Article Text

Abstract
Endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS-FNAB) is the optimal method for sampling lesions of the pancreas. This procedure is being performed at increasing numbers of hospitals and therefore, more and more cellular pathology departments are having to process and report EUS-FNAB specimens. This article outlines the advantages of using tissue/cell block preparation to process these specimens. In particular, such preparation concentrates, conserves and preserves sampled material which is then available for a full array of further analyses. Tissue/cell block preparation also enables EUS-FNAB specimens to be assessed by a wider range of cellular pathologists. This article demonstrates how a tissue/cell block protocol permits the diagnosis of the full range of pancreatic pathologies sampled by EUS-FNAB. The protocol is identical for all these pathologies (including both solid and cystic lesions) and is simple at all stages of the specimen pathway, from collection to processing to assessment.
- endoscopic ultrasound
- fine needle aspiration
- pancreas
- histopathology
- immunohistochemistry
Statistics from Altmetric.com
Introduction
Endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS-FNAB) is well accepted and established as the optimal method for sampling lesions of the pancreas for pathological analyses.1 Because EUS-FNAB was initially performed just by a few clinicians working in tertiary referral centres usually with hepatopancreaticobiliary (HPB) surgical units, these specimens were only received by the few cellular pathology departments that served these centres. However, more and more endoscopists are now performing EUS-FNAB in a wider range of hospitals. Therefore, equally more cellular pathologists and their departments now need to process and assess these specimens. The needles used for EUS-FNAB were initially of a narrow calibre and because the resulting samples usually comprised cells rather than intact tissue, the samples were traditionally prepared as cytology specimens and assigned to cytopathologists.2 However, the wider bore needles now being used are designed to preserve tissue architecture1 and the resulting tissue fragments and whole cores can therefore be processed differently and potentially reported by a wider range of cellular pathologists. This author responded to the local introduction of EUS-FNAB (as one of the first UK centres to provide the service) by exploring different methods of preparing the specimens and subsequently has accumulated more than 10 years of experience in assessing these pancreatic samples. The following article aims to share this experience particularly with the increasing range of pathologists who more recently are assessing EUS-FNAB specimens. In particular, the article outlines the preparation technique favoured by the author for these specimens and how a full range of pancreatic pathologies can thus be diagnosed.
Processing of EUS-FNAB specimens
EUS-FNAB specimens were traditionally prepared as cytology specimens, therefore using techniques such as direct smears, cytospin and liquid-based cytology (LBC) methods.3 Furthermore, direct smears were encouraged by the initial enthusiasm for rapid on-site evaluation (ROSE). This evaluation was promoted to ensure adequate cellularity was achieved in EUS-FNAB samples2 especially when narrower needles yielded less cellular material. However, ROSE is no longer recommended as essential by more recent guidelines.1 There have been randomised controlled trials which showed ROSE not to improve EUS sampling, and meta-analyses on this subject have produced conflicting findings.1 The reduced need and demand for ROSE may relate to the use of wider bore needles which are therefore more likely to ensure sampling of diagnostic material and/or the realisation that concentrating all of an aspirated sample into one specimen may prove more diagnostic than splitting the aspirate between an on-site preparation and subsequent specimens.
The fact that these wider needles now yield tissue fragment and cores has led to the use of tissue/cell block techniques for EUS-FNAB specimens. Indeed, based on observational studies of sampling pancreatic or subepithelial masses or lymph nodes, preparing EUS-FNAB specimens as tissue/cell blocks is now recognised as superior to direct smears and LBC, in terms of sensitivity, accuracy and negative predictive value.1 There are much less data on whether tissue/cell block preparation can be successfully applied to EUS-FNAB samples from pancreatic cystic lesions. However, this author has recently documented that, with such samples from pancreatic mucinous cysts, tissue/cell block preparation is superior to direct smears in demonstrating mucin and shows higher diagnostic sensitivity than cyst fluid carcinoembryonic antigen (CEA) biochemistry.4 The author is not aware of any published direct comparison between tissue/cell block preparation and cytospin and/or LBC for processing EUS-FNAB samples from pancreatic cystic lesions. However, tissue/cell block preparation has several advantages (see also box 1) over the latter two in this context. The preparation of one or, at most, two tissue/cell blocks from one EUS-FNAB specimen concentrates all its contents. There is no need to divide the specimen for various analyses, and the same tissue/cell block can be used for morphological assessment, histochemistry, immunohistochemistry and genetic analyses; this not only conserves specimen material but is also invaluable when a pathologist wants to be certain that the same cells in a haematoxylin and eosin (H&E)-stained section are showing a particular immunoprofile. By contrast, cytospin and LBC techniques will not concentrate all of a specimen’s contents if further analyses are anticipated and also have to split the specimen contents across different analyses; in addition, LBC protocols may remove mucus/mucin.5 Tissue/cell blocks are the optimal preparation for immunohistochemistry, whereas such analysis on cytospin and LBC samples can be substandard due to background artefact or interference with some antigens6 7; this is pertinent to that fact that some pancreatic cysts are actually cystic variants of solid neoplasms (eg, neuroendocrine tumour (NET))3 which are best diagnosed with immunohistochemistry. With the simple tissue/cell block protocol proposed for all pancreatic EUS-FNAB specimens (see below), there is no need for specialist and more costly reagents and equipment (eg, commercial fixatives and cytospin or LBC machines). The EUS-FNAB material is more conveniently stored as paraffin-embedded blocks for later additional testing; in particular, DNA will be available and better preserved for targeted gene analyses, for example, KRAS and GNAS genotyping. Finally, tissue/cell block preparations yield stained tissue sections which are more familiar and accessible to non-cytopathologists; pancreatic EUS-FNAB specimens can thus be reported by HPB histopathologists (who report pancreatic resections and are usually the pathologists who attend HPB multidisciplinary team meetings where EUS-FNAB results ae discussed) but also a wider range of cellular pathologists in less-specialist centres.
Advantages of the tissue/cell block preparation protocol for endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS-FNAB) specimens from the gastrointestinal tract, including the pancreas
Automatically and always concentrates EUS-FNAB material.
Conserves material because the same tissue/cell block can be used for multiple analyses.
Permits direct comparison of the same cells between multiple analyses.
Best for immunohistochemistry.
Does not require costly reagents and laboratory equipment.
Best for long-term storage of material which is therefore available for retrospective analyses.
Stores DNA for retrospective genetic analyses.
Permits assessment by a wider range of cellular pathologists.
Simple preparation protocol for EUS operators.
Simple processing protocol for cellular pathology departments.
Identical protocol for all lesions, regardless of nature and location in the gastrointestinal tract.
Having trialled commercial fixatives marketed for cytological specimens and other preparation techniques (including direct smears and cytospin) when EUS-FNAB samples were initially submitted to the author’s department, the latter has settled on and been using the following protocol for the past 7 years. Over these years, the local endoscopists have generally used 22G needles for lesions accessed via the duodenum and 19G needles for transgastric EUS-FNAB when there is less scope angulation. Over the last 2 years, Boston Scientific Acquire needles have been predominantly used but before this Cook Medical ProCore needles were used.
Regardless of whether the pancreatic lesion is solid and/or cystic and regardless of the nature of the EUS-FNAB material (eg, mainly fluid or abundant tissue fragments), all this material is ejected directly from the EUS needle into a single container and fixed with 30–40 mL of 10% neutral buffered formalin. This volume of formalin also allows the needle to be agitated/washed within it to release any material still adhering to the needle. When the specimen is received at the cellular pathology department, any cores/tissue fragments which can be picked out with forceps are processed as a separate cassette (using the conventional protocol for cores/biopsies) to produce a paraffin-embedded tissue block. The remainder of the formalin-fixed sample is then spun down and processed as a paraffin-embedded cell block. The cell block is always worth processing and assessing even when abundant tissue appears to have been blocked separately because the author has reported a few cases where diagnostic material (eg, of adenocarcinoma) was present only in the cell block and not in the core/tissue fragment block. The author’s department used an agar-embedding method and then a thrombin clot method for preparing cell blocks, and there have been no obvious differences in the resulting sections.
This tissue/cell block protocol is particularly attractive because of its simplicity and identical application to all EUS-FNAB specimens regardless of the location and nature of the targeted lesion. With regard to the latter, it has already been noted that pancreatic cysts may actually represent cystic variants of solid tumours, but there are also solid variants of pancreatic cystic neoplasms (eg, solid serous adenoma). The same protocol is used if the specimen is a repeat attempt at tissue sampling because, as discussed above, the tissue/cell block protocol maximises the diagnostic yield of an EUS-FNAB specimen and, in the author’s opinion, adequacy of an EUS-FNAB specimen is more dependent on EUS operator technique, accessibility of the target and/or patient tolerance to the procedure. Finally, the same protocol is used regardless of the suspected type of neoplasm (eg, carcinoma vs lymphoma).
The ‘poor man’s cell block’ is a novel method of fixing aspirated material (by formalin fumes rather than immersion in formalin) to form one or more pellets which can then be directly processed into paraffin-embedded blocks.8 This method has been successfully applied to EUS-FNAB material from solid and cystic pancreatic lesions (Tim Bracey, personal communication). The author plans to trial it locally especially because it avoids diluting and then re-concentrating EUS-FNAB material and it requires even less processing on receipt by the cellular pathology laboratory.
The contents of this article hereafter are based purely on EUS-FNAB specimens processed as tissue/cell blocks. This is not intended to exclude readers who are already assessing these specimens with more traditional cytological techniques, but to demonstrate an alternative technique with the above-mentioned advantages and attractions. Furthermore, the article intends to provide a knowledge base for those pathologists (especially non-cytopathologists) who are about to or have just begun receiving EUS-FNAB specimens. The article will cover such specimens from within and also around the pancreas because the two may produce overlapping differential diagnoses and it can be difficult, at EUS, to determine the exact location of a lesion in relation to the pancreas. EUS-FNAB specimens derive not just from pancreatic and peri-pancreatic lesions but also mediastinal, oesophagogastric and rectal lesions. The remit and length of this article preclude discussion of the latter three categories, but the above-mentioned tissue/cell block protocol has been identically and successfully used for all EUS-FNAB and also endobronchial ultrasound-derived specimens submitted to the author’s department.
Assessment of EUS-FNAB specimens
The author’s department insists that an EUS-FNAB specimen will only be processed and assessed if accompanied by a copy of the EUS report. This report can be crucial to the interpretation of histological findings. Clinical data that can be crucial this way have been listed elsewhere9 but include: a patient’s history of extra-pancreatic malignancy such as melanoma (see below); evidence of chronic pancreatitis (to support a diagnosis of pseudocyst); whether the lesion was solid or cystic or both; the macroscopic appearance of the aspirated fluid.
The department routinely issues three H&E stained sections for each EUS-FNAB specimen block. Unlike unprocessed cytospin or LBC specimen material, paraffin blocks (including those of EUS-FNAB specimens) are stored indefinitely by the department.
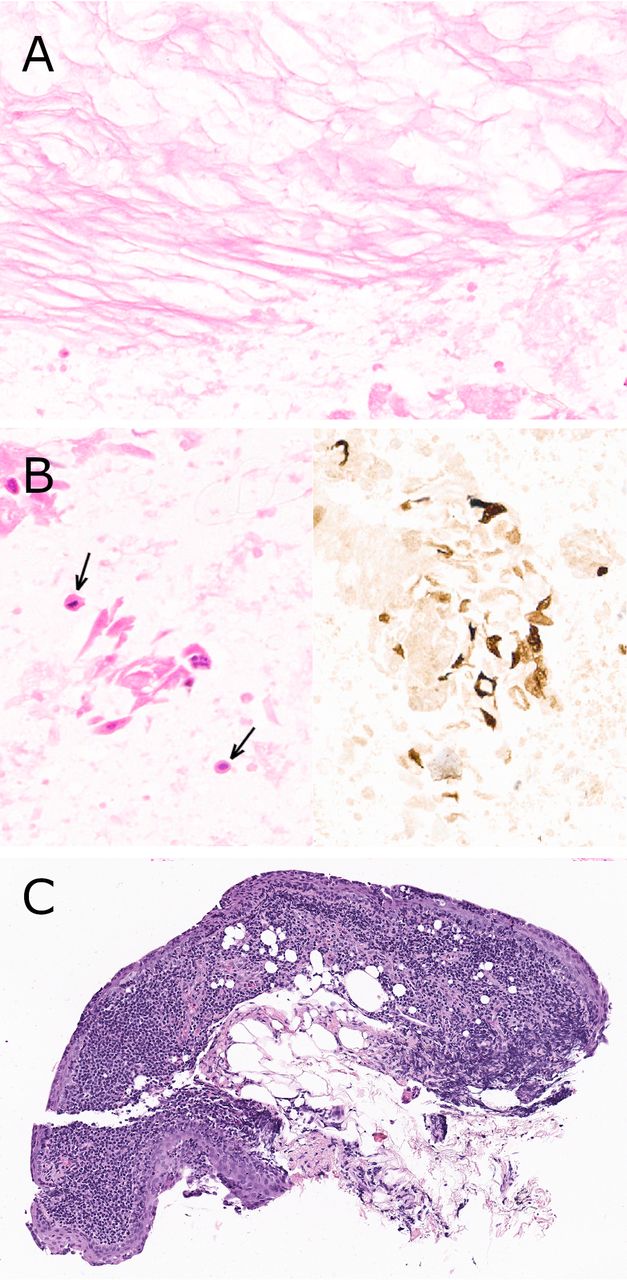
The pathologist assessing pancreatic/peri-pancreatic EUS-FNAB specimens should always bear in mind several cell types which may potentially contaminate these specimens and which should not be mistaken for a pathology. Oesophageal squames are discussed further below. The EUS report should state the route of the aspirating needle, though in the absence of this information, pancreatic body and tail lesions are usually sampled through the stomach whereas head/uncinate lesions are through the duodenum. Pancreatic neck lesions and some more superior head lesions may be sampled through the duodenal bulb, the pylorus or the gastroduodenal junction. The author has found that most EUS-FNAB specimens contain strips of glandular epithelium and/or larger mucosal fragments from the organ traversed by the needle. Another cell population that can contaminate transgastric EUS-FNAB specimens is mesothelium, presumably lining one or both sides of the lesser sac. These mesothelial strips may not catch the pathologist’s attention if scanty and sectioned through their thinnest plane. On the other hand, if reactive and/or present as sheets enface (figure 1A), contaminating mesothelium could be mistaken for neoplastic cells. However, provided a pathologist considers the possibility of such contamination, a mesothelial phenotype can then be confirmed easily with immunohistochemistry (figure 1B).

(A) Two clusters of contaminating mesothelial cells whose nature were confirmed by their immunopositivity for CK5/6, WT1 and (B) calretinin; the latter stain only showed non-specific staining of a strip of foveolar epithelium which also contaminated this transgastric aspirate of a pancreatic body lesion.
In its following, more specific discussions of how EUS-FNAB specimens are assessed, the article will not outline every morphological, immunohistochemical and genetic characteristic of every pancreatic pathology, but instead will discuss those pathologies most likely to be sampled by EUS-FNAB and their features in these specimens which particularly help indicate their diagnoses. To help structure the article, pancreatic and peripancreatic lesions are discussed using the traditional subcategories of solid and cystic lesions, though overlap between these two categories is already noted above.
Solid lesions
Primary neoplasia
Adenocarcinoma
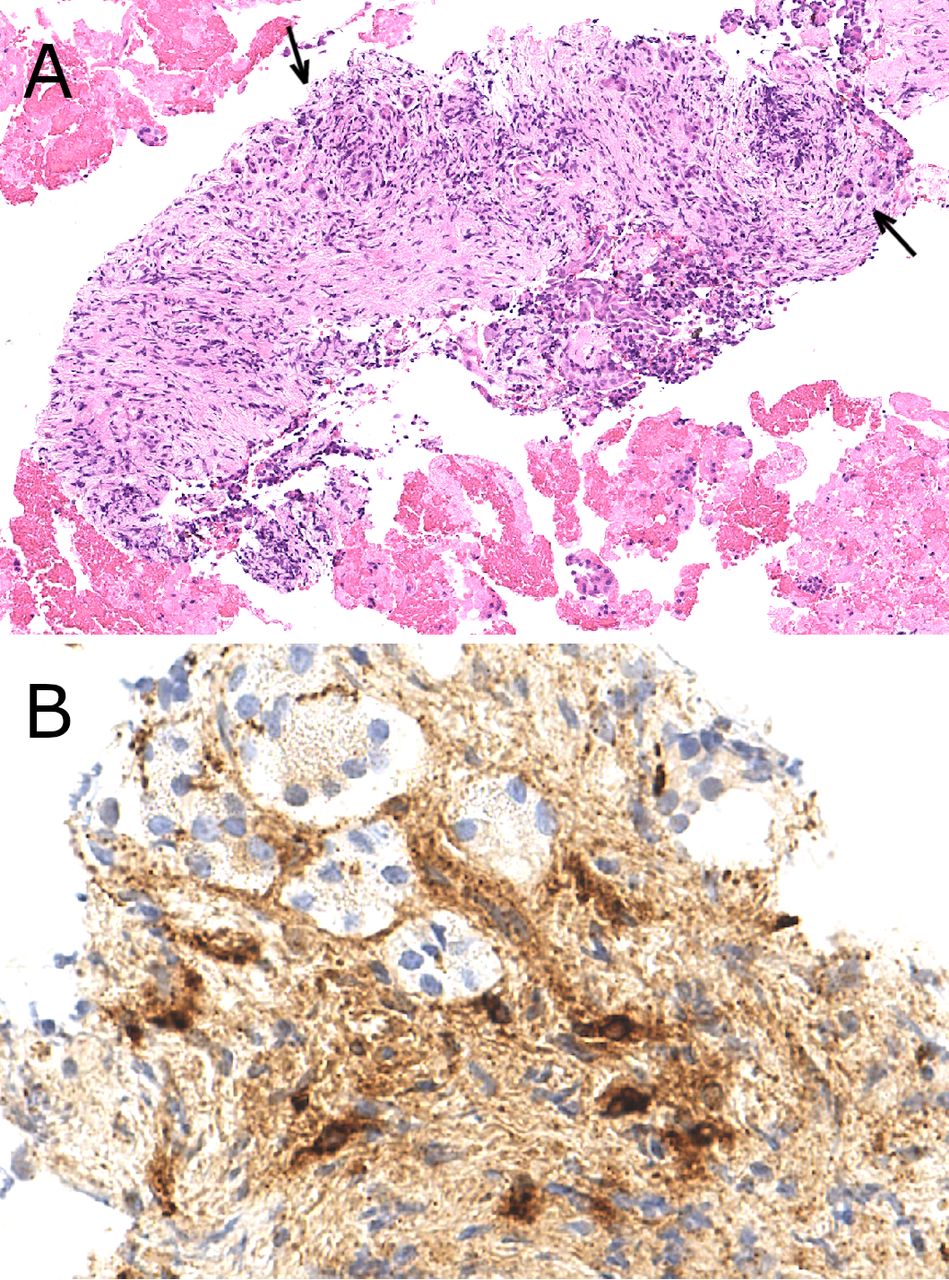
It is not yet possible to distinguish between pancreatic ductal adenocarcinoma (PDAC), cholangiocarcinoma and ampullary carcinoma in EUS-FNAB material especially from pancreatic head tumours. The following therefore considers these together as primary pancreaticobiliary adenocarcinoma. The author’s experience is that EUS-FNAB material from such adenocarcinoma tends to fall into one of four categories according to how much is sampled: (1) stromal fragments containing neoplastic glandular epithelium (figure 2A); (2) a cellular sample with free-floating neoplastic glandular epithelium but no stromal invasion demonstrable (figure 2B); (3) a hypocellular sample with only scattered (ie, no more than two to three) strips of atypical glandular epithelium and (4) no neoplastic glandular epithelium.

(A) Sampling of a pancreatic adenocarcinoma comprising neoplastic glands infiltrating the left side of the tissue core and free-floating neoplastic epithelium at the bottom of the panel; the arrows delineate remnant intralobular ducts and emphasise their retained organoid arrangement. (B) A free-floating strip of glandular epithelium showing pleomorphic, non-polarised nuclei and both apoptotic (examples arrowed) and mitotic (in the bottom right corner) figures as well as ‘bubbly’ cytoplasm (seen best in the centre of the panel); the strip was therefore regarded as neoplastic and supportive of a diagnosis of adenocarcinoma if a solid lesion had been sampled. (C) Sampling of a primary pancreatic carcinoma showing only squamous differentiation. (D) Grade 3 neuroendocrine carcinoma (Ki67 labelling index >90%) with small cell morphological features including prominent apoptotic bodies (examples arrowed) and focal nuclear smearing (inset). (E) Acinar cell carcinoma showing amphophilic to basophilic cytoplasm and pseudoacini, with (F) widespread trypsin immunopositivity.
Not surprisingly, the first category is the easiest to report though well-differentiated adenocarcinoma should not be confused with smaller, physiological glands and especially intralobular ducts which remain after acinar tissue has atrophied in chronic pancreatitis. In this context, adenocarcinoma is favoured by nuclear pleomorphism and mitotic activity, whereas residual intralobular ducts are favoured by an organoid arrangement (figure 2A). Perineural invasion is occasionally demonstrated in EUS-FNAB cores/fragments but the author has only rarely identified lymphovascular invasion. Desmoplastic stroma is not a reliable indicator of adenocarcinoma because similar fibrotic stroma can be seen in chronic pancreatitis alone.
Correlation with EUS findings is crucial when interpreting the second category, especially as free-floating neoplastic glandular epithelium could represent the dysplastic lining of a cystic lesion (figure 3B) rather than carcinoma. If the EUS operator has clearly stated that the sample derived from a solid (hypoechoic) lesion, the author reports this category of specimens as ‘not diagnostic of malignancy by itself but supportive of adenocarcinoma only if the specimen was from a solid lesion’. Contaminating physiological gastric or duodenal epithelium (see above) can serve as a useful population to compare against suspected neoplastic glandular epithelium. When the distinction between the two is less obvious and/or the atypical epithelium is acutely inflamed, the following features favour neoplastic epithelium: nuclear pleomorphism, loss of nuclear polarity, mitotic and apoptotic figures and ‘bubbly’ cytoplasm (figure 2B). The latter is an anecdotal observation of the author, is speculated to represent abnormal packaging of mucin in the cytoplasm of neoplastic glandular epithelium, and has only very rarely been seen in reactive/regenerative intestinal or pancreaticobiliary epithelium.

Examples of (A) low-grade and (B) high-grade dysplastic epithelium in EUS-FNAB samples from MCLs. (B) In isolation, the morphological features of free-floating, high-grade dysplastic epithelium are potentially indistinguishable from those of adenocarcinoma (see figure 2B) and therefore, must always be interpreted in the context of the lesion sampled, for example, cystic versus solid, showing invasion of peripancreatic structures. (C) This foveolar-like mucinous epithelium from an MCL shows less obvious dysplasia than seen in (A) but it shows both (D) neutral and acidic mucin within its apical vacuoles; the presence of the acidic mucin in this foveolar-like epithelium defines ‘mismatched epithelial mucin’. EUS-FNAB, endoscopic ultrasound-guided fine-needle aspiration biopsy; MCL, mucinous cystic lesion.
The third category is hypocellular and usually lacks much, if any, contaminating physiological epithelium, which further hampers interpretation of the scattered atypical strips. The author reports these cases as ‘raising a possibility of glandular neoplasia’. While some may argue that this statement is not insightful from a purely diagnostic perspective, the statement is worded purposely to maintain or trigger investigations for malignancy, for example, repeat EUS-FNAB.
The fourth category is included to prompt discussion of how many sections should be examined of EUS-FNAB specimens which appear to be non-diagnostic. In truth, the answer is as unclear as for how many deeper levels should be cut when endoscopic biopsies of a lesion do not show any pathology. There is unlikely to be an answer that applies to all departments because it is dependent especially on how far a block is trimmed into before the first H&E sections are cut. However, the author had encountered a case where neoplastic epithelium was only visualised in the eighth section (ie, after the first three routine sections and then the fourth deeper level). Therefore, if a specimen represents sampling of a tumour suspected by EUS but the first three routine sections show no neoplasia, the author will always assess six deeper levels and if these show no additional features, only then report the specimen as non-diagnostic of neoplasia.
Other carcinomas
In addition to or instead of glandular differentiation, pancreaticobiliary carcinomas may less commonly show a squamous or neuroendocrine phenotype (figure 2C,D). The former can easily be confirmed with immunohistochemistry, for example, for CK5/6 and p63 or p40. While there are genetic differences between PDAC and adenosquamous carcinoma,10 the author has not yet seen an adenosquamous carcinoma diagnosis change a patient’s management from that for conventional adenocarcinoma. By contrast, chemotherapy regimens differ between PDAC and neuroendocrine carcinoma (NEC), the latter being managed with platinum-based drugs.11 There are increasing data showing that the small and large cell subtypes of pancreatic NEC are closely related and therefore, may be managed similarly.11 12 It is beyond the remit of this article to discuss how much positivity of how many of which neuroendocrine markers distinguishes NEC of particularly large cell type from PDAC. One useful marker for supporting a diagnosis of NEC (regardless of a lung or extrapulmonary origin) is TTF-113 14 but while the literature suggests PDACs do not express this transcription factor,14 15 the author has seen rare exceptions to this rule.
Two specific but rare subtypes of primary pancreatic carcinoma are acinar cell carcinoma and anaplastic carcinoma with osteoclast giant cells. The former should be suspected on morphological grounds (eg, eosinophilic or basophilic cytoplasm, and arrangement as sheets or pseudoacini/clusters) and can most easily be confirmed by trypsin or chymotrypsin immunohistochemistry (figure 2E,F). The author believes that cellular pathology departments receiving pancreatic resections and a high volume of EUS-FNAB specimens should routinely stock one of these two immunomarkers and favours a Merck-Millipore trypsin monoclonal antibody (MAB1482) especially because of its clean staining. Anaplastic carcinoma with osteoclast giant cells can be diagnosed from EUS-FNAB material by a mixture of morphological (especially the giant cells) and immunohistochemical (absence of immunopositivity for most markers) features.
Neuroendocrine tumour
The fact that these tumours usually yield very cellular specimens is an initial clue to the diagnosis (figure 4). While EUS-FNAB can yield fragments or cores of intact NET, these neoplastic cells are more commonly found as free-floating islands or more dissociated among blood (figure 4A). In the latter state, they can be confused with dispersed acinar cells from background pancreas though the two can be distinguished with immunohistochemistry for chromogranin, synaptophysin (figure 4B) and if available, an acinar cell marker like trypsin (ie, another reason for stocking this immunomarker). The author continues to resist requests to grade a NET from EUS-FNAB material particularly as the tumour will usually be resected and could then be more confidently graded. However, tissue/cell blocks allow for good enough preservation of cell morphology to distinguish between NET and NEC and, if needed and in the author’s experience, Ki67 labelling should help distinguish between NEC (labelling index usually >90%) and even Grade 3 NET (usually <60%).

(A) EUS-FNAB specimens of pancreatic neuroendocrine tumours are typically hypercellular though the neoplastic cells are often dispersed among blood. (B) Immunohistochemistry for neuroendocrine markers such as synaptophysin will confirm the hypercellularity of these specimens. EUS-FNAB, endoscopic ultrasound-guided fine-needle aspiration biopsy.
Solid pseudopapillary neoplasm
Like with NET, solid pseudopapillary neoplasm can yield a cellular EUS-FNAB sample. This cellularity often permits retention of a pseudopapillary architecture (figure 5A). The diagnosis is easily confirmed through its more specific immunohistochemical characteristics such as nuclear beta-catenin positivity, dot-like CD10 positivity (figure 5B,C) and progesterone receptor (PR) positivity.

(A) The pseudopapillary architecture of this solid pseudopapillary neoplasm is clearly shown. The neoplasm shows (B) diffuse nuclear beta-catenin positivity (more easily seen and distinguished from cytoplasmic staining among the dispersed cells) and (C) focal CD10 cytoplasmic dot positivity (examples arrowed).
Secondary neoplasia
Demonstration of squamous cell carcinoma in an EUS-FNAB sample of a pancreatic tumour should prompt consideration of a possible metastasis to the pancreas instead; however, the author has not yet knowingly encountered the latter scenario in a pancreatic resection or EUS-FNAB specimen.
By contrast, two malignancies which show a predilection for metastasising to the pancreas are melanoma and renal cell carcinoma (RCC). Insisting an EUS-FNAB specimen is always submitted with its EUS report will help ensure the assessing pathologist is aware of the possibility of metastatic neoplasia. This is particularly important for melanoma in view of its wide range of potential morphologies and therefore differential diagnoses which would otherwise need excluding. The only subtype of RCC that the author has seen in pancreatic resection and EUS-FNAB specimens is the clear cell variant (figure 6A). Theoretically, the glycogen-filled cytoplasm of this variant could morphologically mimic serous cystadenoma (SCA). However, compared with RCC, SCA typically produces a more hypocellular EUS-FNAB specimen with smaller and more monomorphic and hyperchromatic nuclei, and in the author’s experience, less obvious clear cytoplasm (see below and figure 7A). In the rare event of morphological indecision, immunopositivity for CD10 and PAX8 will help confirm the diagnosis of RCC (figure 6B).

A fragment of metastatic renal cell carcinoma to the pancreas. The neoplasm shows (A) widespread clear cell morphology with the typical delicate vasculature (arrowed) of renal cell carcinoma as well as (B) widespread PAX8 immunopositivity.

(A) High-power view of a cluster of SCA cells with monomorphic, hyperchromatic nuclei; if more dispersed, these nuclei may be mistaken for lymphocytes (example arrowed). (B) Low-power view of a characteristically hypocellular specimens derived from aspiration of SCA but showing how inhibin immunohistochemistry can help identify scattered neoplastic cell clusters (arrowed). (C) Less commonly in EUS-FNAB specimens, SCA cells can demonstrate cytoplasmic glycogen in the form of PAS positivity (examples arrowed) which is removed by diastase treatment. EUS-FNAB, endoscopic ultrasound-guided fine-needle aspiration biopsy; PAS, periodic acidic Schiff; SCA, serous cystadenoma.
On rare occasions, the author has been asked to comment whether the adenocarcinoma in the EUS-FNAB sample of a pancreatic lesion represents PDAC or a metastasis from the patient’s concurrent or previous colorectal carcinoma (CRC). While ‘dirty necrosis’ is characteristic of the latter, this histological feature can also be shown by PDAC,16 and morphological assessment and most immunoprofiling are still not able to confidently distinguish between these two differential diagnoses. Both SATB2 and gpA33 appear to be expressed by CRC and not pancreaticobiliary adenocarcinoma15 17 18 but most pathologists will not yet have ready access to either immunomarker. Genetic profiling of the primary CRC vs the EUS-FNAB material (made particularly feasible by tissue/cell block preparation) may be helpful; it is recognised that both CRC and PDAC can harbour KRAS and p53 mutations but it would be unusual for CRC and PDAC in the same patient to harbour identical, somatic variants in both these genes.
Other solid lesions
A clue to splenunculus being sampled by EUS-FNAB is the lesion’s location in the pancreatic tail or body. If the aspirated tissue is intact and large enough, splenic tissue architecture can be recognised (figure 8A) and immunohistochemistry—especially CD3-positive endothelium within the red pulp—will help confirm splenic tissue (figure 8B,C). A mixture of morphological and immunohistochemical features should also exclude nodal tissue; furthermore, the author believes truly intrapancreatic nodes are much rarer than intrapancreatic splenunculi. Lymphoid tissue might prompt the pathologist to consider lymphoma. However, the more likely differential diagnosis morphologically would be a low-grade lymphoma and, even before immunohistochemistry is used to make the distinction, it would be highly atypical for such a lymphoma to present as an intra-pancreatic lesion without neighbouring lymphadenopathy.
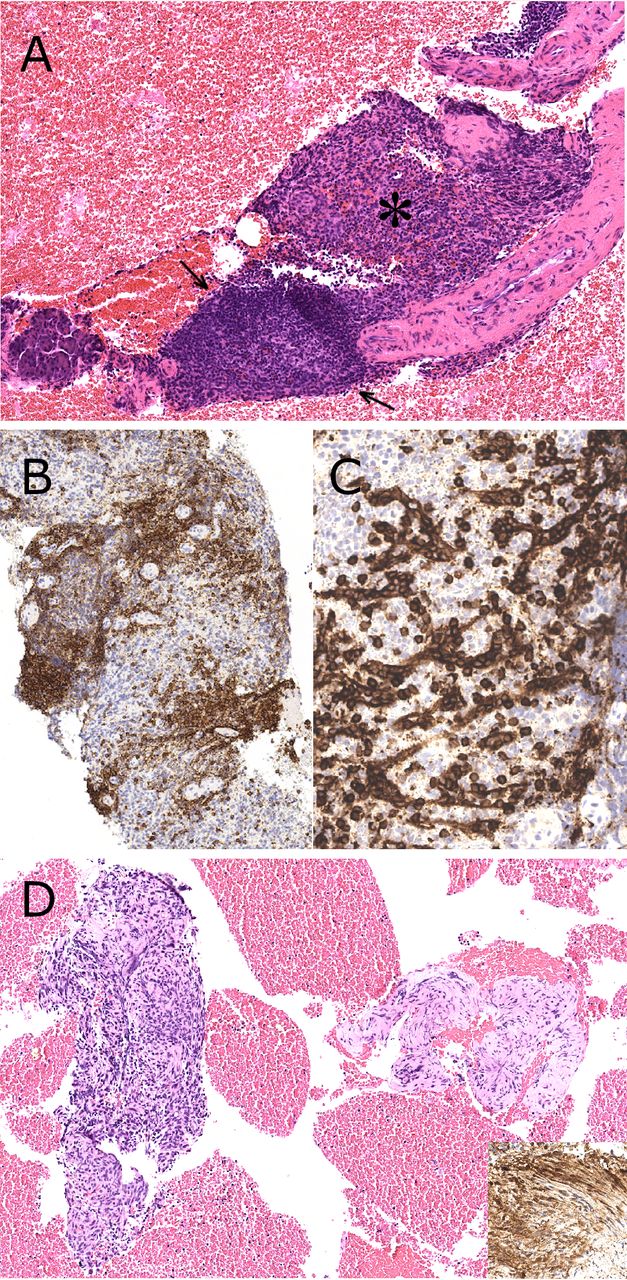
(A) Sampling of this intrapancreatic (background acinar tissue in the bottom left corner) lesion showed splenic tissue with fibrous trabeculae containing vessels, and distinct red pulp (*) and periarteriolar white pulp (including a lymphoid follicle between the arrows). (B) CD20 helped demonstrate the B-cell component of the white pulp but splenic tissue was confirmed by the (C) CD3-positive endothelial cells of the red pulp which highlighted its capillary network; a splenunculus could therefore be diagnosed. (D) Two fragments of a peri-pancreatic schwannoma showing hypercellular (left side of the panel) Antoni A and hypocellular Antoni B areas with diffuse S100 positivity (inset).
Other solid lesions in or around the pancreas that the author has received EUS-FNAB specimens from include gastrointestinal stromal tumour (strongly supported by diffuse positivities for DOG1 and CD117); and schwannoma (diagnosed by morphology and diffuse S100 positivity, figure 8D).
Cystic lesions
Intraductal papillary mucinous neoplasm and mucinous cystic neoplasm
The more generic term mucinous cystic lesion (MCL) will be used hereafter to include both intraductal papillary mucinous neoplasm (IPMN) and mucinous cystic neoplasm (MCN). This is particularly because, with rare exceptions (see below), it is difficult to distinguish between these two entities in EUS-FNAB specimens. The assessment of an EUS-FNAB specimen for MCL can be divided into that for mucin and that for cellular material. The author demonstrated, in a recent and predominantly prospective study, that tissue/cell block preparation is superior to direct smears in demonstrating mucin in this context.4 This study’s findings and the author’s additional experiences confirm that Alcian blue periodic acidic Schiff (ABDPAS) staining is essential for mucin assessment in EUS-FNAB tissue/cell block preparations. Assessment of H&E sections may hint at the presence of free-floating mucin but ABDPAS staining: (i) helps identify mucin at low power examination (figure 9B); (ii) confirms that it is mucin (with a ‘soft’, wispy rather than granular or hard edged appearance) and (iii) indicates the mucin subtype (neutral or acidic or mixed; see below) (figure 9B,C). Some worry that blood contamination during the aspiration will compromise an EUS-FNAB specimen for mucin assessment, and some cytological preparation techniques routinely remove blood. However, if anything, blood contamination aids mucin assessment because gaps between red blood cells quickly point out at low power where mucin may be present (figure 9A,B).

(A) The gaps (arrowed) left between the red blood cells indicate where mucin may be present. (B) This impression was confirmed by ABDPAS staining which showed neutral mucin; the wispy nature of thinner mucin is demonstrated in this panel. (C) ABDPAS staining of this transduodenal EUS-FNAB sample revealed free-floating neutral (top right location in the panel) and acidic (left and central locations in the panel) mucins. The neutral mucin and the foveolar epithelium (*) are regarded to have originated from an MCL, whereas the intestinal epithelium (arrowed) is more likely to be contaminating duodenal mucosa. The free-floating acidic mucin could either have come from the MCL or duodenal mucosa. ABDPAS, Alcian blue periodic acidic Schiff; EUS-FNAB, endoscopic ultrasound-guided fine-needle aspiration biopsy; MCL, mucinous cystic lesion.
It is well recognised that aspirates from pancreatic cystic lesions often show low cellularity.3 The author is unaware of any published study of EUS-FNAB specimens that has formally compared tissue/cell block preparation with cytological preparations for demonstrating cellular material from MCLs. However, if observational studies of sampling and diagnosing pancreatic masses show tissue/cell block preparation is more sensitive than direct smears and LBC techniques,1 tissue/cell blocks are expected to also be superior for demonstrating cellular material from MCLs. In addition, assessing the H&E-stained sections produced by tissue/cell block preparation is more familiar to a wider range of pathologists with regard to diagnosing and grading dysplasia (figure 3A,B). This is because the histopathological (rather than cytopathological) criteria for diagnosing and grading pancreatic dysplasia would be identical to those already well established for biopsies and resection specimens.19 Diagnosing dysplasia would effectively confirm a diagnosis of MCL, and the presence of high-grade dysplasia is now regarded as an absolute indication for surgical resection of IPMN.3
The author is also unaware of any published data on the diagnostic significance of ‘mismatched mucin’ in EUS-FNAB specimens from pancreatic cystic lesions. ‘Mismatched free-floating mucin’ is defined as the presence of acidic mucin in a transgastric FNAB or the presence of neutral mucin in a transduodenal FNAB (figure 9C). The author regards both scenarios to increase the likelihood that mucin in an EUS-FNAB specimen indicates origin from an MCL; this is even more so for transgastric samples because transduodenal aspiration could potentially sample the neutral mucin of Brunner’s glands (table 1). Conversely, the author will always raise the possibility that free-floating neutral mucin in a transgastric aspirate and free-floating acidic mucin in a transduodenal aspirate represent mucosal contaminant rather than the contents of an MCL (table 1 and figure 9C). ‘Mismatched epithelial mucin’ is defined as the presence of acidic mucin in foveolar-like epithelium (figure 3C,D) (or theoretically neutral mucin in intestinal-like epithelium though the author has not yet observed this) and is regarded anecdotally to diagnose MCL with high specificity. ‘Mismatched mucin’, whether free floating or epithelial, will always be less sensitive for diagnosing MCLs than the presence of mucin per se because a MCL may produce the same mucin subtype as the mucosa through which it is sampled, and a MCL may just be lined by foveolar epithelium containing neutral rather than acidic mucin. However, it is very difficult to calculate the exact specificities of ‘mismatched free-floating mucin’ or ‘mismatched epithelial mucin’ for diagnosing MCLs. These values cannot be determined using EUS-FNAB specimens from resected pancreatic cysts alone because, by the fact resection occurred, most would be MCLs and there would be vast under-representation of other cystic lesions, for example, pseudocyst and SCA. These values also cannot be determined with certainty using EUS-FNAB specimens from unresected pancreatic cysts because their diagnoses would have been based only on a combination of radiological, biochemical and even EUS-FNAB findings, and these cannot replace a gold standard, resected tissue diagnosis. Therefore, while there is biological logic to why ‘mismatched mucin’ patterns should increase specificity for diagnosing MCLs, the author accepts that this remains anecdotal.
Proposed interpretations of each combination of different free-floating mucin subtypes according to the route of EUS-FNAB
Equipment are now available for taking micro-biopsies of pancreatic cyst walls. The author has thus seen a handful of MCL wall biopsies which contained ovarian type stroma that could be confirmed with oestrogen receptor, PR and desmin immunohistochemistry (figure 10A–C) and therefore used to diagnose MCN.

(A–C) Microforcep biopsy, taken via EUS, of a pancreatic mucinous cystic neoplasm (as was confirmed histologically when the neoplasm was surgically resected). The epithelium was (A) attenuated but showed (B) apical mucin vacuoles, containing only acidic mucin in this panel. The underlying stroma was (A) more cellular and showed (C) focal oestrogen receptor positivity (examples arrowed). (D) This first time, transduodenal EUS-FNAB sample from a pancreatic cystic lesion showed blood, scattered macrophages (arrowed) and abundant acellular pink debris which resembled necrotic material found in pseudocysts (see figure 11) but was mainly fibrin—as was proven by MSB staining (inset, also showing yellow erythrocytes). (E) ABDPAS showed abundant free-floating neutral mucin which favoured a diagnosis of MCL which was presumed to have previously bled into itself. ABDPAS, Alcian blue periodic acidic Schiff; EUS-FNAB, endoscopic ultrasound-guided fine-needle aspiration biopsy; MCL, mucinous cystic lesion.

Sampling of two different pseudocysts. (A) The more cellular specimen shows acute inflammation, with scattered microcalcification (arrowed) and acellular pink material which focally resembles necrotic fat (*). (B) The less cellular specimen still shows similar acellular pink material but also more prominent haematoidin and both free-floating macrophages and multinucleated giant cells (inset).
On a final note about MCLs, previous sampling or even spontaneous bleeding20 can cause stripping of the glandular lining and filling of the lumen with blood. The resulting EUS-FNAB specimen can therefore contain macrophages, acellular debris, haematoidin and/or inflammatory cells and can potentially be misdiagnosed as pseudocyst contents especially if a mucin stain is not performed (figure 10D,E).
Serous cystadenoma
The author’s experience that SCAs consistently yield hypocellular EUS-FNAB specimens has also been reported elsewhere.21 Indeed, this contrast with the usually hypercellular specimens from NET is a first way to exclude what the author feels is the closest, most common morphological mimic of SCA. The cytological features of SCA (see above) and the usual presence of only scattered small cell clusters within blood means that they can be mistaken for lymphocytes at low power (figure 7A). Because inhibin is a highly sensitive marker of SCA,22 23 this immunomarker is an invaluable tool for highlighting sparse cells when not obvious in H&E sections (figure 7B). More cellular specimens from SCA can include fibrous stroma fragments which are lined by and/or contain the neoplastic cells. The following may or may not be a consequence of tissue/cell block preparation but the author has found SCA cells in these preparations to only uncommonly show clear cytoplasm and/or cytoplasmic glycogen (assessed using PAS staining +/−diastase treatment) (figure 7C). While inhibin positivity can be used to support a diagnosis of SCA, its specificity is not absolute especially in that it is expressed by a small proportion of NETs.23 24 Therefore, the author is currently analysing a panel of immunomarkers, including inhibin and other proposed biomarkers of SCA,22 23 among a large cohort of EUS-FNAB specimens from SCAs and NETs.
Pseudocyst
The typical aspirated contents of pseudocyst include bile-like pigment, haematoidin and/or inflammatory cells, including siderophages, multinucleated giant cells and neutrophils (figure 11A,B). The author has also seen pink, anucleated material which can resemble necrotic fat, microcalcification (figure 11A,B) and less commonly, cholesterol clefts within inflamed stroma.
Lymphoepithelial cyst
The first clues to the diagnosis of lymphoepithelial cyst (LEC) are the peripancreatic rather than intrapancreatic location of the cyst, a location close to the spleen and the aspiration of turbid (rather than serous or mucoid) fluid from the cyst. A rare drawback of tissue/cell block preparation is that it does not demonstrate the characteristic square/rhomboid crystals which are seen in air-dried smears of LEC contents. However, this is more than compensated for by the facility to apply squamous immunomarkers to EUS-FNAB material (figure 12B). The squamous material of LEC can be distinguished from contaminant squames (presumably from the oesophagus) because only the former includes acellular and/or laminated keratin and dyskeratotic cells (figure 12A). If microbiopsies of the cyst wall are received, these will usually show dense lymphoid stroma (figure 12C).
EUS-FNAB samples of lymphoepithelial cysts. More cellular specimens may include intact strips of squamous epithelium. (A) Laminated keratin and (B) dyskeratotic cells (examples arrowed in the left side of the panel) can be seen in less cellular specimens, and the latter cells can be confirmed with CK5/6 immunohistochemistry (right side of the panel). Microbiopsies (panel C) may show the characteristic lymphoid stroma directly beneath the squamous epithelium. EUS-FNAB, endoscopic ultrasound-guided fine-needle aspiration biopsy.
Other cystic lesions
Other cystic lesions in or around the pancreas that the author has received EUS-FNAB specimens from include: lymphocoele (concentrated lymphocytes, figure 13A,B); and ciliated foregut cyst (ciliated epithelium showing TTF1 positivity, figure 13C).

(A) Aspirate of a lymphocoele showing concentrated lymphocytes which are predominantly, but not all, T cells as confirmed with (B) CD3 positivity. (A) The scattered larger cells (examples arrowed) are macrophages. (C) Fragment of the wall of a ciliated foregut cyst showing respiratory-type epithelium with clear cilia.
Non-lesional pathologies
The author is occasionally asked to assess for autoimmune pancreatitis in non-lesional EUS-FNAB samples. Some of these specimens showed pancreatitic changes with increased numbers of IgG4 positive cells and fibrosis (figure 14A,B) though phlebitis has not yet been seen. If there are more than 10 IgG4-positive plasma cells per high powered field, the author will then request IgG immunohistochemistry to determine the IgG4:IgG ratio. If the acinar tissue sampled is not inflamed or there are no obvious plasma cells in stromal fragments, IgG4 immunohistochemistry is not requested by the author.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tissue sampling of a case of autoimmune pancreatitis which was associated with elevated blood IgG4 levels and the typical ‘sausage-shaped’ radiological appearance of the pancreas. (A) There was widespread atrophy of acinar tissue (a few residual foci are arrowed) with fibrosis and chronic inflammation. The latter included (B) IgG4-positive plasma cells which focally numbered more than 10 per high-powered field. (B) At least six such cells are present in the panel which also shows residual acinar cells as well as positivity of background stroma that the author has occasionally seen with grossly elevated blood IgG4 levels.
Conclusions
There are numerous advantages to using tissue/cell block preparation for EUS-FNAB specimens from pancreatic lesions (box 1). This article has shown how such processing enables the diagnosis of a complete spectrum of pancreatic pathologies that may be sampled this way. One reason for this is how tissue/cell block preparation concentrates and conserves sampled material which is then available for a full range of histochemical, immunohistochemical and genetic analyses. Tissue/cell block preparation also enables EUS-FNAB specimens to be assessed by a wider range of cellular pathologists. The tissue/cell block protocol outlined in this article is simple for EUS-FNAB specimen collection, processing and assessment and is the same regardless of the nature (ie, solid or cystic) or location of the targeted lesion within the GI tract, including the pancreas. The mandatory submission of an EUS report with its EUS-FNAB specimen provides clinical information which may be crucial to interpreting the microscopic findings.
Take home messages
Tissue/cell block preparation is an optimal method for processing EUS-FNAB specimens from the pancreas, and permits the diagnosis of a full range of pathologies sampled this way.
The same tissue/cell block protocol can be used regardless of the site and nature (e.g. cystic versus solid) of the lesion sampled.
This tissue/cell block protocol is simple from collection to processing to assessment, and it permits assessment by a wider range of cellular pathologists.
Acknowledgments
The author thanks Drs Sophie Beavers, Tim Bracey and Jemima Denson for their comments on this manuscript.
References
Footnotes
Handling editor Runjan Chetty.
Contributors NACSW wrote the entire manuscript.
Funding The author has not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.