Article Text

Abstract
Traditionally, immunohistochemistry (IHC) is used by pathologists to localise specific proteins or peptides in tissue slides. In the era of personalised medicine, however, molecular tissue analysis becomes indispensable for correct diagnosis, prognosis and therapeutic decision, not only on the DNA or mRNA level but also on the protein level. Combining molecular information with imaging presents many advantages. Therefore, matrix-assisted laser desorption/ionisation imaging mass spectrometry (MALDI IMS) is a promising technique to be added to the armamentarium of the pathologist. Here, we focus on the workflow, advantages and drawbacks of both MALDI IMS and IHC. We also briefly discuss a few other protein imaging modalities and give examples of applications.
- proteomics
- MALDI IMS
- mass spectrometry
- pathology
Statistics from Altmetric.com
Introduction
The discipline of histopathology has a long history.1 Technical improvements have led us from macroscopy over microscopy into molecular analysis. The use of microscopy images for clinical diagnosis lies at the core of the pathologist’s profession. Therefore, the pathologist is likely the best-placed medical professional for integrating molecular findings with information from detailed microscopic images.2
Over the last years, pathologists have become familiar with molecular techniques for DNA and mRNA analysis from tissue. However, measurement of protein alterations potentially better predicts functional consequences (and thus diagnosis and prognosis) than DNA alterations, because proteins themselves execute biological processes.3 Recently, many techniques have been developed for more detailed molecular protein analysis. Especially, matrix-assisted laser desorption/ionisation imaging mass spectrometry (MALDI IMS) emerges as a powerful tool. Virtually no diagnostic pathology laboratories have yet embraced MALDI IMS for day-to-day practice, though this is likely to change in the near future.
This review aims to introduce clinical pathologists to MALDI IMS. In order to outline the advantages of the technique, a comparison with immunohistochemistry (IHC) is made. The workflow of both techniques is summarised, advantages and disadvantages are compared and applications are discussed.
Immunohistochemistry
Principle and workflow
The essence of IHC is to make specific proteins or peptides visible under the microscope by means of antigen–antibody recognition by a specific immunoglobulin or primary antibody. IHC is mostly performed on slides cut from formalin-fixed, paraffin-embedded (FFPE) tissue, on slides generally around 2–5 µm thick that are first deparaffinised, washed with xylene and rehydrated through graded ethanol series (100%, 96% and 70%) before being subjected to antigen retrieval and application of antibodies. Heat-induced or enzyme-based antigen retrieval is necessary on FFPE tissue to make the epitopes ready for recognition by the primary antibody.4 The primary antibody is either monoclonal (generated via hybridoma technology)5 or polyclonal. Monoclonal antibodies have better specificity, while polyclonal antibodies tend to be more sensitive but less specific and give more background staining. The antigen–immunoglobulin interaction is visualised by addition of a conjugate at the primary antibody (direct IHC) or the secondary antibody (indirect IHC). In IHC, this conjugate is an enzyme, usually horseradish peroxidase or alkaline phosphatase. The addition of a chromogenic substrate results in a coloured precipitate. Different secondary antibody detection techniques have been developed over the years, such as the avidin–biotin–peroxidase complex, the labelled streptavidin–biotin complex and polymer-based detection systems.4 Polymer-based detection systems allow for good visibility and are now widely used in routine diagnostics. Automatisation techniques enable high throughput for diagnostic use,6 using robotisation for pipetting reagents on slides. The workflow of an IHC experiment, including tissue preparation, is outlined in figure 1.
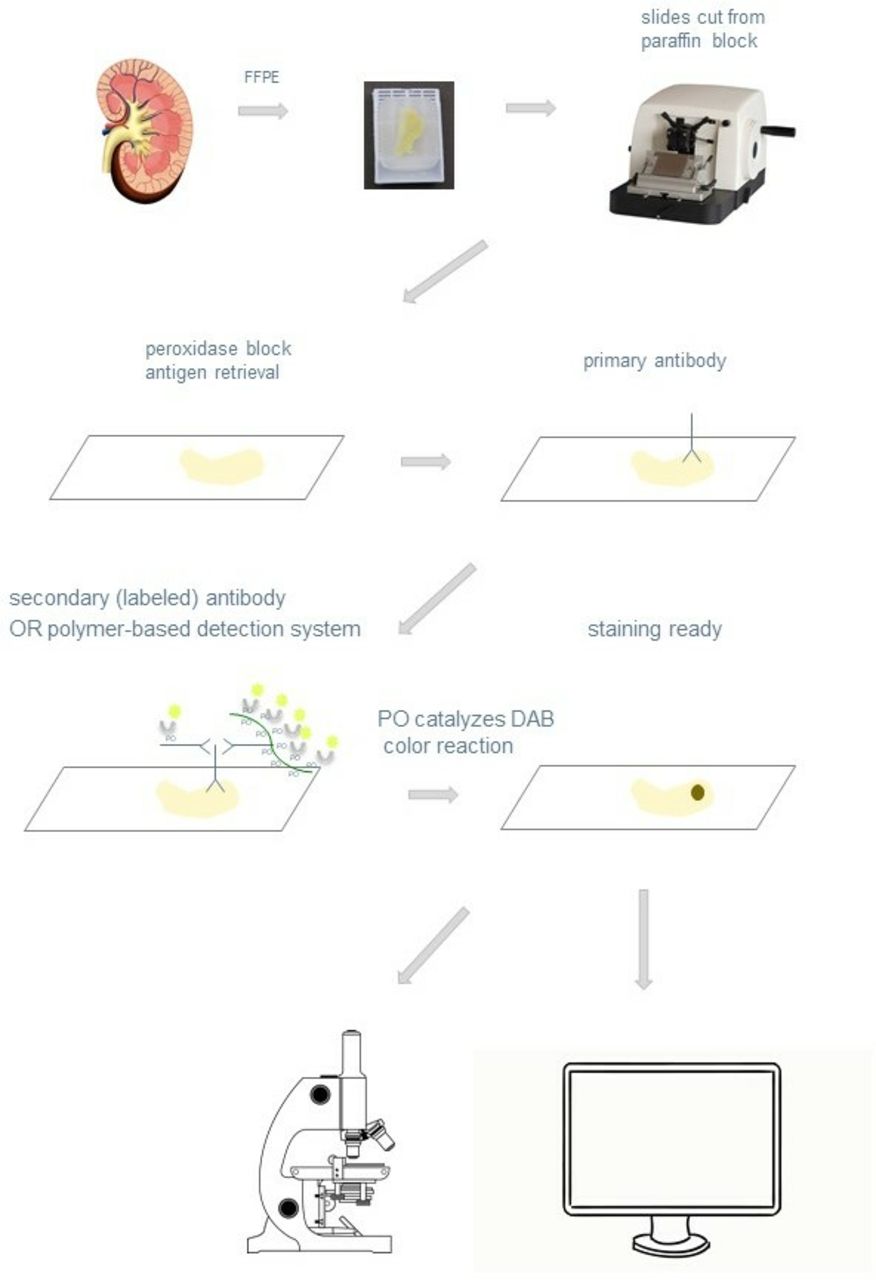
Workflow of immunohistochemistry on FFPE sample: the tissue is FFPE. Tissue sections are cut on a microtome and put on a slide, which is then deparaffinised and rehydrated. After peroxidase block and antigen retrieval (typically performed by boiling or microwaving the tissue in a buffer), the primary antibody is added to the slide. Then, the secondary antibody or polymer-based secondary antibody system is added. A PO moiety is present on this secondary antibody or moiety. This permits the DAB horse radish peroxidase substrate to be oxidised by the PO and changed into a brown colour on the tissue slide. The brown colour thus indicates the place of binding of the primary antibody with the targeted (protein) antigen. The slide is then interpreted by the human eye under the microscope or analysed through the computer after digital slide scanning (picture of FFPE block: Leica, picture of microtome: chinamedevice.com). DAB, 3,3-diaminobenzidine; FFPE, formalin-fixed, paraffin-embedded; PO, peroxidase.
IHC can be performed on cytology specimens, provided adequate tissue preparation is used,7 and on frozen sections.4 8
In immunofluorescence (IF),9 mostly performed on frozen sections, the conjugate consists of a fluorophore instead of an enzyme.
Some applications and future perspectives of IHC
IHC on FFPE is widely used in the pathology laboratory. At the Antwerp University Hospital, on average, two immunostains are performed per case, with a wide variability from 0 to more than 20 stains per diagnostic case.
IHC helps to subtype tumours, or visualises specific structures in the tissue, enabling the pathologist to establish a specific diagnosis. IF studies on skin or kidney tissue are typically used to visualise immunoglobulin or complement deposits.9
However, in the era of precision medicine, pathologists are increasingly involved in the evaluation of predictive factors for treatment, especially in the oncology field. Not only rendering a specific diagnosis is thus requested but also also the determination of certain prognostic and predictive factors. Examples include the determination of oestrogen and progesterone receptor status in breast carcinoma,10 the use of ALK staining for screening for ALK translocation in lung carcinoma11 and the determination of BRAF V600E mutation status in melanoma.12 Whereas conventional diagnostic decision-making usually includes more contextual clues, these assays guide treatment in a more binomial (yes/no) manner. This obviates the need for stringent quality control measures and validated scoring schemes for predictive immunohistochemical tests. An example of a scoring system is the Allred score for quantification of hormonal receptors in breast cancer.13 14
In the very nearby future, variability in human interpretation might benefit considerably from digital image quantification performed on scanned slides.15 In 2017, the FDA approved marketing of first whole slide imaging system for digital pathology.
In the field of IF, exploiting physical characteristics have led to the advent of a series of techniques that have improved spatial resolution by limiting diffraction, such as confocal scanning laser microscopy or super-resolution microscopy techniques, such as structured illumination microscopy, stimulated emission depletion microscopy, near-field scanning optical microscopy, saturated structured illumination microscopy, photoactivation localization microscopy and light-sheet microscopy, just to mention a few.16 17 These techniques are extremely popular for scientific research and are highly suited for digital quantification, but are currently not often used for day-to-day practice.
Matrix-assisted laser desorption/ionisation imaging mass spectrometry
Principle and workflow
Mass spectrometry (MS) encompasses a whole set of techniques to analyse different molecules, including, but not limited to, proteins and peptides, based on the molecular mass. MALDI IMS is one of these MS techniques, that additionally boasts the advantage of generating images.18 The workflow of a MALDI IMS experiment is outlined in figure 2.

{kind=link}
{kind=link}
Workflow of MALDI IMS: the tissue is FFPE or frozen. Tissue sections around 5–10 µm thick are cut. Preparation steps differ, depending on the tissue used (FFPE: deparaffinization, washing with xylene to rewax, rehydration, antigen retrieval, trypsin solution and enzyme application; fresh frozen tissue: ethanol washing±trypsin application, depending on the molecular weight of the protein). The treated tissue is put on a conductive, transparent material, typically, a glass slide coated with ITO. A suitable matrix for desorption and ionization is applied onto the slide. For many points/pixels on the tissue, a mass spectrum is generated based on mass-to-charge ratio, in a time-of flight mass spectrometer device. An image can be constructed for each peak length (peptide) representing the relative abundance of the peptide on each pixel. FFPE, formalin-fixed, paraffin-embedded; ITO, indium–tin oxide; MALDI IMS, matrix-assisted laser desorption/ionisation imaging mass spectrometry.
Preparation of a sample requires a tissue section around 5–10 µm thick. Preparation steps differ, depending on the tissue used, FFPE or frozen sections. FFPE tissue sections have to undergo deparaffinization and washing with xylene in order to rewax the tissue. Hereafter, rehydration through graded ethanol series (100%, 96% and 70%) is needed. Antigen retrieval can be either enzymatic, whereby proteins are cleaved into peptides, or heat mediated, whereby proteins undergo denaturation. These step are similar to the intial steps needed for preparation of FFPE tissue for IHC. Then, trypsin solution is applied with a spraying system. Tissue is digested during 1.5 hours at 37°C under 95% humidity. Enzyme application is a crucial preparation step for FFPE as different approaches can be used (different buffers, different concentrations of enzyme required, different digestion times and temperatures) in order to minimise the time and effort needed and maximise the spatial information.19–22
For fresh-frozen (FF) tissues, the preparation step consists of ethanol washing for direct profiling of protein with a mass below ±25 kDa. An additional preparation step for high-molecular-weight proteins (>±25 kDa) is trypsin application, since these proteins are not easily detected in matrix-assisted laser desorption/ionisation (MALDI) analysis of FF tissues due to their poor ionisation efficiency in this mass range.19 23
The tissue is then placed on a target. In the next step, the tissue section has to be coated with a matrix and air-dried. The method of application of the matrix also needs to be optimised, finding the balance between sufficient extraction of the analytes and avoiding lateral diffusion, which is detrimental for the resolution of the obtained images. Different matrices can be used for different types of analytes. The background signal can be quite high, limiting sensitivity of detection for some small molecules.
Then the sample is introduced into the mass spectrometer. During the ionisation process, a laser beam irradiates the matrix. Laser energy is absorbed, causing the transition of the solid matrix and the embedded analytes into a gaseous phase in which the molecules acquire a charge. MALDI is typically coupled to a time-of-flight (TOF) mass analyser. The ionised molecules are accelerated in a fixed electric field. Mass to charge ratio (m/z) is derived by determination of the time the ions travel through the fixed length of a flight tube. Ions with a lower m/z ratio will have a higher speed and reach the detector faster than molecules with a larger m/z. After calibration, a plot of m/z ratio (x-axis) and intensity (ion counts, y-axis) is achieved. This plot is the MS spectrum. The mass range in a normal MALDI-TOF instrument is in theory not limited, though usually in MALDI IMS it amounts to 30 kDa for intact protein analysis in FF sections. For peptides obtained from FFPE section after digestion, the mass range is 500–3200 m/z.20 The mass spectra are recorded with their two-dimensional coordinates on the tissue slide and then are processed, and images with localization of the analysed molecules are reconstructed. MALDI is a so-called ‘soft’ ionisation process because the matrix is the actual energy absorber instead of the tissue itself, minimising the protein fragmentation and/or destruction. For a more detailed discussion of technical aspects, we refer to the literature.24–28
For alternative imaging MS techniques such as desorption electrospray ionisation (DESI),29 MALDI Fourier-transform ion cyclotron resonance MS imaging,30 laser ablation electrospray ionisation31 32 and electrospray-assisted desorption/ionisation,33 we equally refer to the literature.
Some applications and future perspectives of MALDI IMS
In the oncology field, publications have highlighted applications of MALDI IMS in lung cancer, breast cancer, brain tumours, gastrointestinal tract cancer, urogenital cancer, and head and neck cancer, among others.34–37 This technique has been experimentally applied for the detection of malignant tumour margins, tumour typing, grading37 and determination of cancer heterogeneity.21
Most papers are in the research phase, though some include potential applications in diagnostic decision-making, for example, for determination of primary carcinoma type in peritoneal or pleural fluid washes.38
Digital PCR (dPCR) with subsequent MALDI IMS has also been investigated. Performing proteomic and genetic analyses on the same tissue section is an attractive alternative when low amounts of tissue are available. Kazdal et al demonstrated MALDI-IMS did not deteriorate the genetic information for dPCR analysis.20
Outside of the oncology field, applications are scarcer though still promising. An example from the pathology lab is the use of a highly sensitive and cost-effective MS-based test system for the detection of human papillomaviruses in FFPE tissue sections. This MALDI IMS method is suitable for detection of both high-isk and low-risk human papilloma virus subtypes.39
Advantages and disadvantages of MALDI IMS compared with IHC
Both MALDI IMS and IHC are techniques to visualise proteins or peptides in the tissue, with preservation of histology. Therefore, there are similarities but also important differences.
MALDI IMS allows for an untargeted investigation of molecules in a section, enabling an unbiased analysis, since no antibodies are needed for detection. In IHC, often diagnostic inconsistencies result from variable purity and different specificity of the antibody.40 An immunohistochemical signal is at best semiquantitative. IHC signal intensity follows a steep logistical (sigmoidal) chart in the function of epitope concentration. This means that a certain epitope concentration is needed for a staining intensity to be present altogether, followed by a small window where staining intensity is almost linearly correlated to epitope concentration. Nonetheless, this linearity is quickly maxed out at higher antigen concentrations, inhibiting further possible quantification.41 In MALDI IMS, absolute quantification is equally difficult, but because of other reasons. Strong signal variations resulting from non-uniform crystal formation, co-crystallisation issues of matrix and analyte across the substrate and the difficulty of introducing standards in the tissue. Therefore, MALDI IMS is often considered as, at best, semiquantitative in the sense that relative differences in intensities of different analytes in the same pixel or region are taken into account. Nevertheless, several technical solutions do exist to collect absolute quantitative data from individual compounds in MALDI IMS, although these are, at the moment difficult to implement on a routine basis.42
In MALDI IMS, many different peptides can be analysed and located in a single assay at no additional cost in analysis time, labels or biological material.43 IHC is in comparison a rather low throughput technique, because, typically, one antigen is assayed on one slide at a time, though double or even triple staining for two and three antigens, respectively, on one slide has become more common.44 45 Still, performing a panel of IHC stains is at the cost of needing multiple slides using a considerable amount of tissue.
Many of the limitations of IHC extend to IF techniques, but some differences exist. IF is typically performed on frozen sections. As no formaldehyde is used for IHC or IF on frozen sections, there is no crosslinking of proteins and protein configuration is preserved. No antigen retrieval techniques are therefore applied and conduction time is fast.46 IF boasts an often higher sensitivity and specificity.47 However, morphology is hindered by freezing artefacts, and slides need to be stored in refrigerated conditions instead of room temperature. Additionally, an immunofluorescent microscope is needed for reading and interpretation of the slides, and this is sometimes seen as a drawback for routine practice in comparison with enzymatic visualisation techniques that make the immune reaction visible under a simple light microscope. However, multiplexing is easier to achieve in IF by using multiple antibodies, each tagged by a different fluorophore (different wavelength) or even by multispectral imaging.15
Both FF and FFPE samples can be assayed with MALDI,19 although analysis of FFPE needs more preparation steps and is generally more complex and less reproducible.48 The advantage of FFPE tissues is that they are routinely available from pathology archives spanning many years, which make them an ideal resource for retrospective biomarker discovery.19
In addition to the identity (through their molecular mass) of molecules, information on spatial distribution is obtained directly by scanning the laser in raster on the surface of the tissue. By recording both the spectra and the location from where the spectra were obtained, images can be created showing the distribution of individual molecules in the tissue. Relative abundances of a large number of biomolecules (eg, peptides, proteins and metabolites) can be provided directly in situ from a tissue specimen.
MALDI IMS is mostly non-destructive, this gives the possibility to use the tissue slide afterwards for conventional histochemical or immunohistochemical imaging or other molecular analyses (such as PCR).20 Even though MALDI IMS provides a high level of molecular information, a good spatial resolution is generally at the cost of high data acquisition times and sensitivity, although recently there has been progress on the matter.49 The combination of the two techniques, microscopy and MALDI-IMS, results in an image with good spatial resolution and high molecular specificity.50
Both MALDI IMS and digitally scanned IHC slides are amenable to machine learning.15 51–53
MS instruments are not yet in the standard equipment of the average pathology laboratory. The instrument time, though declining, can be long and instruments are expensive. However, recent studies performed with high-speed mass spectrometers demonstrate a total measurement time of 1.5 hours per tissue at a 50 µm pixel size for tissue sections of ±5 µm thickness.21 Recent years have seen a breakthrough in the use of cheaper ‘desktop’ mass spectrometers for microbiology, indicating that these systems are increasingly around in hospitals and medical laboratories.54
Considering technical notes, software and an overview of commercial instruments, information can be found at the website of the MS Imaging Society (https://ms-imaging.org).
For a summary of characteristics of MALDI IMS compared with IHC, we refer to table 1.
Comparison of properties of immunohistochemistry and MALDI imaging for protein analysis
Example of a candidate disease to evaluate by MALDI IMS: amyloidosis
Amyloidosis is a group of disorders characterised by abnormal protein folding. The conformational change that occurs in susceptible proteins leads to the formation of an insoluble beta-pleated sheet secondary structure.55 This misfolding causes extracellular accumulation of pathological amyloid protein. Because these proteins are abundant and concentrated in the depositions, amyloidosis is a good candidate for analysis by MALDI IMS as signal to noise ratio is expected to be high.
Furthermore, from a clinical perspective, amyloidosis represents a disease in which an improvement in diagnostic accuracy has huge clinical consequences, that is, better treatment options and thus prognosis. Improving the knowledge on newer diagnostic techniques in a broad audience of pathologists might also set the scene for clinical implementation of MALDI IMS.
The most common forms of amyloidosis are immunoglobulin light-chain (AL) amyloidosis and amyloid A (AA) amyloidosis. The latter is a secondary form in various chronic inflammatory diseases. Hereditary amyloidosis is a third group.56
Currently, conventional microscopy and IHC are typically used to diagnose amyloidosis. Amyloid deposits stained by Congo Red show apple-green birefringence under polarised light. IHC studies are helpful in subtyping, using a more or less extensive panel of stains.55 57 However, laboratories typically do not have antibodies available for detection of all amyloid subtypes.55 MS in general is a very valuable and straightforward alternative as it does not require target-specific antibodies and has the ability to identify multiple different peptides at once, including new and unknown ones.57
Interestingly, MS can even be used upfront as it detects subtle amyloid deposition in an earlier stage than Congo red staining.57 The MS diagnosis of amyloidosis is based on detection of serum amyloid P component, apolipoprotein E, vitronectin and perlecan since all of these proteins are linked to both AL and AA amyloidoses.56–59 Although mostly tissue extraction and liquid chromatography (LC)-based MS techniques have been used for analysis of amyloid,56 MALDI IMS might be very suitable as well. An important advantage of MALDI IMS is the preservation of spatial information since one does not need to make a tissue lysate as in LC-based MS.60
Other techniques
A technique called mass spectrometry immunohistochemistry (MSIHC) combines IHC with MS.61–63
Instead of fluorophores or chromogens, metal-labelled antibodies are used for detection of peptides of interest. The strategy employs antibodies that are labelled with elemental mass tags, such as isotopically pure lanthanides not typically found in biological specimens, rather than with typical fluorophores or chromogens. The metal-labelled antibodies are then detected in tissue using lasers or ion beams to liberate the tags for subsequent MS detection. Typically, magnetic sector instruments are time-of flight (TOF) instruments that are dedicated just for this type of analysis. In a multiplex panel, the metal labels are selected so as not to overlap. In theory, this means up to 100 antibodies (for respective antigens) can be detected at once on a single slide.61
In the TagMass method, a specifically designed antibody against a target antigen64 65 is linked to a laser-cleavable peptide64–68 with known sequence.64 65 An MS image of the tissue is generated. The sequence and the identity of the peptide are then determined by means of MS and are subsequently imaged on the surface of the tissue.65–67 In contrast to MSIHC, this type of analysis can be performed with fairly common MALDI IMS instruments.
Scanning mass cytometry (SMC) is another technique in which a form of laser ablation technique with spot sizes down to 1 mm is used to liberate tissue into a carrier gas. The ablated sample is then transported into argon plasma, ionised and thereafter detected by MS. All targets are scanned at once, while the full sample thickness is destroyed.61 62
Multiplexed ion-beam imaging (MIBI) is based on another MS technique than MALDI, namely, secondary ion mass spectrometry, in which the sample is scanned by an ion beam with a submicron spot size. A mass spectrometer then detects the released secondary ions.61 63
An alternative method is based on the combination of MALDI IMS with IHC, but without the need for the costly design and production of specific antibodies. Therefore, in situ tryptic digestion of the primary antibody against an antigen is imaged. This tryptic digestion is needed, due to the large masses of the primary native antibodies. Furthermore, it is also possible to separate the heavy chains from the light chains by means of reduction and alkylation. Instead of the application of a secondary antibody, a matrix layer is applied after digestion an overnight incubation for the desorption-ionisation of the digested fragments of the primary antibody. The principle consists of a direct comparison of the peptide mass fingerprint after in-gel tryptic digestion and the peptide mass fingerprint after antibody incubation, followed by tryptic digestion. A great advantage of this method is the compatibility with every polyclonal and monoclonal antibody for the detection of a specific antigen, whereas Tag Mass, SMC and MIBI need specific designs of antibody and labelling.65
All these techniques allow for extensive multiplexing and are considered a ‘next-generation’ approach to IHC.61 69 The most limiting factor of MSIHC is the cost,61 including design of antibodies and cost of instruments for analysis and imaging.
Vibrational spectroscopy is another group of innovative techniques that can detect molecular changes in tissue. Raman spectroscopy and Fourier transform infrared microspectroscopy are both vibrational imaging modalities. Here, imaging is based on physical characteristics of the interaction between light and matter providing data based on the molecular vibrations on the chemical bonds between atoms. Although the principle is not new, due to great advances in instruments, high-quality images can be produced. Just as for MALDI IMS, spectral histopathology is based on the detection of changes in biochemical composition, rather than on morphological features, and shows that tissue morphological features observed in classical pathology are accompanied by changes in the biochemical composition at the cellular level.70 71
Conclusion
Although MALDI IMS is often complex and requires investments in equipment, applications might be coming into the routine pathology laboratory relatively soon, probably linked with software for unbiased image analysis and deep learning.
There is evidently a great need for multiplex systems that have the ability to measure several proteins at once. Oncology might benefit from techniques where predictive biomarkers are quickly analysed in parallel. In the non-oncological field, the imaging and characterisation of amyloid in tissues by MALDI IMS are one promising example.
DNA markers have made their way into our laboratories over the past few decades, first detected by PCR, then by Sanger sequencing and massive parallel sequencing (next-generation sequencing); it might just be about time for proteins to follow course.
References
Footnotes
Handling editor Tahir S Pillay.
Contributors DA designed the initial structure of the review. AM, BG, DA, VCAH and BG edited and reviewed the manuscript. GB and PP reviewed the manuscript. SK performed the MALDI experiment to generate a picture of a human kidney.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.