Article Text

Abstract
Aims Primary lung adenocarcinoma consists of a spectrum of clinical and pathological subtypes that may impact on overall survival (OS). Our study aims to evaluate the impact of adenocarcinoma subtype and intra-alveolar spread on survival after anatomical lung resection and identify different prognostic factors based on stage and histological subtype.
Methods Newly diagnosed patients undergoing anatomical lung resections without induction therapy, for pT1-3, N0-2 lung adenocarcinoma from April 2011 to March 2013, were included. The effect of clinical–pathological factors on survival was retrospectively assessed.
Results Two hundred and sixty-two patients were enrolled. The 1-year, 3-year and 5-year OS were 88.8%, 64.3% and 51.1%, respectively. Univariate analysis showed lymphovascular, parietal pleural and chest wall invasion to confer a worse 1-year and 5-year prognosis (all p<0.0001). Solid predominant adenocarcinomas exhibited a significantly worse OS (p=0.014). Multivariate analysis did not identify solid subtype as an independent prognostic factor; however, identified stage >IIa, lymphovascular invasion (p=0.002) and intra-alveolar spread (p=0.009) as significant independent predictors of worse OS. Co-presence of intra-alveolar spread and solid predominance significantly reduced OS. Disease-free survival (DFS) was reduced with parietal pleural (p=0.0007) and chest wall invasion (p<0.0001), however, adenocarcinoma subtype had no significant impact on DFS.
Conclusions Our study demonstrates that solid predominant adenocarcinoma, intra-alveolar spread and lymphovascular invasion confer a worse prognosis and should be used as a prognostic tool to determine appropriate adjuvant treatment.
- lung
- lung neoplasms
- carcinoma
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. The retrospective database including all data collected will be available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Lung cancer is the leading cause of cancer-related mortality worldwide, with adenocarcinoma being the most common histological subtype accounting for 35% of lung cancers.1 Pulmonary adenocarcinoma is heterogeneous in its histological pattern, molecular profile, clinical findings, radiological presentation and treatment options.2
In 2015, a new WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart (fourth edition) was published defining five different histological subtypes: lepidic, acinar, papillary, micropapillary and solid patterns.3 4 This new classification for adenocarcinomas was based on the International Association for the Study of Lung Cancer, American Thoracic Society and European Respiratory Society (IASLC/ATS/ERS) recommendations made in 2011.5 6
Since 2011, several publications have reported a strong correlation between predominant patterns of adenocarcinoma and prognosis, with solid and micropapillary patterns conferring a worse prognosis (reduced overall survival (OS)) and lepidic predominance having a better prognosis.7–9 Despite this, tumour subtype is currently not a criterion used to select patients for adjuvant therapies.10
More recently, tumour intra-alveolar spread has been shown to strongly correlate with lymph node and distant metastases as well as a higher incidence of local recurrence of tumour, hence serving as an independent negative prognostic factor for lung adenocarcinomas.11–13
The main aim of our study is to evaluate the impact of adenocarcinoma subtype and intra-alveolar spread on survival after anatomical lung resection and to identify different prognostic factors based on stage and histological subtypes.
Patients
Patient recruitment
All patients undergoing anatomical lung resection between April 2011 and March 2013 for pT1-3 N0-2 lung adenocarcinoma were included. Exclusion criteria were patients with pT4 tumours, tumour types other than adenocarcinoma (neuroendocrine tumour, small cell lung cancer squamous tumours), incomplete resection and those undergoing induction treatment, chemo and or radiotherapy. Patients who had tumours larger than 40 mm, or N1/N2 disease, received adjuvant chemotherapy. Patients with N2 disease or R1 resections received adjuvant radiotherapy. cN2 single station surgery was indicated.
Data acquisition and analysis
Demographic, clinical and survival data for those patients who fulfilled the inclusion criteria were retrospectively obtained from hospital electronic medical records and serial follow-up information obtained from correspondence letters with primary care physicians.
H&E-stained sections from resected lung adenocarcinomas were reviewed, and according to the 2015 WHO classification of lung tumours,14 histological diagnosis of adenocarcinoma was confirmed and subclassification to lepidic, acinar, papillary, micropapillary and solid type was made. All tumours were documented for tumour size, lymphovascular invasion, visceral or parietal pleural invasion and lymph node metastasis. Tumour stage was based on the Tumour Nodes Metastases (TNM) eighth edition classification.15 In order to derive the percentage contribution of each subtype of adenocarcinoma to the overall tumour, all H&E-stained slides for tumours were digitally scanned using a Hamamatsu Nanozoomer scanner and analysed using proprietary software (Hamamatsu NPD.View2). This tumour area, represented by each histopathological subtype, was defined and expressed as a percentage of the overall tumour. The presence of adenocarcinoma in situ, minimally invasive adenocarcinoma, lepidic, acinar, mucinous, solid and micropapillary components, was reported on percentage. Additionally, the presence of the intra-alveolar spread has then been reported. Spread through air spaces (STAS) was defined as small clusters of tumour cell nests within air spaces in the lung parenchyma beyond the edge of the main tumour. The edge of the main tumour was defined as the outer border of the tumour. STAS was considered present when tumour cells were identified beyond the edge of the main tumour.16
Statistical analysis
Continuous variables were expressed as mean±SD and categorical data expressed as counts and percentages. Univariate analysis was performed using χ2 or unpaired t-tests where appropriate. Survival was measured from the date of surgical intervention and survival data were analysed using Kaplan-Meier methodology. Factors significantly affecting survival in univariate analysis (at p<0.005) were included in a multivariate Cox proportional hazard regression mode. The stepwise backward procedure based on the likelihood ratio was used to assess the significance of covariate included in the model. HRs and 95% CIs were calculated. Statistical significance was defined where p<0.05. All analyses were carried out using STATA V.12.0.
Results
Demographic and clinical patient data
A total of 262 patients, who underwent an anatomical lung resection from February 2011 to March 2013, were included in the analysis. The average age of the study population was 69.7±8.7 years, of whom 45% (118/262) was men. Full demographic details and clinical details are included in table 1.
Baseline characteristics of the study population
Overall survival
All patients were followed up until July 2018. The median OS for the study population was 42.6 months (range 0.4–68.1). The 1-year, 3-year and 5-year survival rate were 88.8%, 64.3% and 51.1%, respectively (figure 1). The 30-day mortality rate was 1.1% (n=3). As expected, there was a stepwise decrease in OS with more advanced pathological stage (figure 2). Stage IB tumours did not demonstrate significantly worse survival than stage IA tumours (p=0.264) (table 2). When compared with stage I disease, stages II and III showed worse OS.

Overall survival. 1 year 88.8% (84.2–92.1); 2 years 73.87% (68.0-78.8); 3 years 64.3% (58.1–69.9); 4 years 58.9% (52.5–64.8); 5 years 51.1% (42.8–58.8).

Survival according to disease stage. Stage II and III tumours showed worse overall survival. Stage IB showed no statistical difference to IA.
Univariate analysis of predictors of overall survival
At univariate analysis, clinicopathological factors conferring a worse prognosis at 1 and 5 years were the presence of lymphovascular invasion (85% vs 91% at 1 year and 39% vs 60% at 5 years; χ2=17.3, p<0.0001), parietal pleural invasion (69% vs 90% at 1 year and 8.6% vs 67% at 3 years; χ2=26.31, p<0.0001), chest wall invasion (40% vs 90% at 1 year; χ2=26.82, p<0.0001), visceral pleural invasion (84% vs 92% at 1 year and 48% vs 54% at 5 years; χ2=4.04, p=0.0444) and smoking status (87% vs 100% at 1 year and 56 vs 100% at 5 years; χ2=6.55, p=0.0105).
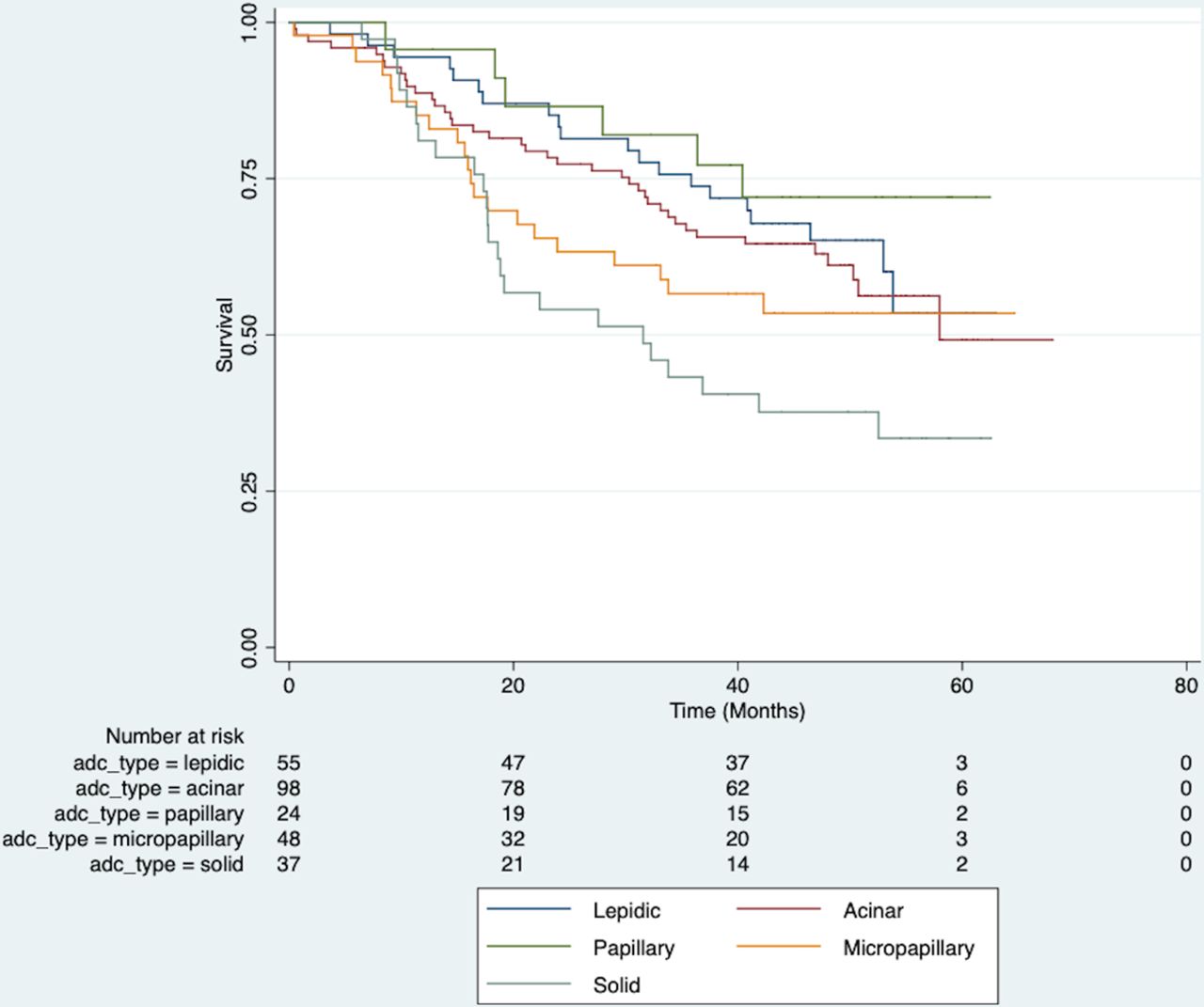
Solid predominant adenocarcinomas exhibited a significantly worse OS than other histopathological subtypes when compared with lepidic predominant adenocarcinomas (p=0.008) (figure 3). Other variables analysed included age, gender, performance status and intra-alveolar spread or STAS. The presence of STAS was identified across all operation types. Furthermore, patients undergoing pneumonectomy (p=0.043) and bilobectomy (p=0.022) exhibited significantly worse OS than those undergoing segmentectomy or lobectomy: 26.5 months (range 6.5–56.5) and 17.7 months (range 7–60 months) versus 47.6 months (range 22.3–54.5 months) and 43.1 months (range 0.4–68.1) respectively, probably reflecting more locally advanced tumour (table 2).
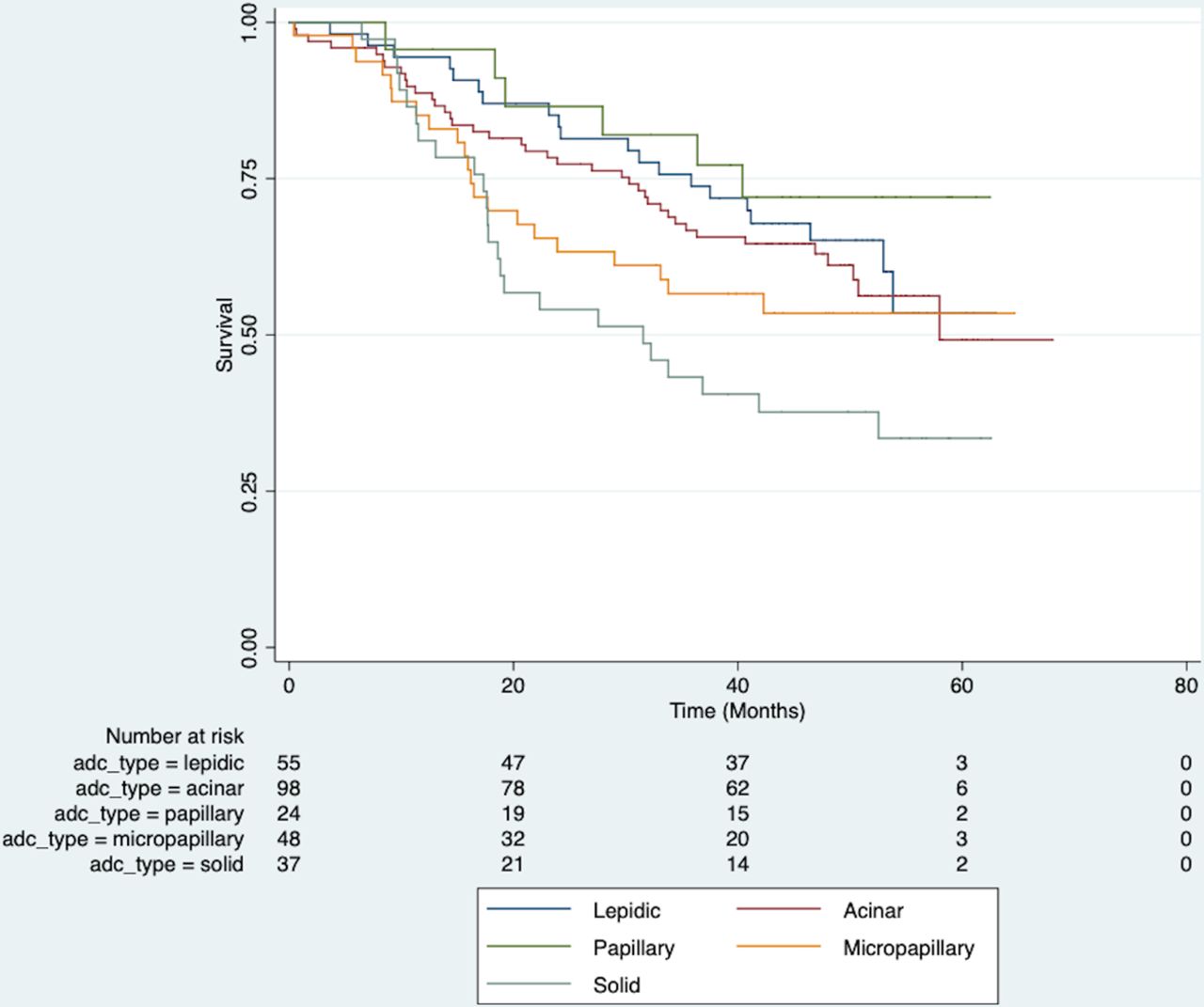
Effect of tumour subtype on overall survival. Solid adenocarcinomas had a worse overall survival than other subtypes compared with lepidic (p=0.008).
The association of the solid component and STAS with sex, age, smoking history, lymphovascular invasion, visceral and parietal invasion and lymph node status did not show any significant correlation.
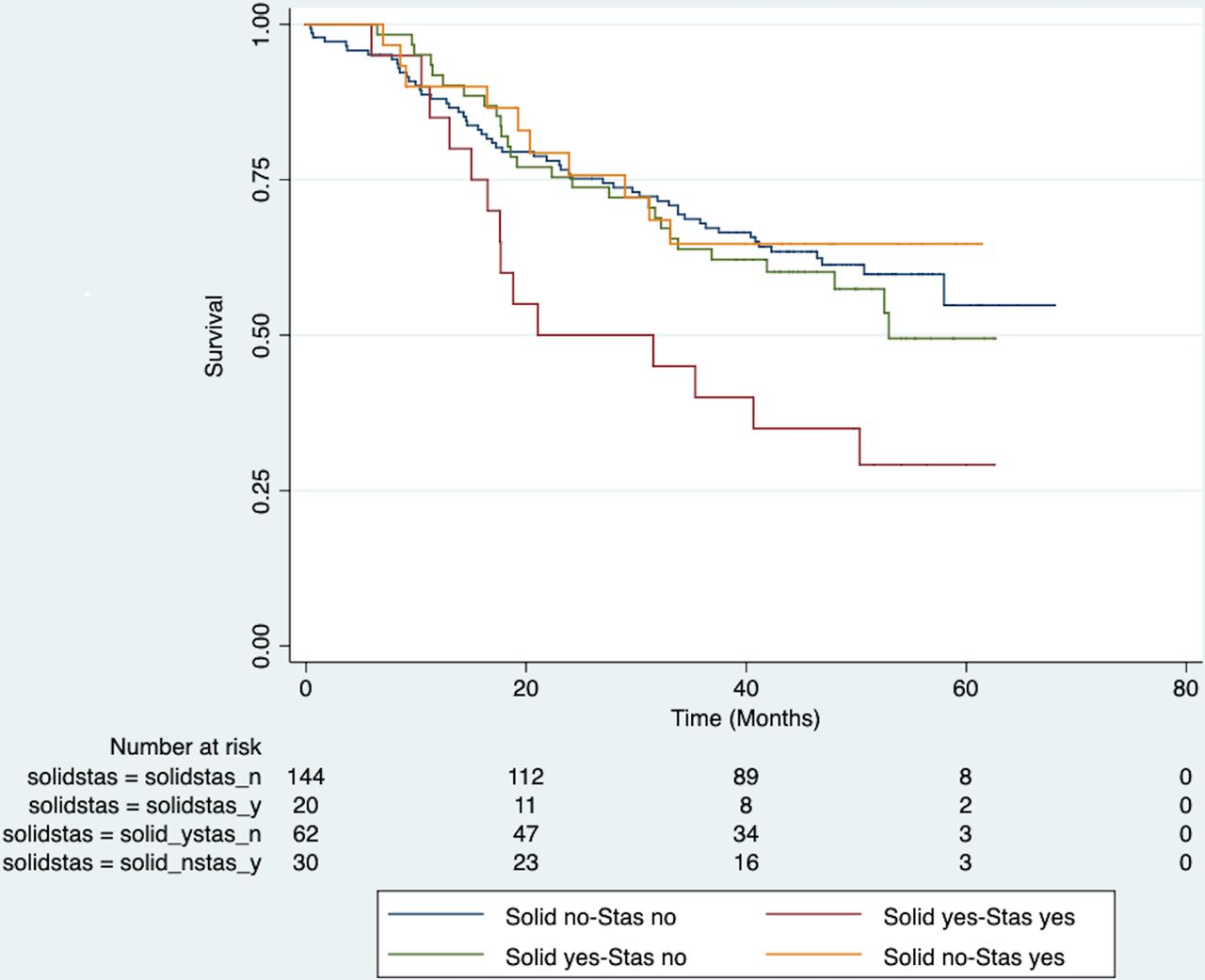
Additional analysis was performed based on literature reports, looking at the concomitant presence of both intra-alveolar spread and solid predominant disease. This demonstrated a significantly worse survival in these patients (n=20; p=0.01, HR 2.18, CI 1.2 to 3.9), when compared with those without either solid component or intra-alveolar spread (n=144) (figure 4).

Kaplan-Meier survival based on intra-alveolar spread and solid component. Concomitance of solid predominance and presence of intra-alveolar spread showed significantly worse survival (p=0.01, HR 2.18, CI 1.2 to 3.9).
Disease-free survival
Of the 262 patients, data were available on recurrence in 163 cases. Of these, 72 (44%) exhibited disease recurrence during the study period. Date of recurrence were available in 60 of the 72 patients with recurrent disease and these 60 were included in analysis of disease-free survival (DFS). Mean time to recurrence was 20.6±14.6 months. Univariable analysis did not show any significant impact of gender, age, operative site, performance status, intra-alveolar spread (STAS) or lymphovascular invasion on DFS. Advancing stage was an overall predictor of shorter DFS (p=0.046), as were the presence of parietal pleural (χ2 11.62, p=0.0007) and chest wall invasion (χ2 21.32, p<0.0001). Patients with solid tumours again tended to have shorter DFS (figure 5), however, adenocarcinoma subtype did not significantly impact on DFS in this patient cohort.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of tumour subtype on disease-free survival. Solid adenocarcinomas had a shorted disease-free survival overall, but not statistically significant.
Subgroup analysis
Subgroup analysis was performed by stage, analysing the characteristics in the different stage categories. As expected, OS was better in earlier stage (IA-IIA) tumours with a 1-year, 3-year and 5-year survival of 90.6%, 73.6% and 58.8%, respectively compared with stages IIB and IIIA. The presence of lymphovascular invasion (p=0.0016), visceral pleural (p=0.048) and parietal pleural (p<0.0001) invasion remained significant univariate predictors of worse OS in every stage subgroup. In stage IA-IIA tumours adenocarcinoma subtype and STAS were not a significant predictor of OS. However, in this specific subgroup, the presence of intra-alveolar spread and solid predominant tumour subtype together (N=12) again resulted in significantly worse OS than in those without either solid component or intra-alveolar spread (N=105) (HR 2.65, 95% CI 1.22 to 5.77, p=0.014).
Multivariate regression model
A Cox proportional hazard, multivariate model was used to determine significant survival predictors. Significant interaction was seen between the variables of lymphovascular invasion and parietal pleura invasion as well as between age and intra-alveolar spread and these were incorporated into the final model. Confirmation that the proportional hazard assumption met was assessed through Schoenfeld residuals (global test: χ2=2.26 p=0.659). The fully adjusted model including interaction variables is shown in table 3. In this model advancing age (p=0.021), stage above IIa (all p<0.01), lymphovascular invasion (p=0.002) and intra-alveolar spread (p=0.009) were all significant independent predictors of worse OS outcome. Solid adenocarcinoma subtype was not an independent prognostic factor.
Multivariate Cox regression model: n=26; LR χ2=66.38; df=15; p < χ2 ≤0.00001
Discussion
Lung adenocarcinoma is the most frequent nonsmall cell lung cancer subtype. Currently, TNM staging remains the strongest predictor of survival and, together with tumour size, is the basis on which patients are offered adjuvant treatment after surgical resection.17 18 Among patients with the same pathological staging, a number of biological tumour characteristics may contribute to determine the prognosis and the risk of recurrence. Recently, adenocarcinoma subtype, lymph vascular invasion and intraalveolar spread have been investigated as potential prognostic factors.
The rates of the predominant adenocarcinoma subtypes vary in the literature.19 As previously reported OS is affected by predominant adenocarcinoma subtype: solid and micropapillary subtypes are associated with worse long-term prognosis.20–23 Our results demonstrated that the solid histological subtype, regardless of the expression percentage, conferred the worst OS identifying it as an independent negative prognostic factor for survival. These results are consistent with a recent study by Li et al 24 who also demonstrated a worse survival in solid adenocarcinoma subtypes. Solid component is associated with features of aggressive behaviour such as lymph node involvement, lymphovascular invasion as reported by Li J, which may account for worse long-term prognosis.23 25
We found that patients with solid tumour subtype and tumour STAS had a significantly worse prognosis than those who did not have either biologic tumour characteristic. The poor prognostic role of solid histologic subtype of adenocarcinoma is well reported, particularly most recently in a systematic review and meta-analysis by Miyahara et al.26 In our series, the combined effect of solid subtype and tumour intra-alveolar spread is even more marked, particularly in earlier stages (stage IA-IIA; HR 2.65, 95% CI 1.22 to 5.77, p=0.0.014).
Clinical stage and tumour size were the major criteria to determine the extent of resection27 and the adjuvant treatment. The correlation between histological subtype and survival, and the impact of STAS demonstrated in our findings, can provide a more accurate assessment of whether a wide resection is appropriate (sublobar vs lobar resection), even for small peripheral tumours. We have previously reported, together with various authors, on the prognostic impact of tumour lymphovascular invasion.28 We reported that even in early stage lung cancer, the presence of tumour lymphovascular invasion conferred a worse OS and correlated with the likelihood of lymph node metastases. It could be argued that the presence of these biologic markers of tumour aggressiveness (tumour lymphovascular invasion, intra-alveolar spread, solid subtype) should at least be investigated as criteria for adjuvant therapies in prospective clinical trials.
As limitations, this is a single centre retrospective study and the simple size of the study is smaller than other groups, such as the 2018 solid component study,24 but all the cases were reviewed by a dedicated thoracic pathologist, and the predominant subtype was classified objectively using proprietary software to minimise interpretations bias.
Conclusion
In conclusion, our results demonstrate that solid predominance with intra-alveolar spread and lymphovascular invasion confer a worse prognosis and, therefore, should be used as a prognostic tool when determining the appropriate treatment for patients. STAS is a novel criterion that can help to further stratify patients after lung resection who may benefit from adjuvant treatment. The impact of these prognostic factors on adjuvant chemotherapy remains unclear and further studies on adjuvant treatment based on these biological characteristics rather than the size criteria only are needed.
Take home messages
Solid predominance in lung adenocarcinoma confers a worse prognosis.
Intra-alveolar spread is an independent predictor of survival.
Copresence of intra-alveolar spread and solid predominance significantly reduce overall survival.
Tumour type and intra-alveolar spread should be used as a prognostic tool to determine appropriate adjuvant treatment.
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. The retrospective database including all data collected will be available upon reasonable request.
Ethics statements
Patient consent for publication
References
Footnotes
Handling editor Runjan Chetty.
Contributors All named authors have made a significant contribution towards the design, data acquisition and analysis, statistical analysis and writing of the final manuscript. AB has been responsible for the overall supervision of the project.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.