Article Text

Abstract
Aims To elucidate the clinicopathological features and the diagnostic value of mutation specific antibody H3F3 K36M of chondroblastoma (CB) in China.
Methods Clinicopathological profiles were retrieved, and immunohistochemistry was performed on 185 CB specimens and the control group.
Results Our series included 307 patients with a mean age of 22.1 years. Long tubular bones (63.8%, 196/307) were most commonly involved, followed by short bones of the hands and feet (22.1%, 68/307), sesamoid bones (8.1%, 25/307), flat bones and irregular bones (5.9%, 18/307). The most commonly involved site was the proximal femur, followed by distal femur, proximal humerus and calcaneus. The average age in the long bones group (20.3 years) was significantly younger than the short bones group (24.9 years) (p<0.001), sesamoid bones group (24.4 years) (p=0.02) and flat bones and irregular bones group (29.1 years) (p<0.001). Microscopically, aneurysmal bone cyst-like change (63.6%, 117/184), necrosis (43.5%, 80/184) and chicken-wire calcification (26.1%, 48/184) were variably noted. In rare cases, cortical destruction, soft tissue and lymphovascular invasion were identified. Positive immunoreaction with H3F3 K36M was examined in all non-decalcified, all EDTA decalcified, 87.1% hydrochloric acid (HCl) decalcified CB samples and the high-grade sarcoma secondary to CB, but not the control group.
Conclusions CB usually involves the long tubular bones in younger age group. H3F3 K36M can identify K36M mutation with 100% specificity and 100% sensitivity in non-decalcified and EDTA decalcified samples, more than 80% sensitivity in HCl decalcified samples. Virtually, all CBs harbour an H3K36M mutation.
- Bone Neoplasms
- IMMUNOHISTOCHEMISTRY
- Pathology, Surgical
- Morphological and Microscopic Findings
Data availability statement
The data presented in this study are available on request from the corresponding author.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Approximately 70%–95% of chondroblastomas (CBs) and rare non-CB bone tumours were reported to harbour a p.K36M mutation. CBs have been reclassified as benign neoplasms in the fifth edition of the WHO classification. The existence of atypical or malignant CB remains to be controversial.
WHAT THIS STUDY ADDS
The antibody H3F3 K36M can identify K36M mutation in H3F3A or H3F3B gene with 100% specificity and 100% sensitivity in non-decalcified and EDTA decalcified samples. The immunoreactivity retained in a high-grade sarcoma secondary to CB. Curettage and en-bloc resections provide favourable outcome for CB patients, including those with atypical/ aggressive histological and/or imaging features.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Virtually, all CBs harbour an H3K36M mutation. We proposed ‘CB with uncertain malignant potential’ to describe CBs with atypical/ aggressive histological and/or imaging features.
Introduction
Chondroblastoma (CB) is a rare cartilaginous neoplasm that accounts for fewer than 1% of all bone tumours, and most commonly presents as an epiphysial or apophyseal (epiphyseal-equivalent) mass in adolescents and young adults.1 CB usually has a benign clinical course, curettage with packing is curative in most patients. However, rare cases of atypical, metastatic and malignant CB have been documented in the literature.2–5 Extremely rare cases of CB developed malignant transformation to high-grade sarcoma.6–8 The biological behaviour of CB has been controversial. In the latest WHO classification,9 CB has been recategorised as a benign neoplasm from an intermediate tumour. More large cohort of researches on the clinicopathological and radiological characteristics of CB are needed to declare the behaviour of this tumour entity. In addition, 70%–95% of CB were reported to harbour a p.K36M mutation in either H3F3A (chromosome 1) or H3F3B (chromosome 17), with the majority involving the latter.10–14 Mutation-specific antibody H3F3 K36M can be applied to detect these point mutations with high sensitivity and specificity.15 Nevertheless, there are few studies about the expression of the antibody in decalcified specimens and high-grade sarcoma originated from CB. In this study, we sought to better describe the clinicopathological, epidemiological features of CB in China with a large cohort of 307 patients. Furthermore, we evaluated the expression of the mutation specific antibody H3F3 K36M in non-decalcified and decalcified CB and a secondary malignant CB to determine the utility of it in the diagnosis of CB.
Materials and methods
An electronic search of the pathology archives was undertaken to identify CB diagnosed between 2008 and 2021 in our institution. Clinicopathological profiles of 307 cases of CB were retrieved from the electronic medical record system. Two hundred and thirty-four patients had biopsy and/or surgery samples in our hospital while 73 patients were outside consultation cases. Available H&E-stained slides, and immunohistochemistry (IHC) when necessary, were reviewed by two specialist bone tumour pathologists (HZ and QZ). Preoperative radiological images were reviewed by two musculoskeletal radiologists when accessible (DH and JZ).
Decalcification
Decalcification protocols for hydrochloric acid (HCl) and EDTA were showed in table 1. Both HCl and EDTA decalcification solution was replaced every 48 hours, and the specimens were checked daily until the decalcification was complete. Then the specimens were rinsed in running tap water for 1 min prior to histological processing.
Decalcification protocols for HCl and EDTA
Immunohistochemistry
IHC was performed on 3 µm thick formalin-fixed paraffin-embedded full tissue sections using the rabbit monoclonal histone H3F3 K36M mutant antibody (clone RM193, 1:200 dilution, RevMAb Biosciences USA). IHC was performed with an automated IHC stainer (Ventana BenchMark ULTRA, Ventana Medical Systems, Tucson, Arizona, USA). Sections were deparaffinised and pretreated with ULTRA Cell Conditioning Solution 1 (CC1, Ventana, Arizona, USA). The duration of decalcification in both HCl and EDTA was 2–7 days. All the 670 non-CB tumour samples in this study were non-decalcified or EDTA decalcified. H3F3 K36M positivity was recorded when moderate to strong nuclear immunoreaction was determined in more than 10 mononuclear tumour cells but not the multinuclear cells and the background.
Statistical methods
Statistical analyses were performed with SPSS Statistics V.26.0 (IBM), and a p<0.05 was considered statistically significant. Pearson χ2 test was used to compare the distribution of tumour site between two age groups (<25 vs ≥25 years). The age distribution of tumours in four bone types was compared by one-way analysis of variance with multiple comparison.
Results
Clinical findings
Our series included 307 CBs, 225 males and 82 females (male:female=2.74:1). The age of the patients ranged from 5 to 63 years (median 22.1 years) at the time of diagnosis (figure 1A). The most commonly affected site was the proximal femur (25.7%, 79/307), followed by distal femur (12.7%, 39/307), proximal humerus (11.1%, 34/307) and calcaneus (10.1%, 31/307). The site distribution is summarised in table 2. Classified by the shape of the bones, 63.8% (196/307) cases occurred in long bones, 22.1% (68/307) in short bones, 8.1% (25/307) in sesamoid bones and 5.9% (18/307) in flat bones and irregular bones. The cases were divided into two groups, younger group (< 25 years, 205 patients) and older group (≥ 25 years, 102 patients) according to the age at the time of presentation (table 3). Comparing between the four types of bones, the average age of the patients in the long bones group (20.3 years) was significantly younger than the short bones group (24.9 years) (p<0.001), sesamoid bones group (24.4 years) (p=0.02) and flat bones and irregular bones group (29.1 years) (p<0.001). No statistically significant difference was found between the remaining groups. The distribution of tumour differed significantly between the two age groups in our cohort (p<0.001) (figure 1C).
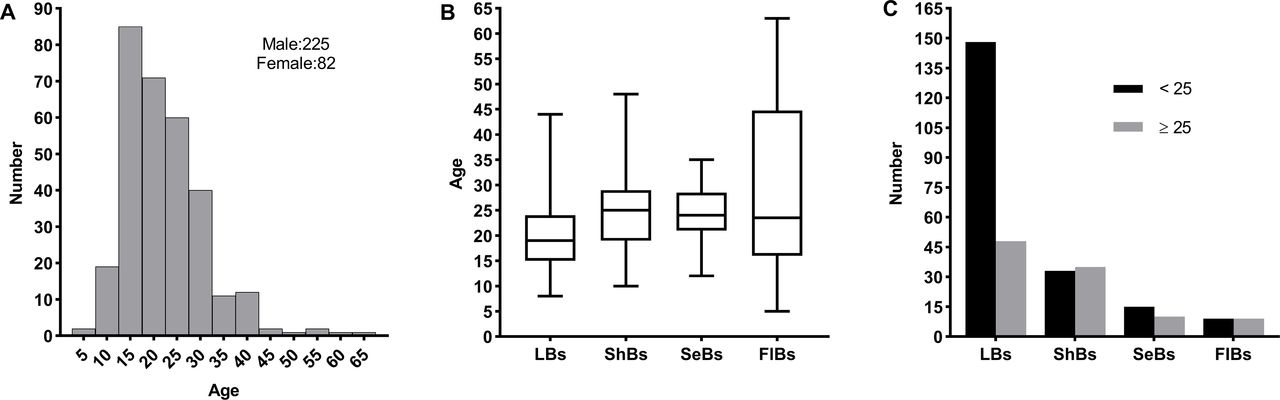
Age and skeletal distribution. (A) Age distribution and gender of 307 chondroblastomas. The mean age and SD at the time of diagnosis was 22.1±8.6 years old. (B) Comparison of the average age of patients in different types of bones. The average age in the long bones group (20.3 years) was significantly younger than short bones groups (24.9 years) and sesamoid bones group (24.4 years) (p<0.05). (C) Comparison of skeletal distribution of CBs in the two age groups (<25 years vs ≥25 years). The distribution differed significantly between the two groups (p<0.01). CBs, chondroblastomas; FIBs, Flat bones and Irregular bones; LBs, long bones; SeBe, sesamold bones; ShBs, short bones.
Site distribution of 307 chondroblastomas
Skeletal distribution classified based on the shape of the bones in the two age groups
In this study, 93.5% (216/231) patients were treated with curettage, 6.5% (15/231) patients underwent en-bloc resection. The remaining three patients went to other hospitals for surgery therapy after biopsy. Chest X-ray or CT scan was taken before surgery in all of the 231 patients treated in our institution, and in 182 patients postoperatively for routine follow-up in the first 2 years after surgery. Only one patient developed lung metastasis in our study, who was a female presented with a well-defined lytic lesion in the distal femur and a solitary nodule in the left lung suggested to be a pulmonary metastasis radiologically in her late 50s. The bone lesion was treated with curettage and diagnosed as CB histologically. Eight months after the initial curettage, the patient developed a local recurrence and en-bloc resection was performed. Bilateral multiple lung metastases were shown by chest X-ray 18 months after the second surgery, but no histological confirmation was available because the patient refused pulmonary biopsy or surgery.
Radiological findings
Preoperative imaging (CT and/or MRI) was available for review for 153 cases. The status of adjacent physis was open in 34/153 (22.2%) patients, and it was closed in 119/153 (77.8%) patients at the time of presentation. The tumours measured 7.0–100.0 mm in size (average 33.7 mm, median 29.0 mm). All 153 cases demonstrated a predominantly osteolytic lesion. Marginal sclerosis was detected in 135/153 (88.2%) cases. Pathological fracture with dislocation occurred in 11/153 (7.2%) cases. Fluid–fluid levels were identified in 103/153 (67.3%) cases, indicative of intralesional haemorrhage and cyst formation. An aggressive behaviour with soft tissue involvement was observed in 13/153 (8.5%) tumours radiologically (figure 2).

(A–C) Radiologic images of a male in his early 20s with chondroblastoma located in the greater trochanter of the femur. (A) X-ray shows a well-defined radiolucent bone lesion. (B) CT shows an osteolytic lesion with a thin peripheral rim of sclerosis, cortical destruction and internal trabeculations. (C) T2-weighted MRI demonstrates the lesion is heterogeneous with a few fluid–fluid levels suggesting haemorrhage and cystic component. (D) T2-weighted (SPAIR T2W) MRI of a male in his early 20s with chondroblastoma involving the proximal humerus. The lesion is heterogeneous with obvious bone destruction and soft tissue mass.
Histological findings
Histologically, all CBs in our study exhibited classical pathological features at least focally. They were composed of sheets of uniform neoplastic mononuclear cells with interspersed osteoclast-like giant cells, eosinophilic chondroid matrix and various forms of calcification. The mononuclear cells are round or polygonal, sometimes exhibiting longitudinal nuclear grooves. Calcification surrounding single cells gives the characteristic chicken-wire calcification configuration. In rare cases, psammomatous calcifications were observed, presented as concentrically laminated calcified structures. Mitoses could be found in most cases (0–4/2 mm2), and no atypical mitosis was observed. Cytologic atypia of various degree could be observed in some cases. Cellular atypia was estimated when mononuclear cells exhibit cytologic atypia compared with the nuclei of surrounding multinucleated giant cells, and the cellular atypia was always mild and moderate.
In our cohort, aneurysmal bone cyst-like change was noted in 63.6% (117/184) cases, and chicken-wire calcification was observed in 26.1% (48/184) cases. Necrosis was present in 43.5% (80/184) cases, which is often composed of ghost cells lacking inflammation background. Microscopically, 4.9% (9/184) cases had cortical destruction and soft tissue infiltration and 2.7% (5/184) cases showed lymphovascular invasion, which indicate an aggressive behaviour morphologically. The histological features were summarised in figure 3A–F.

{kind=link}
{kind=link}
{kind=link}
Histological features (A–F), malignant transformation (G–J) and immunohistochemistry of H3F3 K36M (K–M) of chondroblastoma. (A) Sheets of uniform mononuclear cells embedded in an eosinophilic chondroid matrix (left) and pericellular ‘chicken-wire’ calcification (right). (B) Psammomatous calcifications were presented as concentrically laminated calcified structures in rare cases. (C) Cellular atypia and mitotic figures (arrows). (D) Bland necrosis without inflammation background. (E) Lymphovascular invasion. (F) Cortical destruction and soft tissue involvement. (G) Core needle biopsy of the recurrent lesion revealed a high-grade spindle cell sarcoma. (H) Inset of an MRI showed tumour recurrence 175 months after initial curettage. (I) Higher magnification field showed obvious cytologic atypia. (J) The tumour cells were positive for H3F3 K36M immunostaining. Immunohistochemistry for H3F3 K36M demonstrated diffuse and strong nuclear positivity in an non-decalcified (K) and an EDTA decalcified (M) CB sample, while the staining was patchy and weak in a HCl decalcified CB sample (L). Note that the immunoexpression is restricted to the mononuclear cells, but not the osteoclast-like giant cells or the matrix. HCL, hydrochloric acid.
In addition, one CB developed malignant transformation in our cohort, namely secondary malignant CB (figure 3G–J). A male patient in his late 20s with a CB arising in the distal femur underwent curettage at an outside institution. The patient received no radiation therapy and remained asymptomatic until he developed local pain 180 months after this surgery. Radiological examination showed an aggressive mass arising in the previous surgery site. Core needle biopsy revealed a high-grade spindle cell sarcoma with a strong and diffuse positive nuclear immunoreaction for H3F3 K36M. Mitoses were frequently observed. An H3F3B p.K36M (AAG to ATG) mutation was further confirmed by DNA sanger sequencing. En bloc resection with prosthetic replacement was performed in local hospital, and was finally diagnosed as malignant transformation of CB to high-grade osteosarcoma.
Immunohistochemical findings
IHC was performed on full tissue sections of 185 CB specimens from 157 patients. IHC of H3F3 K36M was positive in all 136 (100%) non-decalcified CB samples, all 18 (100%) EDTA decalcified and 27/31 (87.1%) HCl decalcified CB samples. Of the 31 HCl decalcified samples, 28 cases (including 3 immuno-negative samples) have concurrent non-decalcified specimens from the same patients, which were all positive. The immunoreactivity in non-decalcified and EDTA decalcified samples revealed diffuse and strong nuclear staining. Meanwhile, the immunoreactivity in HCl decalcified samples was always focal, weak to moderate, in a ‘mosaic’ type (figure 3K–M). These results further supported that EDTA is a better decalcifying agent than HCl to keep antigen activity.
In addition, we analysed 670 other primary bone or joint tumours by IHC, including those may enter the pathological differential diagnosis of CB, especially giant cell-rich bone lesions and cartilaginous tumours. All of these tumours showed negative immunoreaction with H3F3 K36M (table 4).
Immunohistochemistry result for H3F3 K36M mutant antibody in 185 chondroblastomas and 670 other primary bone lesions
Discussion
CB is a rare primary cartilaginous tumour representing less than 1% of all primary bone tumours. Much remains to be studied for its clinicopathological features. Our series showed a strong male predominance, with a male: female ratio of 2.8:1. The result is consistent with previous publications, in which the male: female ratio was reported to be 1.56–3.48:1.16 17 According to the shape of the bones, the most commonly involved bones were long bones (196/307, 63.8%), followed by short bones (68/307, 22.1%), sesamoid bones (25/307, 8.1%) and flat bones and irregular bones (18/307,5.9%). The patients was significantly younger in the long bone group at a cut-off value of 25. Our findings help to support the prior hypothesis that the involvement of non-long bones was more often observed in elderly individuals and the site distribution of CB in older patients are more variable.18–23 Surgical management has remained the mainstay of treatment for CB. Meticulous curettage followed by augmentation with bone graft or cement could provide favourable outcome for most patients. A small number of patients with complex conditions need radical surgery, en bloc resection or even amputation. Radiation therapy should not be employed for the ordinary CB.
Radiologically, most CB in our cohort were osteolytic lesions, and a peripheral rim of sclerosis was detected in 135/153 (88.2%) cases. It was recorded as marginal sclerosis when imaging showed the margin in the medullary cavity was high density or signal similar to cortical bone. Note that the thin cortex caused by lytic bone destruction are not real marginal sclerosis and were excluded in this study. Furthermore, all of those arising in long bones with available radiological images were epiphysial or apophyseal in origin. CB is a rare primary bone neoplasm usually involving skeletally immature patients. However, the status of adjacent physis was open in only a small segment (34/153, 22.2%) of the patients at the time of diagnosis in our cohort.
Though CB was classified as a benign neoplasm in the fifth edition of the WHO classification,9 its biological behaviour has been controversial. In our cohort, one patient developed presumed lung metastasis, and another patient experienced malignant transformation. Cortical destruction and infiltration of soft tissue were observed in 4.9% (9/184) cases microscopically and 8.5% (13/153) cases radiologically. Local recurrence after treatment has been reported ranging from 10% to 36%.24–26 Metastases and malignant CB has been documented in previous literature.4 5 27–30 All these findings question the notion that CB is a uniformly benign neoplasm. Histological features indicating malignant potential include cytologic atypia, high mitotic rate (>5/10 HPF), atypical mitosis, surrounding soft tissues involvement and lymphovascular invasion as reported.5 31 As necrosis is not uncommon in CB especially in specimens with preoperative biopsy, it could not be regarded as a clue for aggressiveness generally. However, we have reservations about the diagnostic nomenclature of ‘malignant CB’. In our experience, curettage and en bloc resections provide favourable outcome for CB patients, including those with atypical/ aggressive histological and/or imaging features. No patient died of CB or underwent amputation in the current study, only one patient developed unfavourable outcome with possible lung metastasis. Local recurrence always occurred within 2 years following initial surgery, probably due to incomplete operation and residual tumour. In addition, the diagnoses of ‘malignant CB’ in the literature were nearly always retrospective following unfavourable outcome. These metastases generally have an indolent course without any significant effect on disease specific mortality. Consistent with the findings of Konishi et al, we believe that there are no reliable histological criteria that predict the risk of local recurrence or metastases, including cytologic atypia and mitotic rate. These are not the definite diagnostic criteria for malignant CB. This maybe also the reason why it was reclassified as a benign neoplasm in the fifth edition of the WHO classification. Only CB with high-grade transformation into sarcoma is true malignant tumour. We proposed ‘CB with uncertain malignant potential’ to describe low-risk neoplasms to bridge the gap between benign and malignant as inspired by the classification of thyroid tumours.32–34 . They include neoplasms that have been reported to give rise to metastases but the incidence of spread is extremely low. Rather than classify them as malignant CB, the designation is intended to reduce the risk of overtreatment.32 33 These include CBs with atypical/aggressive histological and/or imaging features. More researches with greater number of cases are needed to elucidate the biological behaviour of CB. One limitation of our study is lacking longtime follow-up information for most patients.
All 3 cases with psammomatous calcification showed positive immunoreactivity for H3F3 K36M, which is different from the previous report that CB with psammomatous calcification were negative for H3F3 K36M and may harbour a different genetic event.19 Therefore, we propose that psammomatous calcifications in CBs have no special genetic significance.
We report here an extremely rare case of CB with a high-grade sarcoma transformation 180 months after the initial curettage, which was found to harbour H3F3 K36M mutation by both IHC and sanger sequencing. Spontaneous malignant transformation of conventional CB without radiation therapy is extremely rare.6–8 35
Approximately 70%–95% of CB were reported to harbour a p.K36M mutation.10–14 In our cohort, IHC of H3F3 K36M was positive in all non-decalcified and EDTA decalcified CB samples. Absent staining for H3F3 K36M in CB is probably false-negative immunoreaction caused by destructive sample decalcification and fixation, nearly all CB harbour an H3F3 K36M mutation. Other than CB, H3F3 K36M mutation was reported to be found in 1/75 conventional chondrosarcoma and 1/15 clear cell chondrosarcoma.10 In our series, none of the 670 non-CB bone tumours showed immunoreaction with H3F3 K36M, including 24 chondrosarcomas and 24 clear cell chondrosarcomas. According to Catalogue of Somatic Mutations in Cancer (COSMIC) database (http://cancer.sanger.ac.uk/cosmic), CB is the only neoplasm harbouring H3F3 K36M mutation in over 1 million tumours.36 The mutation-specific antibody H3F3 K36M is actually 100% specific for CB. Positive immunostaining restricted to the nuclei of the mononuclear cells showed that true neoplastic cells in CB were the mononuclear cells, not the osteoclast-like giant cells. Compared with DNA sequencing, immunohistochemical staining to detect the p.K36M mutation in the H3F3A or the H3F3B genes is a high-performance diagnostic tool for routine practice, as immunoreactivity in even a few cells is useful to confirm the diagnosis. Besides, DNA sequence remains expensive and time consuming. The high-grade sarcoma transformed from CB was also positive for H3F3 K36M antibody, which indicate that this antibody is not available for distinguishing malignant CB from its conventional counterparts. However, it is a valuable immunomarker to determine the origination of the transformation.
In summary, we have described the epidemiological and clinicopathological features of CB and shared the Chinese experience with a large cohort of 307 patients. The H3F3 K36M mutant antibody is a high-performance diagnostic tool, with 100% specificity for CBs, 100% sensitivity in non-decalcified and EDTA decalcified samples, and 87.1% sensitivity in HCl decalcified samples. Diagnosis of CB, especially assessment of the aggressiveness in individuals, should base on a combination of clinical, morphological and radiological features. To our knowledge, this is by far the largest single centre study describing the clinicopathological characteristics and IHC of H3F3 K36M of CB.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Data availability statement
The data presented in this study are available on request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee of Shanghai Sixth People’s HospitalApproval No:2018-KY-024(K). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank Jingyi Guo for her assistance with the statistical analysis of the data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Vikram Deshpande.
Twitter @power3719zqq
Contributors HZ contributed to the research study design. ZL supervised the project and revised the manuscript. ZL accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. QZ wrote the manuscript. JT, YL, JH performed data analysis and statistical analysis. DH, JZ and TJ collated the data. All authors critically reviewed and approved the final version of the manuscript.
Funding This research was funded by National Nature Science Foundation of China (Grant No. 81972500), Grant from Innovation Program of STCSM (Science and Technology Commission of Shanghai Municipality) (Grant No. 20Z11900304) and Clinical research funds from Shanghai Sixth People's Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (Grant No. ynlc201727).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.