Article Text

Abstract
Aims Accurate and reliable diagnosis is essential for lung cancer treatment. The study aim was to investigate interpathologist diagnostic concordance for pulmonary tumours according to WHO diagnostic criteria.
Methods Fifty-two unselected lung and bronchial biopsies were diagnosed by a thoracic pathologist based on a broad spectrum of immunohistochemical (IHC) stainings, molecular data and clinical/radiological information. Slides stained with H&E, thyroid transcription factor-1 (TTF-1) clone SPT24 and p40 were scanned and provided digitally to 20 pathologists unaware of reference diagnoses. The pathologists independently diagnosed the cases and stated if further diagnostic markers were deemed necessary.
Results In 31 (60%) of the cases, ≥80% of the pathologists agreed with each other and with the reference diagnosis. Lower agreement was seen in non-small cell neuroendocrine tumours and in squamous cell carcinoma with diffuse TTF-1 positivity. Agreement with the reference diagnosis ranged from 26 to 45 (50%–87%) for the individual pathologists. The pathologists requested additional IHC staining in 15–44 (29%–85%) of the 52 cases. In nearly half (17 of 36) of the malignant cases, one or more pathologist advocated for a different final diagnosis than the reference without need of additional IHC markers, potentially leading to different clinical treatment.
Conclusions Interpathologist diagnostic agreement is moderate for small unselected bronchial and lung biopsies based on a minimal panel of markers. Neuroendocrine morphology is sometimes missed and TTF-1 clone SPT24 should be interpreted with caution. Our results suggest an intensified education need for thoracic pathologists and a more generous use of diagnostic IHC markers.
- lung neoplasms
- diagnosis
- immunohistochemistry
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Evaluation of pulmonary tumours by surgical pathologists is central in the clinical diagnostic process to confirm a malignant disease, determine the histological type, suggest the site of origin and finally to propose further molecular analyses. All these aspects are essential for treatment selection, which stresses the demand for accurate and reliable diagnosis.
Adenocarcinoma (AC), squamous cell carcinoma (SqCC) and small cell lung carcinoma (SCLC) are the most common primary lung cancers.1 Metastases to the lungs of various origins and types, although commonly AC,2 3 are also prevalent. Samples from the lungs are typically small specimens, where immunohistochemical (IHC) staining is often necessary to complement morphology for diagnosis. Ideally, histological type should be determined, and a non-pulmonary origin (if suspected from morphology, radiological/clinical findings or patient history) should be confirmed or ruled out. At the same time, limited panels of diagnostic IHC stainings are preferred as a considerable amount of tumour material is often needed for predictive IHC and molecular analyses.4
Lung tumours should be diagnosed in accordance with the WHO guidelines.5 6 According to these guidelines, there is no need for IHC staining in morphologically obvious SqCC or (non-mucinous) AC. For non-small cell carcinoma (NSCC) without clear squamous or glandular differentiation, one IHC marker for AC and one for SqCC is recommended, with thyroid transcription factor 1 (TTF-1) and p40, respectively, as first choice. Neuroendocrine (NE) markers should only be performed in cases with NE morphology (other markers may also be appropriate for NE tumours, eg, cytokeratins (CK) and Ki67). Additional IHC staining is also performed if both TTF-1 and p40 are negative, if a non-pulmonary origin is suspected and to confirm rare tumour types including non-epithelial malignancies. In Sweden, these guidelines have generally been adopted, but with the exception that TTF-1 is recommended also in morphologically obvious AC (including non-mucinous) to support origin in the lungs.
The WHO group recommends TTF-1 clone 8G7G3/1,6 which is a less sensitive but more specific marker compared with, for example, clone SPT24.3 7 NordiQC (www.nordiqc.org), contracted for external technical quality assurance of IHC staining by >200 pathology departments including Sweden, on the other hand recommends a more sensitive protocol with, for example, clone SPT24.8 Accordingly, most pathology departments in Sweden use TTF-1 clone SPT24, and while it is known that more SqCC,3 7 9 10 metastases to the lungs3 11 12 and non-epithelial tumours13 14 are positive with this clone, there is a lack of data on how often this results in incorrect diagnoses in the clinical setting.
The aim of the present study was to evaluate interpathologist diagnostic concordance in unselected bronchial and lung biopsies from suspected malignant tumours in relation to current diagnostic guidelines and standard practice. For each case, sections stained with H&E, p40 and TTF-1 clone SPT24 were scanned, and the involved pathologists were to state the most likely diagnosis and if additional diagnostic IHC staining was regarded to be necessary.
Material & Methods
Cases
In total, 52 bronchial forceps and transthoracic lung core biopsies that were part of investigation of a suspected malignant disease were included in the study. Cases were selected to represent the diagnostic work routine in Sweden. The basis for this was consecutive cases diagnosed at the Department of Genetics and Pathology, Lund, Sweden, by the principal investigator (HB) in June to August and December 2019. Biopsies with limited or only completely normal tissue were excluded. Cases were replaced with matched ones from the pathology archives if p40 and TTF-1 clone SPT24 (if not already performed) could not be stained without risking tissue for predictive analyses or other diagnostic markers of need. Also, cases with suboptimal scanning quality were, if still suboptimal after re-scanning, replaced with archival cases. Furthermore, some bronchial biopsies were replaced with archival lung biopsies as bronchial biopsies are more frequent in Lund compared with other sites in Sweden. In total, 16 of the 52 cases were matched cases from the archives, all with the same diagnosis as the ones they replaced in order to reduce selection bias.
All cases were stained for p40 (clone BC28; Histolab/Biocare Medical, Concord, California, USA) and TTF-1 (clone SPT24; Leica Biosystems, Nussloch, Germany) using a Ventana Benchmark Ultra (Ventana Medical Systems, Tucson, Arizona, USA) as clinical samples at the Department of Genetics and Pathology, Lund, Sweden. Control tissue was used on each slide and was also included in the scanned image. The H&E and IHC slides were scanned using an Aperio ScanScope AT Digital Pathology Slide Scanner (Leica Biosystems) at 40× magnification and saved as svs-files. Aperio ImageScope (Leica Biosystems) was suggested as viewer to the participating pathologists, but any viewer was allowed and for example, QuPath (University of Edinburgh) was used by at least one pathologist.
In the clinical setting, the cases were diagnosed using a microscope, but the scanned images were also reviewed. Additional IHC markers, ancillary conventional stains and level sectioning was performed when necessary and used as basis for the reference diagnosis. For all cases, clinical and radiological information was available in the clinical setting. Consultation of colleagues was possible (the consulted pathologists then unaware that the cases were included in the study), and for more than half of the cases concurrent cytological samples were also available. The reference diagnosis did not rely on follow-up information, but such information (including follow-up samples) was reviewed as part of the study.
Pathologists
Board-certified surgical pathology consultants diagnosing at least one lung cancer case per year were invited to participate. Pathologists in Sweden and abroad that were known by the principal investigator (HB) were contacted, but the invited pathologists were also encouraged to invite others, and in total half of the pathology departments in Sweden were contacted. The pathologists who accepted participation and completed the assignment are all coauthors of the study (ie, all authors except HB and CC).
Instructions
For each case, the pathologists were instructed to individually state which diagnosis was the most probable from those listed in box 1. No other diagnostic categories than those given were possible, but the pathologists could add comments. Also, the pathologists were to state if they would have ordered additional diagnostic IHC markers before the final diagnosis in the clinical setting (yes/no). Information on age, gender and previous malignancy was available for each case, and that the biopsy was taken to confirm/rule out malignancy, but no other clinical/radiological information. The pathologists were allowed to use literature, as in the clinical diagnostic situation, but were not allowed to consult colleagues.
Selectable diagnoses in the present study.
Adenocarcinoma/non-small cell carcinoma favour adenocarcinoma.
Squamous cell carcinoma/non-small cell carcinoma favour squamous cell carcinoma.
Small cell lung carcinoma*
Non-small cell carcinoma probably large cell neuroendocrine carcinoma*
Carcinoid tumour
Non-small cell carcinoma, other specified type (adenosquamous carcinoma, sarcomatoid carcinoma, salivary gland type carcinoma and so on)
Non-small cell carcinoma not otherwise specified
Non-epithelial primary malignancy
Metastasis to the lung (regardless of type or origin)
Suspicion of malignancy
Atypia of undetermined significance
Benign tumour, normal tissue or non-neoplastic disease
Also, there were general questions for each pathologist: number of years as consultant (<5/5–14/≥15 years), number of lung cancer cases signed out per year (1–49/≥50 cases), experience in diagnosing scanned cases (yes/no), experience in TTF-1 clones (SPT24/8G7 G3/1/both/other/not known) and the time it took to diagnose the cases rounded to the closest half-hour.
See the online supplemental material for the full instructions and template for the participating pathologists (English versions). As evident, no specific hypotheses were mentioned in the instructions.
Supplemental material
Statistics
Multivariable regression analysis was used for correlation between the pathologists’ number of cases in agreement with the reference diagnosis and number of cases for which additional IHC would be ordered, respectively, with years as consultant (<5/5–14/≥15 years), number of lung cancer cases signed out per year (1–49/≥50 cases), experience in diagnosing scanned cases (yes/no), TTF-1 clone experience (8G7G3/1/SPT24/both) and time for diagnosing the cases (<4/≥4 hours). A p value of <0.05 was considered statistically significant. The analyses were performed with MedCalc V.14.12.0 (MedCalc Software, Ostend, Belgium).
Results
Participating pathologists
The participants consisted of 20 board-certified pathologists. Of these, six had been consultants for <5 years, five for 5–14 years and nine for ≥15 years. Five and 15 of the pathologists signed out 1–49 and ≥50 lung cancer cases, respectively, a normal year. Exactly half reported to have experience in diagnosing scanned cases. One pathologist had experience of TTF-1 clone 8G7G3/1, 12 of clone SPT24 and 7 of both clones. The median time it took to diagnose the cases was 3.5 hours (range 2–6.5 hour).
Cases
The 52 cases consisted of 29 bronchial forceps biopsies and 23 transthoracic core biopsies from 27 women and 25 men who had a median age of 71 years (range 32–88 years). There was a known previous malignancy in 23 of the cases, whereof 4 had two previous malignancies. The tumours were breast cancer (n=6), prostatic cancer (n=6), lung cancer (n=5), colorectal cancer (n=2), kidney cancer (n=2), urinary bladder cancer (n=1), endometrial cancer (n=1), bile duct cancer (n=1), melanoma (n=1), skin SqCC (n=1) and chronic lymphocytic leukaemia (n=1; untreated).
The reference diagnosis (thus used for treatment decision) was lung AC in 13 cases, benign/non-neoplastic lesion in 13, metastasis from another organ in 7, SqCC in 6, SCLC in 5 (whereof one mixed SCLC/large cell NE carcinoma (LCNEC)), NSCC probably LCNEC in 2, carcinoid tumour (CT) in 2, suspicion of malignancy in 2 (follow-up sampling confirmed malignancy in one of the cases) and unclear atypia in 1 case. There was also one case that was unclear if lung NSCC not otherwise specified (NOS) or recurrent breast cancer despite comprehensive IHC staining and molecular analysis. The reference diagnosis is marked for each case in table 1. The metastases were breast cancer (n=2), colorectal cancer (n=2), kidney cancer (n=1), bile duct cancer (n=1) and melanoma (n=1). The benign/non-neoplastic lesions included mild-to-moderate inflammation (n=5) whereof two with necrosis, organising pneumonia (n=3) whereof one with focal necrosis, reactive pneumocytes (n=2), hamartoma (n=1), granulomatous inflammation (n=1) and macrophages and anthracosis (n=1).
Suggested diagnosis and if additional diagnostic IHC staining would be ordered by 20 pathologists for 52 unselected bronchial and lung biopsies based on H&E, p40 and TTF-1 (clone SPT24) staining (the reference diagnosis, and if additional IHC staining was performed and used for diagnostics, is marked in grey)
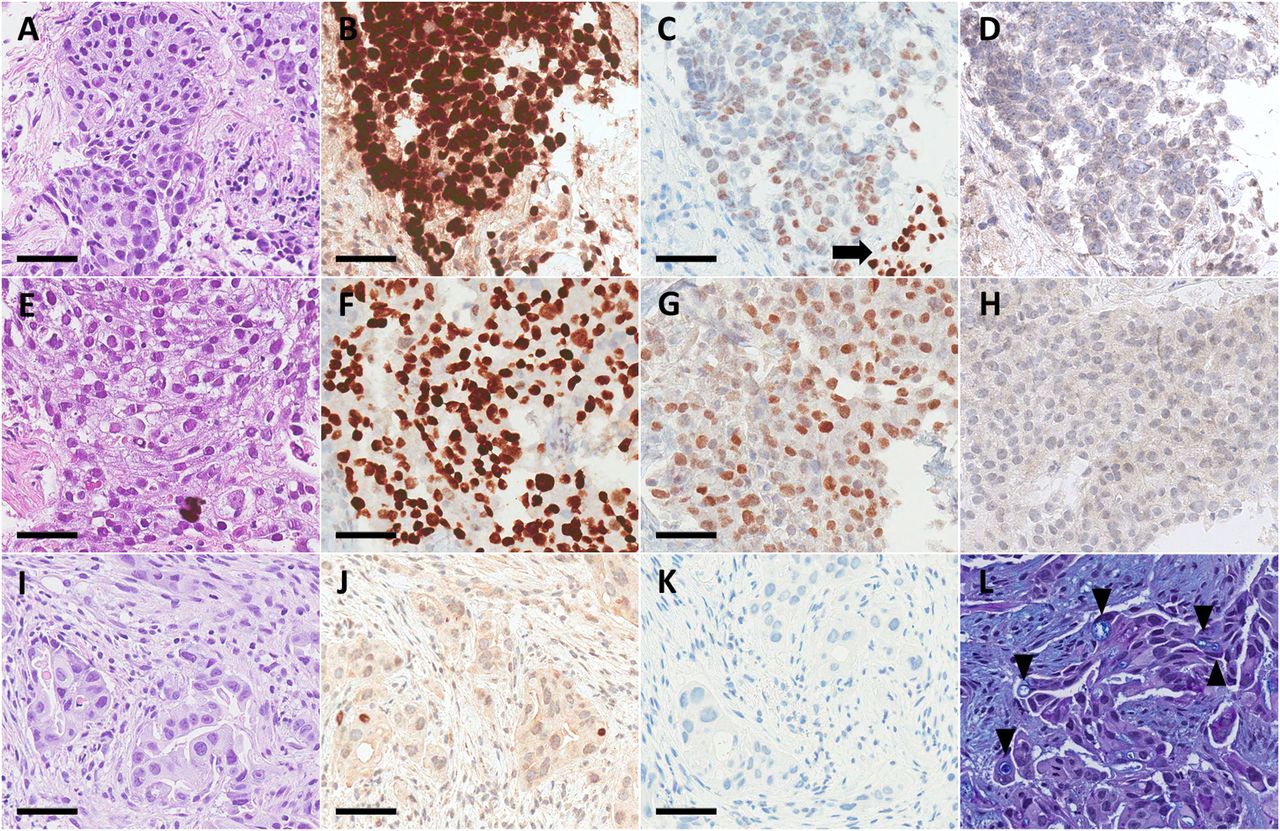
TTF-1 was strongly positive in >95% of the tumour cells in 11 of the 13 AC, 4 of 5 SCLC, both of CT and one of the two NSCC probably LCNEC, while no positivity was seen in the remaining 4 AC/SCLC/LCNEC. All metastases from other organs were completely negative for TTF-1, while weak positivity was seen in five of the six SqCC, with a range of 1%–95% positive tumour cells. See figure 1 for the two cases with >20% TTF-1 positivity. P40 was strongly positive in >95% of the tumour cells in all the six SqCC, and the only other cases with positive p40 cells were one TTF-1-negative AC (see figure 1) and one SCLC (with partial features of LCNEC) with <1% and 1%–2% positive tumour cells, respectively.

Two cases of squamous cell carcinoma (A–D, case 1 and E–H, case 45 in table 1) with diffuse positivity for TTF-1 clone SPT24 (G represents the strongest TTF-1 positivity in squamous cell carcinoma in the study), and one case of adenocarcinoma negative for TTF-1 but with some (<1%) cells positive for p40 (I–L, case 7 in table 1). Staining with H&E (A, E, I), p40 (B, F, J) and TTF-1 clone SPT24 (C, G, K). Note that included here, but not available to the participating pathologists, are TTF-1 clone 8G7G3/1 (D, H) and alcian blue-periodic acid-Schiff (L; arrow heads mark intracellular inclusions). Benign epithelium with stronger TTF-1 positivity is marked with arrow (C). Scale bar is 50 μm.
For reference diagnosis, but not available to the participating pathologists in this study, further IHC markers (in addition to p40 and TTF-1) were used to determine the diagnosis in 34 of the 52 cases. These cases are marked in table 1.
Concordance
As evident from table 1, there was perfect agreement among the participating pathologists on most probable diagnosis in 7 (13%) of the 52 cases (for case 52, both NSCC NOS and metastasis to the lungs was considered to be in agreement since the exact diagnosis could not be established). At least 80% (≥16) of the pathologists agreed with each other and the reference diagnosis in 31 (60%) of the cases. In two other cases, there was also high (≥80%) agreement between the participating pathologists but not with the reference diagnosis. One case (case 23) was judged to be AC by most pathologists while the reference diagnosis was NSCC probably LCNEC, with LCNEC confirmed on follow-up resection. The other case (case 40) was considered to be AC by most pathologists while the reference diagnosis was suspicion of malignancy after IHC staining and level sectioning. AC was confirmed on follow-up biopsy.
The agreement with the reference diagnosis ranged from 26 to 45 (50%–87%) of the 52 cases (mean and median 37 cases) for the individual pathologists.
There was a high agreement (≥80% of pathologists) among the pathologists for 9 of the 13 cases with AC as reference diagnosis. For both the two TTF-1negative AC (cases 7 and 8), the diagnostic concordance was low (<80%). The other two AC cases with low concordance values were poorly differentiated with either focal sarcomatoid features (case 34) or limited small groups and isolated malignant cells (case 43). In 6 of the 11 TTF-1-positive AC cases, 1–6 pathologists had NSCC NOS as most probable diagnosis.
Likewise, there was high agreement (≥80%) for five of the six SqCC cases. The case with low concordance (case 45), with only 55% of the pathologist stating SqCC as most probable diagnosis, expressed weak TTF-1 in 95% of the cells. See figure 1E–H.
For NE tumours, there was high agreement (≥80%) for five of the nine NE tumours. Seven pathologists commented that a NE tumour was considered, but not selected as most probable diagnosis, in one to two of these cases (information not specifically asked for in the study). See figure 2 for example of NE cases.

{kind=link}
{kind=link}
Two cases of carcinoid tumour (A, B, case 48 in table 1) and large cell neuroendocrine carcinoma (C, D, case 23 in table 1), respectively, where a limited number of pathologists suggested these diagnoses. Focal necrosis was seen in the large cell neuroendocrine carcinoma (not shown). Staining with H&E. For both cases, the diagnosis was confirmed on follow-up resection. Scale bar is 50 μm.
Although no other markers than p40 and TTF-1 were provided in the study, there was ≥80% agreement for five of the seven metastases to the lungs.
In multivariable analysis, there was no significant correlation between number of cases in agreement with the reference diagnosis and years as consultant, number of lung cancer cases signed out per year, experience in diagnosing scanned cases, TTF-1 clone experience or time for diagnosing the cases (p=0.071–0.41).
Additional IHC staining
The participating pathologists requested additional IHC stainings to confirm the suggested diagnosis in 15–44 (29%–85%) of the 52 cases (mean 29 and median 28 cases) based on 19 pathologists (no data for 1 pathologist).
In 5 of the 13 AC cases, 1–3 of the pathologists did not suggest AC as most probable diagnosis and at the same time did not request for additional IHC stainings. In all these cases, the suggested diagnosis was NSCC NOS or suspicion of malignancy. All but two pathologists suggested additional IHC stainings in 1–9 (median 4) of the 11 TTF-1-positive AC cases.
Correspondingly, in four of the six SqCC cases, one to two pathologists did not suggest SqCC as most probable diagnosis while not requesting for additional IHC markers. NSCC NOS or suspicion of malignancy was suggested diagnosis in all these cases.
In 6 of the 9 NE tumours, 1–11 of the pathologists did not suggest the same diagnosis as the reference while not requesting additional IHC markers. Most notable was one NSCC probably LCNEC (case 23) and one CT 5 (case 48) where 11 and 5 pathologists, respectively, suggested AC or NSCC NOS with no additional IHC markers.
In two of the seven metastases to the lungs, one pathologist that did not have metastasis as most probable diagnosis stated that more IHC markers would not have been ordered.
In multivariable analysis, there was no significant correlation between number of cases for which additional IHC would be ordered and years as consultant, number of lung cancer cases signed out per year, experience in diagnosing scanned cases, TTF-1 clone experience or time for diagnosing the cases (p=0.30–0.81).
Discussion
This study evaluates the diagnostic decision-making of pathologists in a standardised and systematic but also realistic fashion. It illustrates the difficulties in diagnosing small biopsies and the correct use of IHC markers.
Studies on various specimen types have shown that addition of IHC staining increases interpathologist diagnostic concordance in lung NSCC.15–17 With a limited panel of p40 and TTF-1, for assessment of current guidelines for NSCC with unclear morphology, we here demonstrate a moderate concordance for unselected lung/bronchial biopsies. In our study, cases with limited agreement among pathologists were in particular NE tumours that did not exhibit classic small cell morphology. This has clinical implications, as unresectable pulmonary NE tumours are typically treated differently than NSCC. According to diagnostic guidelines by the WHO group,5 6 IHC staining with NE markers should only be performed in cases with NE morphology. This may be advisable as IHC expression of NE markers is seen in a significant number of AC and SqCC.18 Still, the question is if routine IHC staining with an NE marker in addition to p40 and TTF-1 would increase recognition of NE tumours without significant overdiagnostics of NE tumours.
Compared with TTF-1 clone 8G7G3/1, clone SPT24 stains more metastases to the lungs, for example, colorectal and urothelial metastases,3 11 12 which pathologists need to be aware of. Expression of TTF-1 in SqCC with clone SPT243 7 9 10 19 may also be problematic, at least in cases with substantial TTF-1 positivity, as clearly evident in the present study. None of our TTF-1-positive SqCC cases expressed napsin A or TTF-1 clone 8G7G3/1 (markers not available to the participating pathologists). The very low frequency of TTF-1 positivity in SqCC with clone 8G7G3/13 7 9 10 20 support that this clone indicates adenocarcinomatous differentiation (in the absence of NE morphology). The WHO guidelines recognize that also focal positivity (<10%) counts for TTF-1 clone 8G7G3/1 and that the marker trumps p40 if both are positive in the same cells.5 6 However, as TTF-1 clone SPT24 is frequently used, there is a need for additional recommendations for TTF-1 positivity with regard to the used clone. We suggest diagnostic guidelines for a sensitive TTF-1 clone in table 2. Still, although not specifically investigated in the present study, our data support that 8G7G3/1 should be the preferred TTF-1 clone.
Suggested algorithm for pulmonary non-small cell carcinoma without clear morphology when TTF-1 clone SPT24 is used
From the present study, we may conclude that there is great variability in how often pathologists use IHC in pulmonary biopsies. Several studies have demonstrated the value of IHC for subtyping poorly differentiated lung cancers.21–24 However, in our study additional IHC staining was requested in a subset of TTF-1-positive (and morphologically obvious) AC cases by almost all participating pathologists. This is not in line with international guidelines but may reflect the pathologists’ awareness of TTF-1 positivity (with clone SPT24) in metastases to the lungs or NE tumours. Although a 5-marker panel (including mucin stain) did not affect testing for EGFR with PCR in a study on small specimens,17 any additional IHC should be carefully considered given the use of material as well as time and cost.
It may be noted that most AC cases (all exhibiting glandular formations and/or expression of TTF-1) were categorised as NSCC NOS by some pathologists, which is not in line with the current terminology.5 This may reflect lack of knowledge of the current classification, but perhaps more likely lack of adherence to the terminology (as AC and NSCC NOS are typically treated identically). Thus, it could be argued that these categories should be merged, resulting in a higher interpathologist agreement. The same may apply to NSCC with sarcomatoid features, at least if positive for TTF-1, as in one of our cases.
The aim of our study was not primarily diagnostic accuracy, and such a study would need to include additional IHC markers of relevance (eg, NE markers and various IHC stainings for non-pulmonary origin, also for the TTF-1-negative AC cases). However, inclusion of additional IHC markers for some cases would risk guiding the participating pathologists, while including a broad panel of stains for all cases would not resemble the routine diagnostic situation. Instead, the study focused on evaluating the IHC panel recommended for NSCC and recognition of morphological findings that would guide the selection of further IHC stainings.
Also, the focus of the present study was not on differentiation between benign conditions, unclear atypia, suspicion of malignancy and malignant lesions. For this area, scanning quality, access to level sections and experience in digital pathology probably have a greater impact on diagnostic concordance, and we choose not to draw any strong conclusions from our results. Still, a malignant diagnosis was suggested in cases with organising pneumonia by some pathologists, why we plan to address the topic in future quality assurance work.
Relating to this topic, for one case (case 40 in table 1) the reference diagnosis was suspicion of malignancy based on additional level sectioning and consultation of a colleague. A follow-up sample confirmed AC and most likely the atypical cells in the study sample represent the tumour. That cases are presented as in the diagnostic situation and not based on follow-up sampling may affect concordance with reference diagnosis but not interpathologist concordance (which was our main focus). However, basing the reference diagnosis on follow-up samples would be problematic for other cases (eg, cases 3 and 24).
In conclusion, our study presents a real-world evaluation of practice and reliability of lung tumour diagnostics. It supports previous notions that the addition of IHC markers aid pathologists in the diagnostic process, but in particular highlights difficulties in correct interpretation of markers (especially TTF-1 clone SPT24). The moderate diagnostic concordance, inaccurate diagnoses in some cases (especially NE tumours) and the underuse and overuse of IHC stainings stress the need for further standardisation, continuous education of pathologists and interpathologist consultations.
Take home messages
Based on slides stained with H&E, thyroid transcription factor-1 (TTF-1) clone SPT24 and p40 for 52 lung/bronchial biopsies, there was a moderate interpathologist diagnostic concordance for 20 surgical pathologists.
Diagnostic difficulties include detection of neuroendocrine morphology and TTF-1 positivity in squamous cell carcinomas.
Supplemental material
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted in adherence with the Declaration of Helsinki and approved by the regional ethical review board in Lund (Dnr 2020-00256).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Runjan Chetty.
Contributors Conceptualisation, data curation and analysis: HB. Project administration and technical resources: CC and HB. Data collection: KEL, SW-F, IG, AE, NM, RU, ML, FS, TS, FH, KD, MB, EB, AS, MW, MR, LEDLC, MG, AH, PM. Writing the manuscript: HB. Reviewing and editing: KEL, CC, SW-F, IG, AE, NM, RU, ML, FS, TS, FH, KD, MB, EB, AS, MW, MR, LEDLC, MG, AH, PM.
Funding The study was supported by the Regional Agreement on Medical Training and Clinical Research (ALF) and the Swedish Cancer Society.
Disclaimer The funding sources were not involved in study design, data collection or analysis or writing the report.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.