Article Text

Abstract
Aims While the SARS-CoV-2 pandemic may be contained through vaccination, transfusion of convalescent plasma (CCP) from individuals who recovered from COVID-19 (CCP) is considered an alternative treatment. We investigate if CCP transfusion in patients with severe respiratory failure increases plasma titres of SARS-CoV-2 antibodies and improves clinical outcomes.
Methods Patients with COVID-19 (n=34) were consented for CCP transfusion and serial blood draws pretransfusion and post-transfusion. Plasma SARS-CoV-2 antireceptor binding domain (RBD) IgG and IgM titres were measured by ELISA serially, and compared with serial plasma titre levels from control patients (n=68). The primary outcome was survival at 30 days, and secondary outcomes were length of ventilator and/or extracorporeal membrane oxygenation (ECMO) support, length of stay (LOS) in the hospital and in the intensive care unit (ICU). Outcomes were compared with matched control patients (n=34). Kinetics of antibodies and clinical outcomes were compared using LOess regression and ORs, respectively.
Results Prior to CCP transfusion, 74% of patients were anti-RBD seropositive for IgG (median 1:3200), and 81% were anti-RBD IgM seropositive (median 1:320), while 16% were seronegative. The kinetics of antibody titres in CCP recipients were similar to controls. CCP recipients presented with similar survival, duration on ventilatory and/or ECMO support, as well as ICU and hospital LOS compared with controls.
Conclusions CCP transfusion did not increase the kinetics of SARS-CoV2 antibodies and did not result in improved clinical outcomes in patients with COVID-19 with severe respiratory failure, suggesting that CCP may not be indicated in this category of patients.
- antibodies
- blood transfusion
- COVID-19
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The current global health crisis posed by the SARS-CoV-2 pandemic demands urgent containment through vaccine development and distribution. The management of COVID-19 has nonetheless improved given refined supportive therapies including hyperoxygenation, steroids, remdesivir and anticoagulation.1 Another therapy that has been investigated is passive antibody administration through transfusion of convalescent plasma (CCP) (ie, plasma collected from individuals who have recovered from COVID-19) to prevent the development of severe COVID-19.2 Historically, CCP has been transfused successfully as postexposure prophylaxis and/or treatment for various pathogens, including other coronaviruses (eg, SARS-1, Middle East Respiratory Syndrome).3 Administration of CCP was first attempted during the early stages of the COVID-19 pandemic in China, where it was reported to confer clinical benefit as reflected by faster viral clearance and improved survival.4 5 Today, over 250 000 patients have been transfused with CCP safely in the USA. The Mayo Clinic published preliminary results, citing that the CCP was associated with reduced mortality in recipients early after symptom onset compared with recipients hospitalised for at least 7 days in the intensive care unit (ICU).6 However, conflicting studies have shown no survival benefit when CCP is transfused to critically ill patients with advanced respiratory symptoms.7
The sponsoring institution of the current study, the University of Maryland Medical Center, has one of the highest acute level care and ICU capacities in the USA and has been uniquely prepared to treat COVID-19 with different emerging therapies, including CCP. We evaluated the longitudinal profiles of SARS-CoV-2 antibody titres in plasma from critically ill patients with COVID-19 before and after CCP transfusion and compared them to those measured in patients not transfused with CCP. Additionally, clinical outcomes of CCP recipients were compared with those from a matched control group.
Methods
Study design
This is an observational retrospective control study to investigate the development of the humoral immune response to SARS-CoV-2 in CCP recipients (n=34) and compare it to the humoral response in a group of patients not treated with CCP (n=68, control A). A separate comparison of clinical outcomes is performed between CCP recipients and a matched control group of patients untreated with CCP (n=34, control B).
CCP treated subjects
Patients considered for enrollment in the study presented with severe COVID-19 and were hospitalised in the ICU at University of Maryland Medical Center and at two other sister hospitals. Patients were evaluated by an infectious disease clinician based on Federal Drug Administration (FDA) recommended guidance.2 An institutional ethics committee reviewed the indication of each CCP transfusion. Patients less than 18 years old were excluded. Informed consent was obtained, and CCP was transfused following FDA authorisation. All CCP transfusions occurred between 17 April 2020 and 19 July 2020. CCP units with a SARS-CoV-2 antibody titre >1:160, per FDA guidance, were procured by the regional blood centre.2 Patients received a single unit of ABO compatible CCP of approximately 250 mL. Following transfusion, CCP recipients were closely monitored for a minimum of 4 hours for possible transfusion-related adverse events. Blood samples for SARS-CoV-2 antibody titre measurements were collected immediately pre-transfusion (day 0) and on days 3, 7 and 14 post-transfusion. Data from three of the CCP recipients were excluded from the kinetics analysis due to insufficient plasma sample quantity; these were still included in the clinical outcome analysis.
Non-transfused control subjects
Non-transfused patients (control A) were used for comparison of antibody titres. Remnant plasma samples from non-transfused control A patients were aliquoted 1–3 days following collection and stored at −70°C prior to antibody titre measurement. Sample draws ranged from 0 to 48 days after the onset of symptoms, which varied in severity.
Non-transfused patients (control B), used for the clinical outcome analysis, were matched to CCP recipients based on sex, age, and on three levels of respiratory support requirement (non-ventilated, mechanically ventilated and ventilated with extracorporeal membrane oxygenation (ECMO)) and were admitted in the same hospital. Patients who were administered CCP at an outside institution prior to their admission, pregnant, or had instructions not to escalate care (do not intubate (DNI)/do not resuscitate (DNR)) were excluded as controls. Seven non-transfused-patients were included in both control A and control B.
Clinical data collection and outcomes
After enrolment, the following clinical variables were collected from electronic medical records: symptoms at presentation, level of respiratory support (mechanical ventilation/ECMO status), comorbidities, other SARS-CoV-2 directed therapies, 30-days in-hospital mortality, number of days on mechanical ventilation, number of days on ECMO support, ICU length of stay (LOS) and hospital LOS. Clinical improvement was assessed primarily on survival at 30 days. Secondary outcomes included the number of days on ventilatory and/or ECMO respiratory support, LOS in the hospital and LOS in the ICU.
Antireceptor binding domain ELISA
SARS-CoV-2 spike protein receptor-binding domain (RBD) was produced following the protocol of Stadlbauer et al, 2020.8 RBD was used for anti-RBD IgG and IgM ELISAs. In brief, ELISA plates (Thermo Fisher Scientific, Waltham, Massachusetts, USA) were precoated overnight with RBD. Plates were washed, blocked, washed again before an eight-step, fourfold serial dilution ladder (starting at 1:100 for IgG or 1:40 for IgM) of plasma samples were added and incubated for 1 hour. The wells were then washed, incubated for 1 hour with either Horseradish Peroxidase conjugated goat-antihuman IgG or IgM detection antibody (1:12000) (Invitrogen), washed, incubated with 3,3′,5,5′-Tetramethylbenzidine substrate (Seracare; Milford, Massachusetts, USA) for 10 min in the dark, quenched with 1N sulfuric acid (Thermo Fisher Scientific), and read at an absorbance of 450 nm. Seroconversion was defined as any measurement of anti-RBD IgG or IgM greater than or equal to 1:100 (IgG) or 1:40 (IgM) titres.
Samples collected from patients prior to the COVID-19 pandemic (collected in 2012) served as negative controls, while plasma samples from individuals with PCR confirmed SARS-CoV-2 infections served as positive controls. Negative controls and three dilutions of pooled plasma from positive controls were measured on all plates. Specificity was evaluated using plasma samples from negative controls. Positive controls (n=24) samples were also measured on the Ortho VITROS total anti-SARS-CoV-2 Ig platform.
Statistical analysis
Statistical significance in table 1 was determined using Fisher’s exact test for the categorical variables and Welch’s one-way ANOVA for the continuous and normally distributed Age variable. Plots of antibody titres versus days postsymptom onset were evaluated using loess regression analysis with a span of 0.75% and 95% CIs. A Kruskal-Wallis test was used to compare the non-normally distributed antibody titre distributions. ORs with Wald CIs and p values were used to compare secondary outcomes. An alpha value of 0.05 or less was considered statistically significant. Statistical analysis was performed using R statistical software (Foundation for Statistical Computing; Vienna, Austria) and Prism V.8 (GraphPad; San Diego, California, USA).
Demographics and clinical characteristics
Results
Validation of anti-RBD IgG and IgM ELISAs
Positive control samples (n=24), from individuals with PCR confirmed SARS-CoV-2 infections, were tested on the ELISA and the Ortho VITROS platform. On the ELISA, 22/24 samples were seropositive for anti-RBD IgG with a median titre of 1:6400 (figure 1A) while 23/24 were seropositive for anti-RBD IgM with a median titre of 1:240 (figure 1B). The Ortho VITROS platform detected SARS-CoV-2 antibodies in the majority of samples (22/24) at a median signal to cut-off ratio (S/C) of 490 (figure 1C). Two samples with IgM titres of 1:40 and undetectable IgG were negative by the Ortho VITROS method.

Comparison of antibody titres using different testing platforms. COVID-19 positive control samples (n=24) were measured on the anti-RBD IgG (A) and IgM (B) ELISAs as well as on the Ortho VITROS total anti-SARS-CoV-2 Ig platform (C). ELISA measurements reported as titres and were converted to a log 10 scale (A, B). Ortho VITROS measurements reported as signal to cut-off ratio (S/C) (C). IgG titres below 1:100, IgM titres below 1:40, and S/C values below 1.0 were considered negative. Bars represent the median and IQR (A–C). Titers are shown on logarithmic scale. RBD, receptor binding domain.
Characteristics of CCP recipients compared with non-transfused patients
CCP transfusion was considered and reviewed by an infectious disease expert, for 41 patients with COVID-19, of whom 34 patients were transfused with CCP on obtaining consent. Reasons for non-transfusion included patients or legally authorised proxy changing their mind about the treatment. The anti-RBD IgG and IgM responses of CCP recipients were compared with those of 68 non-transfused control patients (control A); CCP recipients presented with more severe disease requiring ECMO support, but both groups were similar in terms of sex and age (table 1).
CCP recipients and matched non-transfused patient (control B) had similar frequencies of comorbidities, symptoms at presentation and other COVID-19 directed therapies administered during hospitalisation (table 1). ABO type distribution was different between the groups, although it was not available on eight of the 34 (23.5%) matched control patients (table 1).
Kinetics of anti-RBD IgG and IgM responses in CCP recipients and non-transfused patients
Anti-RBD IgG and IgM responses were examined based on titre levels measured in plasma samples drawn on successive days post-onset of symptoms (POS), starting on the day of transfusion in CCP recipients, which was a median of 12 days POS, and a median of 10 days POS in non-transfused control A patients.
The frequency of patients who generated an anti-RBD IgG and/or an IgM response was similar in CCP recipients compared with controls ((frequency of IgG response: 100% (31/31) and 100% (68/68)) (frequency of IgM response: 96.8% (30/31) and 100% (68/68)). Furthermore, the seroconversion rate for both anti-RBD IgG and IgM, analysed using a cumulative frequency plot, was similar in CCP recipients compared with controls (figure 2A,B). The longitudinal profiles of anti-RBD IgG responses showed a peak between 20 and 30 days POS and slowly decayed thereafter for both CCP recipients and controls (figure 2C). The anti-RBD IgM response peaked between 15 and 25 days POS and rapidly decayed thereafter for both CCP recipients and controls (figure 2D).

Kinetics of anti-RBD IgG and IgM responses in CCP recipients and control patients. Cumulative frequency, as the per cent of seropositive CCP recipients (celeste blue line) and control patients (pink line), were plotted against the number of days postonset of symptoms (POS). Seropositive was defined as any titre measurement of IgG (A) or IgM (B) greater than 1:100 and 1:40, respectively. CCP recipients and controls were assumed to be seronegative prior to the first measurement (A, B). Scatter plots were used to display IgG (C) and IgM (D) responses as a function of days POS and a loess regression with a span of 0.75 was used to indicate overall trends. Shadings show the 95% CI for CCP recipients (dashed line, blue CI) and control patients (solid line, pink CI) (C, D). Bold X’s denote highest titres achieved by patients who were seronegative at the time of transfusion and did not survive (C, D). Vertical dashed line represents median days POS at which transfusion occurred (A–D). All titre levels were converted to a log 10 scale. Titers are shown on logarithmic (LOG) scale. CCP, convalescent plasma; RBD, receptor binding domain.
The kinetics of individuals’ anti-RBD IgG and IgM response were also compared between CCP recipients (figure 3A,B) and non-transfused control A patients (figure 3C,D). As was observed at the overall population level in figure 2, the kinetics of the anti-RBD IgG and IgM responses in CCP recipients and control groups at the individual patient level were similar (figure 3A–D). Furthermore, IgG and IgM titres increased with higher respiratory support requirement in both CCP recipients and controls (figure 3A–D).
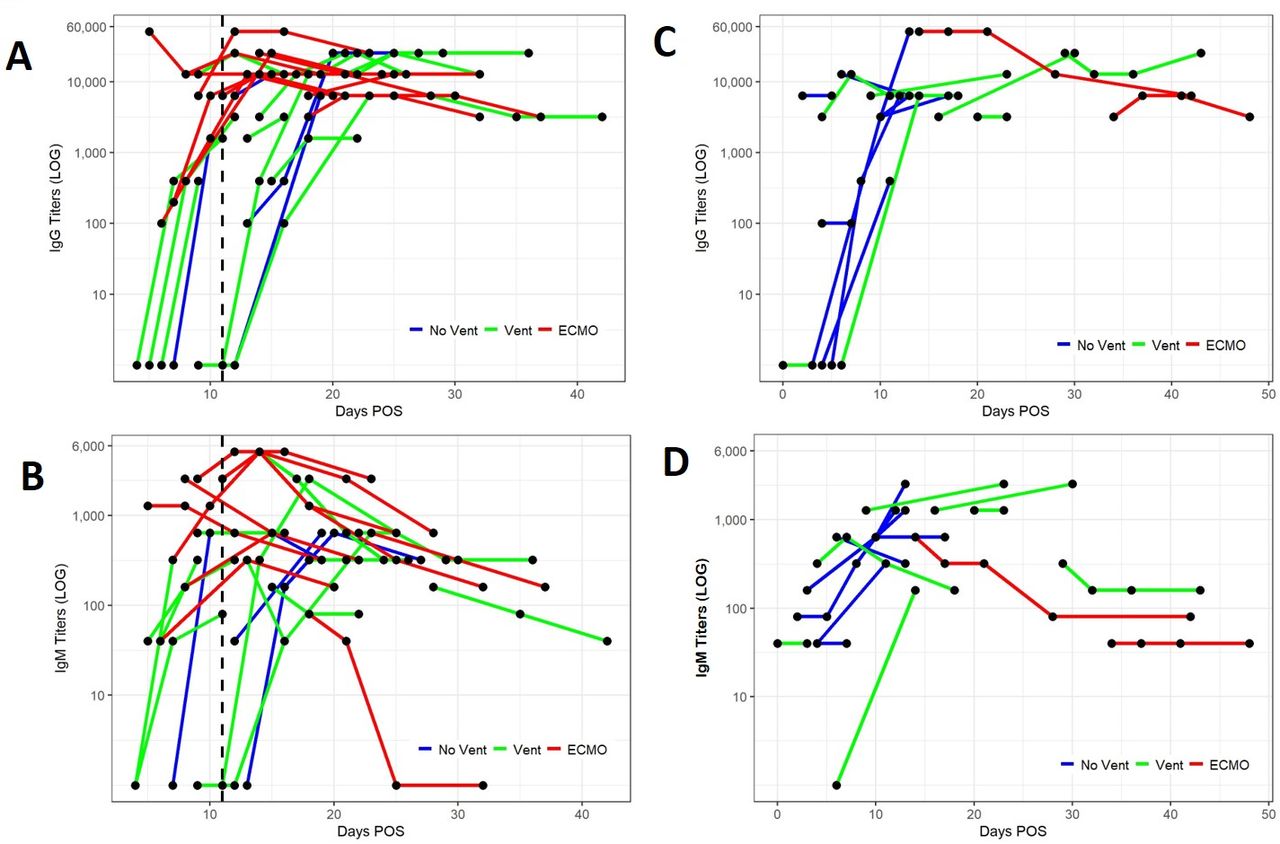
Anti-RBD IgG and IgM longitudinal responses of individual CCP recipients and control patients. For CCP recipients, the first data point of each line represents patient IgG (A) and IgM (B) antibody titres immediately prior to CCP transfusion, and subsequent dots represent titres on post-transfusion days (3,7 and 14). The vertical dashed line represents median days postonset of symptoms (POS) at which transfusion occurred. For control patients, individual anti-RBD IgG (C) and IgM (D) titre longitudinal responses are shown on each line with each dot representing titres measured on sequential days POS. Only controls with sequential data points are shown (C, D). CCP and control patient samples are stratified based on the level of respiratory support needed; no ventilation (dark blue), ventilation only (green) or ECMO (red) (A–D). All titre levels were converted to a log 10 scale. Titers are shown on logarithmic (LOG) scale. CCP, convalescent plasma; ECMO, extracorporeal membrane oxygenation; RBD, receptor binding domain.
Immediately prior to CCP transfusion, 23/31 (74.2%) patients were anti-RBD IgG seropositive (median titre 1:3200, range 1:50–1:9600) (figure 3A), and 25/31 (80.6%) patients were anti-RBD IgM seropositive (median titre 1:320, range 1:40–1:640), (figure 3B), while 5/31 (16%) patients were seronegative for both. Interestingly, three out of these five CCP recipients died within 30 days of transfusion, one of whom was a recent kidney transplant recipient on immunosuppressive therapy. The highest anti-RBD IgG and IgM titres achieved by these three CCP recipients were similar to titres from non-transfused patients, measured at about the same number of days POS (figure 2C,D). For non-transfused control A patients, at the time of initial sample collection 52/68 (76.5%) patients were anti-RBD IgG seropositive (median titre 1:3200, range 1:100–1:6400), and 63/68 (92.6%) patients were anti-RBD IgM seropositive (median titre 1:160, range 1:70–1:640), while 4/68 (5.9%) patients were seronegative for both.
Anti-RBD IgG and IgM titre distribution in CCP recipients and in non-transfused patients
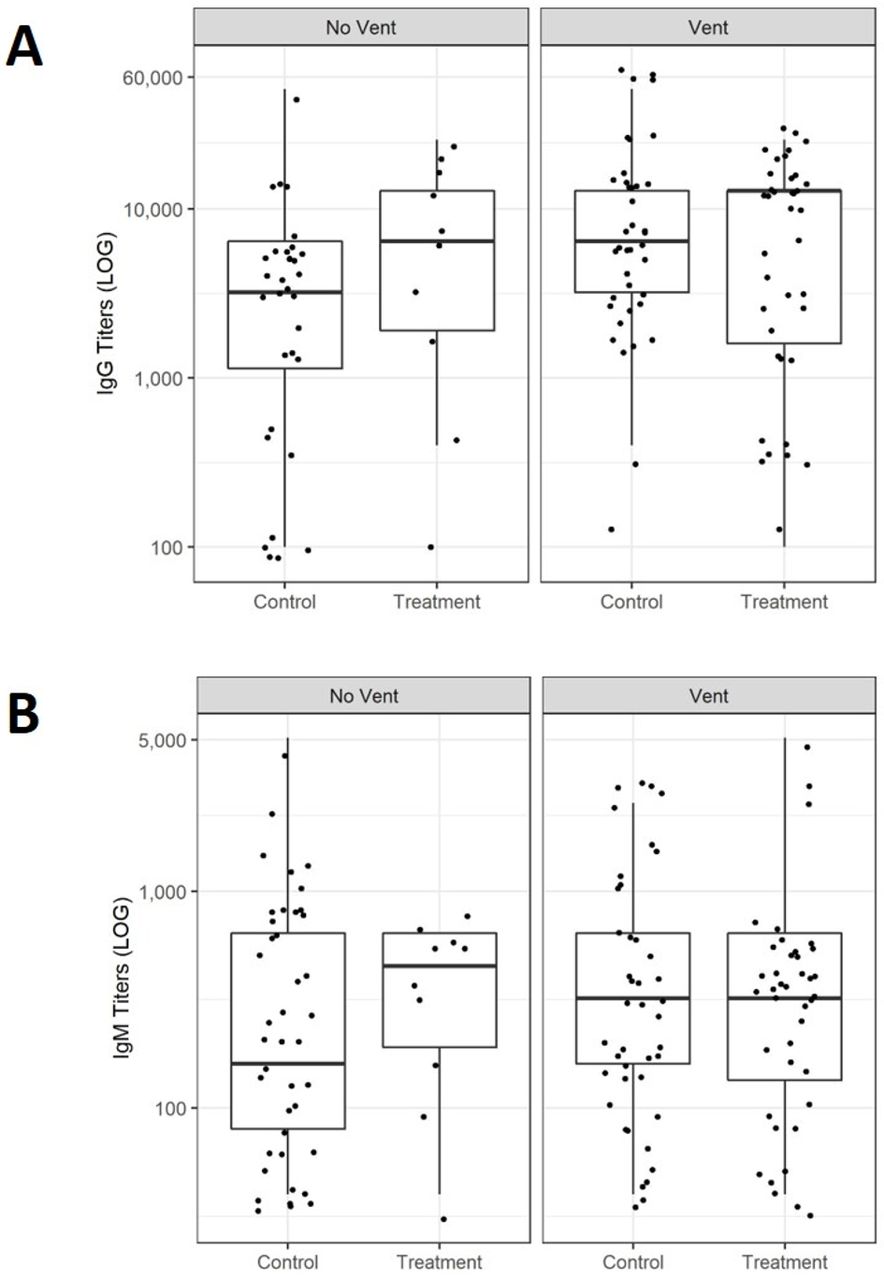
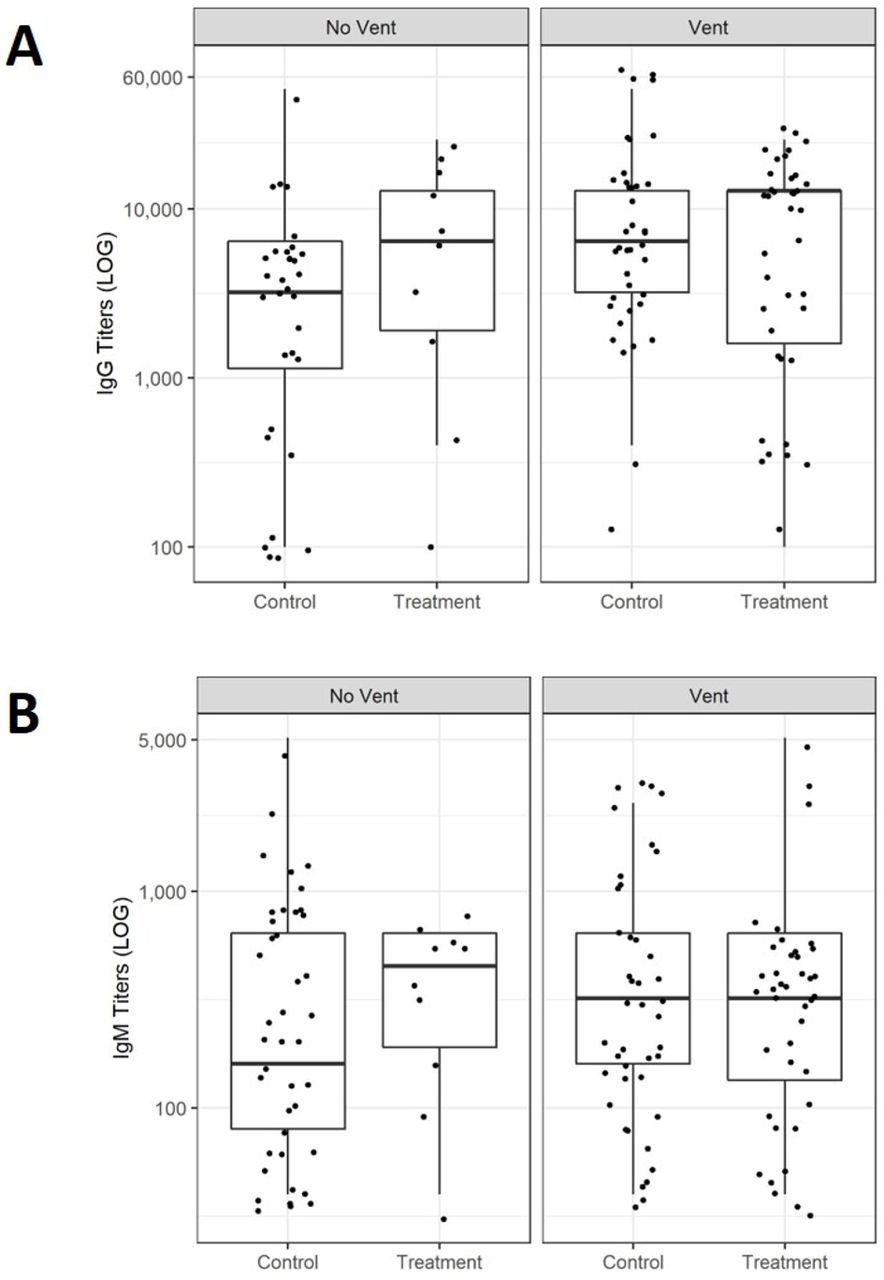
Next, we compared the distribution of anti-RBD IgG (figure 4A) and IgM (figure 4B) titres between CCP recipients and non-transfused patients (controls A) depending on the level of respiratory support needed. In non-ventilated patients, anti-RBD IgG and IgM titres were similar in CCP recipients compared with controls (IgG Median titres: 1:6400 and 1:3200 (figure 4A)), (IgM median titres: 1:480 and 1:160 (figure 4B)). In mechanically ventilated patients anti-RBD IgG and IgM titres were similar in CCP recipients compared with controls (IgG median titres: 1:12 800 and 1:6400 (figure 4A)), (IgM median titres: 1:320 and 1:320 (figure 4B)). CCP recipients on ECMO had similar anti-RBD IgG titres compared with patients on ECMO (IgG median titres: 1:12 800 and 1:6400). In contrast, IgM titre levels were higher in CCP recipients vs controls on ECMO (1:640 and 1:80, respectively) due to a difference in the number of days POS at which samples were drawn. Indeed CCP recipients and control A samples were not matched for POS for comparison. IgM measurements for CCP recipients on ECMO were taken at a median of 18 days POS compared with 28 days POS for control A patients on ECMO.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anti-RBD IgG and IgM response distributions in patients with COVID-19 stratified by disease severity and respiratory support needed. Distribution of anti-RBD IgG (A) and IgM (B) titres in CCP patients compared with controls depending on the level of respiratory support needed no ventilator (vent), ventilator only. Seronegative samples were excluded (A, B). Statistical analysis was performed using a Kruskal-Wallis test. An alpha value of 0.05 or less was considered statistically significant. All titre levels were converted to a log 10 scale. CCP, convalescent plasma; RBD, receptor binding domain.
Clinical outcomes of CCP recipients and non-transfused (matched control B) patients
CCP recipients and matched control patients with COVID-19 (control B) presented with similar 30-day in-hospital mortality (table 2). When stratifying the two groups based on disease severity, no difference in 30-day in-hospital mortality was observed (table 2). Additionally, CCP recipients and matched controls were similar in their respective median ICU LOS and median hospital LOS (table 2). The subgroups of CCP recipients also had similar ICU LOS and hospital LOS when compared with their respective matched control subgroups (table 2). CCP recipients and matched controls also had a similar median number of days on mechanical ventilation and median duration on ECMO (table 2).
Comparison of secondary clinical outcomes in subgroups of COVID-19 severity
Discussion
The kinetics of SARS-CoV-2 IgG and IgM antibodies from plasma of patients with COVID-19 transfused with CCP were comparable to those from a cohort of patients with COVID-19 who did not receive CCP. Furthermore, most CCP recipients already had detectable SARS-CoV-2 antibodies in their plasma prior to transfusion. The highest SARS-CoV-2 antibody titres were observed in the plasma of the sickest subgroup of patients requiring both ventilatory and ECMO support. CCP recipients compared with matched control patients did not show any mortality benefit at 30 days post-transfusion, nor a reduction in either ICU or hospital LOS, or duration of mechanical ventilation/ECMO support; similarly subgroups comparisons based on disease severity, showed no difference in outcomes.
While some of the current findings corroborate results from earlier studies, they contradict others. Hegerova et al reported a modest survival benefit in a matched control study of patients with severe COVID-19 following CCP transfusion within 7 days of hospitalisation.9 A prospective, propensity score-matched study showed that patients transfused with CCP within 72 hours of admission experienced the most benefit compared with the control group.10 By contrast, in an open-label, randomised controlled trial (PLACID TRIAL), CCP was not associated with a reduction in overall mortality or progression to severe COVID-19,11 even when administered within 72 hours of symptoms onset. A retrospective study from March 2020 with 10 patients showed improved oxygenation and better patient survival following CCP transfusion.12 However, 4 of the 10 patients had high (>1:640) SARS-CoV-2 neutralising antibody titres prior to CCP transfusion, suggesting that the patients’ own immunity may have been responsible for the recovery rather than CCP transfusion. Nevertheless, these data suggest the need to prioritise CCP transfusion to patients with COVID-19 within 3–5 days of symptom onset when antibody production is still in the fledgling stages, or in those patients who are immunosuppressed (eg, hypogammaglobulinaemia).13 However, in the current study, three of the CCP recipients who were seronegative prior to transfusion died within 30 days, one of these was a kidney transplant recipient who was receiving T-cell immunosuppression prior to COVID-19 diagnosis, suggesting that T cell response may also be important for controlling SARS-CoV-2 during the acute phase of the infection. T-cell immune responses were not assessed in the current study, but further flow cytometry analyses characterising the profile of lymphocyte subsets in patients with COVID-19 are underway in our laboratory to confirm results from other studies. Indeed a study by Peng et al showed that both SARS-CoV-2 antibody and memory T cell responses were stronger in patients who had recovered from severe disease.14 But patients with COVID-19 with severe disease and who died showed a significant quantitative and functional reduction in CD4 and CD8 T cells.15
The rise of antibody titres in the present study was expected to be higher in CCP recipients on days 2–3 post-CCP transfusion, but it remained similar to the rise observed in control patients. An increase in antibody titres may have been observed if the patients had been drawn for a plasma titre within 24 hours post-CCP transfusion. In a randomised control trial, PlasmAr Study, of 215 patients with severe pneumonia, total SARS-CoV-2 antibody titres were higher in the CCP treated group at day two post-transfusion. Still, no effect on 30-day clinical outcome and mortality between treated vs placebo groups was observed.7 Similarly, in the current study, most patients treated with CCP presented with severe COVID-19, requiring ventilatory support and/or ECMO. The antibody response increased proportionally with the severity of COVID-19, which was also previously reported.16–18
While the exact SARS-CoV-2 antibody titres in CCP units were unknown, these titres should have been greater than 1:160. Exogenous IgG antibodies typically have a half-life of 21 days and should last in the peripheral blood for at least 3 months.19 20 But the kinetics of the individual patient antibody response to SARS-CoV-2 make it difficult to determine the impact of CCP on the titres following CCP administration. Additionally, individuals that received CCP already had high antibody titres of 1:3200 on average and the addition of CCP was not likely to have a measurable impact on antibody titres given the dilutional effect. For example, if a patient received CCP with a 1:200 titre and the volume of plasma given accounted for less than 1/10 of the patient’s plasma volume, the end result would be a ~1:20 titre, which would be negligible for a patient with a 1:3200 titre.
The strength of this study is based on the characterisation of the kinetics of SARS-CoV-2 antibodies following CCP transfusion, which has not been previously described longitudinally in comparison to control plasma samples from non-transfused patients with COVID-19. Times of seroconversion and antibody kinetics in patients transfused with CCP were similar to that of non-transfused patients. These suggest that the antibodies measured are mostly the ones naturally produced by the patients’ immune system rather than those from the CCP treatment. These data on kinetics of SARS-CoV-2 antibodies are consistent with reports showing patients with COVID-19 in general with detectable IgG and IgM in plasma between four and 7 days POS.21 To strengthen the study, we compared the antibody titre measurements by ELISA to those obtained on a commercially available instrument, the Ortho VITROS total anti-SARS-CoV-2 Ig platform, which had been previously validated against a SARS-CoV-2 neutralising live-cell assay.22 23 The median IgG titres prior to CCP transfusion were high (1:3200). Interestingly, Salazar et al showed that anti-RBD IgG titres greater than 1:1350 correlated with SARS-CoV-2 neutralisation (VN) titres greater than 1:160 at 80% probability.22 The FDA (https://www.fda.gov/media/141477/download) recommended that an IgG titre detected on the Ortho VITROS platform at a S/C of 12 or on the Mount Sinai ELISA at 1:2880 may be considered equivalent to a VN titre >1:250 (https://www.fda.gov/media/141477/download). Furthermore, Luchsinger et al showed that both the Ortho VITROS total Ig and IgG platforms, set at a median S/C values of 101 and 11.7, respectively, correlated well to neutralising antibody results and gold-standard ELISAs.23 Our validation showed that the median anti-RBD IgG titre of 1:6400 in ELISA positive control samples, also tested by the Ortho VITROS total Ig method, showed a median S/C of 490 for total anti-SARS-CoV-2 Ig, suggesting that titres of 1:6400 and 1:3200 on the ELISA used in the present study are much higher than the recommended S/C of 12 and are indicative of high neutralising antibody titres.
There are limitations associated with this study. Although the blood supplier originally qualified the CCP donations as high titre (>1:160), in April 2020,2 the exact titres were not provided. Additionally, this is an observational study, thus the reliability in examining clinical outcomes compared with a prospective, randomised, control trial is not as robust; but at the advent of the first surge of the pandemic, a randomised trial was not practical at our institution. Lastly, the numbers of patients enrolled in each group are small, but the clinical outcomes of CCP recipients were compared with matched control patients hospitalised at the same hospital to decrease bias due to the clustering of enrollment.
In conclusion, the current data may further guide clinicians in defining eligibility criteria for CCP transfusion for the treatment of COVID-19. Indeed, these data do not support CCP transfusion to patients with severe COVID-19, especially if presenting with plasma SARS-CoV-2 IgG and IgM neutralising antibody levels at presentation. Taken together with the current literature, our findings confirm that CCP is probably most effective when administered to patients with low antibody titres, who are earlier in the disease course, and who do not yet have complicated COVID-19.
Take home messages
Kinetics of SARS-CoV-2 antireceptor binding domain (RBD) IgG and IgM titres in convalescent plasma (CCP) recipients were similar to patients with COVID-19 not transfused.
The majority of patients (74%) were seropositive for anti-RBD IgG and seropositive for IgM (81%), prior to transfusion with CCP.
SARS-CoV2 antibodies were proportionally higher in patients with more severe COVID-19 requiring increased respiratory support.
CCP recipients and matched controls showed similar 30-day survival and length of respiratory support as well as length of stay in the intensive care unit and in the hospital.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the University of Maryland Baltimore Institutional Research Subject review board (Protocol HP-00092606).
Acknowledgments
We thank Dr. Wilbur Chen for facilitating the procurement of the plasmids for the RBD production. We also thank all the staff of the Transfusion Services at each University of Maryland Medical Systems hospital. We thank the staff and physicians at both the American Red Cross and New York Blood Centre for their coordinated efforts in providing timely convalescent plasma units to our patients.
References
Footnotes
Handling editor Tahir S Pillay.
Twitter @Fontain1J
Contributors MNK and EWW completed the experimental work and clinical data collection and wrote the manuscript. HB, CD, AM-H, AT and JWB completed the clinical data collection and reviewed and edited the manuscript, PZ completed all statistical analysis and editing of the manuscript. EMB contributed to the design and editing of the manuscript. KEM and MJF designed, supervised the experimental work and wrote the manuscript. All authors have reviewed, edited and approved the manuscript before submission. MJF is the guarantor.
Funding This study was funded by the University of Maryland School of Medicine Department of Pathology funds and by the Biomedical Advanced Research and Development Authority (BARDA).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.