinical pathology, College of American Pathologists, Association for Molecular Pathology and the American Society of Clinical Oncology (ASCP/CAP/AMP/ASCO) issued joined guidelines for molecular testing in colorectal cancer in 2017. They recommend that all patients with colorectal cancer considered for anti-EGFR therapy receive extended testing for KRAS and NRAS codons 12, 13, 59, 61, 117 and 146 (table 1).19 The 2018 National Comprehensive Cancer Network (NCCN) guidelines for colon cancer recommends testing for RAS and BRAF in all patients with metastatic colorectal cancer.20
Extended RAS testing in the current guidelinescompared to previous recommended testing.
Type of tissue needed for testing
The NCCN and ASCP/CAP/AMP/ASCO guidelines recommend that either primary or metastatic tumour can be used for testing.20 21 They state in their consensus that both formalin-fixed, paraffin-embedded tissue and cytology specimens after proper validation are appropriate for RAS mutation molecular testing.20 21
Testing methodologies
Various laboratory platforms exist for performing extended RAS testing including allele-specific PCR, PCR high-resolution melting assays, Sanger sequencing and next generation sequencing. These methodologies differ in sensitivity (ranging from 84.4% to 100%) and specificity (ranging from 98% to 100%). The joined guidelines of ASCP/CAP/AMP/ASCO do not favour any of these methodologies if the methodology can detect RAS mutation in specimens with low mutation frequency (5%) (box 1).19 22
Key points from the 2017 ASCO/AMP/CAP guidelines regarding RAS testing in colorectal cancer
RAS genes are the most commonly mutated genes in human malignancy, found in 25% of all cases.
The four RAS isoproteins (KRASA4, KRASB4, NRAS and HRAS) share approximately 80% sequence identity, yet thought to have different roles in health and malignancy.
RAS proteins act as a link in the signal transduction induced by growth factors to promote cell survival.
KRAS and NRAS genes are mutated in 52% of patients with colon cancer, with most of the mutations affecting exon 2.
KRAS mutations have a role in both the development and progression of colon cancer.
According to the latest NCCN guidelines, testing for RAS mutations should be done for all patients with metastatic colon cancer disease.
Testing is preferably performed on metastatic lesions using formalin-fixed, paraffin-embedded tissue. But cytology specimens can be used after proper validation.
Testing should include mutations affecting exons 2, 3 and 4 in both KRAS and NRAS genes (extended RAS testing)
Various testing platforms can be used if they are validated and meet clinical standards.
Testing RAS mutations in liquid biopsy is showing great promise and might replace traditional tissue testing in the near future.
Only patients with wildtype-RAS genes should be considered for anti-EGFR treatment.
Even though decades of research have failed to produce an effective and safe RAS targeted therapy, promising clinical trials are on the way.
Liquid biopsy as a modality for testing
The detection of circulating tumour DNA (ctDNA) from a blood sample is convenient, in theory, and also provides a real-time detection of tumour burden, evolution and heterogeneity. It can be performed on almost every patient, even those with lesions difficult to biopsy.23–25 Recently, the utility of blood-based RAS testing (liquid biopsy) in patients with metastatic colorectal carcinoma showed great promise.25–29 In one study, the use of highly sensitive digital PCR (BEAMing) showed a 90.4% positive agreement, 93.5% negative agreement and 91.8% concordance compared with tissue-based RAS testing.30
Many studies have also shown that detecting KRAS mutation in liquid biopsy postoperatively in patients with colon cancer strongly predicts disease recurrence.25–27 Serial measurement and analysis of ctDNA in patients with colon cancer have also been shown to help both on the assessment of treatment response and the detection of the emergence of treatment resistance.27 28 30
KRAS mutations as prognostic biomarker
Several articles investigated the prognostic value of mutations affecting different codons and alternative mutations affecting the same codons of KRAS gene in the prognosis of patients with colon cancer.21 Patients with mutations involving codons 12 and 61 usually fare worse than those with other mutations,31–37 while mutations in codon 146 are associated with a better outcome.31 While the adverse prognostic effects of mutations involving exon 2 are supported by multiple studies, conflicting results regarding the differences in outcome between the common exon 2 mutated codons, 12 and 13, are seen in the literature.38 Unlike in pancreatic adenocarcinoma, in colorectal cancers, studies failed to show a significant outcome difference between G12D and G12V mutations affecting codon 2.31
RAS-targeted therapies
RAS proteins have always been thought of as potential therapeutic targets due to their critical role in the development of many malignancies including colorectal cancer.39–42 Despite that, more than three decades of research have failed to produce an effective and safe drug that can target RAS proteins.43 This failure is at least partially attributable to the biochemistry of RAS proteins. RAS proteins have a relatively smooth shape that hinder drug attachment, rendering direct targeted therapy difficult.43 Figure 3 shows some of the key categories of direct RAS drugs/experimental molecules and their timeline since RAS discovery until now.

{kind=link}
{kind=link}
{kind=link}
The timeline for the key direct RAS drugs since the discovery of RAS gene mutations in human malignancy and until now. This is not meant to be an exclusive list of the large number of experimental drugs that have been discovered, but a simplified timeline for the main drug and drug categories.
Recent advances have shown that GTP is so tightly bound to RAS proteins that it is nearly impossible for small molecular inhibitors to displace GTP.44 Therefore, novel approaches to discover direct RAS inhibitors have been developed for codon 146 (figure 3).45–48 One of these approaches is to use drugs that target the mutated sites in the KRAS gene. These drugs hinder the formation of the GTP-bound activated KRAS proteins. Examples of these are experimental drugs that interfere with the reaction of the mutant KRAS G12D with SOS1 (one of the guanine nucleotide exchange protein) preventing the formation of KRAS–GTP.49 Others target the cysteine amino acid in KRAS G12C, blocking the activation of RAF and inducing apoptosis in tumours harbouring such mutations.47 48 50 Brito et al suggested another approach through targeting the guanine-rich G4 structure in the KRAS promotor region leading to decreased cell proliferation and increased apoptosis.51 A third interesting approach is the use of miRNA to silence and suppress KRAS-dependent cell growth both in vivo and in vitro.5 52 In 2017, Welsch et al published their discovery of a small multivalent molecule capable of binding the active RAS–GTP protein and preventing the downstream interaction with effector proteins. As they explained in their article, this molecule showed toxic effect of target activity, necessitating further workup and development (box 2).53
Extended RAS testing in the current guidelines compared with previous recommended testing
Testing should be done in all patients with metastatic colon cancer disease considered for anti-EGFR therapy.
Testing is preferably performed on metastatic lesions using formalin-fixed, paraffin-embedded tissue or cytology specimens after proper validation.
Testing should include mutations affecting exons 2, 3 and 4 in both KRAS and NRAS genes (extended RAS testing).
Various testing platforms can be used if they are validated and meet clinical standards.
A recent article in the New England Journal of Medicine showed a promising new approach to treating metastatic colorectal cancer using immunotherapy.54 The authors reported regression in a case of metastatic colon cancer after infusion with KRAS-mutant-specific T-cells, giving new hope for the use of immunotherapy as a potential treatment modality for metastatic colon cancer.54 Despite the tremendous efforts and extensive research over the last few decades, there is still no effective drug targeting mutated RAS genes whether directly or indirectly.55
Summary
Mutations in KRAS and NRAS are seen in approximately 52% of colorectal cancers, commonly involving codons 12, 13 and 61. RAS gene structures and functions have been thoroughly studied and described since their discovery decades ago. Their role in the pathogenesis of malignancy, including colon cancer cases, has been supported by many studies including animal models. The extended testing for KRAS and NRAS mutations is now the standard of care in patients with stage IV colon cancer considered for anti-EGFR monoclonal antibodies. Despite decades of futile attempts to synthesise a safe and effective RAS targeted therapy, the last few years showed a renewed interest and significant progress on new and novel approaches to target KRAS mutated tumours.
References
Footnotes
Handling editor Des Richardson.
Correction notice This paper has been corrected since it was published Online First. Figure 2 and 3 legends were accidentally switched and this has now been rectified.
Contributors OS drafted the article. LC formulated and designed the topic of this review. All the authors critically read, edited and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.